
Abstract
This Practice Guideline provides a summary of strong to moderate evidence that supports clinical recommendations for the use of self-management interventions for adults with chronic conditions. Two case studies, with decision-making algorithms, are presented to highlight how occupational therapy practitioners can apply the evidence to practice.
The prevalence and cost of chronic disease in the United States are experiencing rapid growth. Approximately 6 in 10 American adults have at least one chronic disease, such as heart disease, lung conditions, diabetes, or kidney disease, that lasts a year or more and limits functional daily activities (Centers for Disease Control and Prevention [CDC], 2020). Chronic disease often requires ongoing medical attention, raising annual health care costs. In 2016, chronic disease in the United States represented more than $1 trillion in direct health care expenditures (Waters & Graf, 2018). Several factors have contributed to the growth in the prevalence and cost of chronic disease, including the rising age of the population and disease-specific risk factors such as poor nutrition and sleep, tobacco use, lack of physical activity, and failure to attend annual health care visits. In effect, many adults with chronic disease experience disability (Hung et al., 2012).
Froehlich-Grobe et al. (2016, p. 600) noted that adults “living with both chronic diseases and disability are at a substantially increased risk for poor health status,” which takes a toll on not only their own engagement in meaningful daily activities (occupations), but that of their caregivers (i.e., family members and friends) as well. Researchers have found that family members who provide support to adults with chronic conditions report greater physical distress, lower life satisfaction, and greater limitations in daily activities compared with noncaregivers (Grossman & Webb, 2016; Institute of Medicine, 2012).
Although chronic diseases are among the most common and costly health problems, their functional implications may be mitigated through health management interventions that occupational therapy practitioners provide. Health management interventions focus on “developing, managing, and maintaining health and wellness routines, including self-management, with the goal of improving or maintaining health to support participation in other occupations” (American Occupational Therapy Association [AOTA], 2020b, p. 32) and are within the scope of occupational therapy practice. This Practice Guideline provides a summary of self-management interventions supported by current research to address commonly reported occupational challenges for community-dwelling adults with chronic conditions. Several descriptions of self-management guided the development of this Practice Guideline, including “the ability of the individual, in conjunction with family, community, and healthcare professionals, to manage symptoms, treatments, lifestyle changes, and psychosocial, cultural and spiritual consequences of health conditions” (Richard & Shea, 2011, p. 261); healthy lifestyle behaviors undertaken by individuals for optimal growth and development (Dickson et al., 2008); and preventive strategies performed to promote or maintain health (Dickson et al., 2008).
Occupational therapy practitioners have opportunities to favorably influence the trajectory of chronic disease and resulting disability, thereby maximizing the independence of adults and easing the burden on their caregivers (Liu et al., 2018). Occupational therapy is uniquely positioned to address self-management from a holistic perspective, taking into account a client’s intrinsic factors (cognitive, psychological, physical, sensory, emotional, and spiritual) and extrinsic influences (culture, social determinants of health, social support and capital, the built and natural environment, and policy) while considering the roles and activities in which the client participates.
The four systematic reviews (Kaldenberg et al., 2020; Kearney et al., 2021a, 2021b; Rouch et al., 2021; Smallfield et al., 2021) whose findings are reported in this Practice Guideline addressed four common, noncommunicable, chronic physical conditions that are modifiable through health behaviors: heart disease, chronic lung conditions, diabetes, and kidney disease (see the CDC [2021] list of most common chronic conditions). Cancer, stroke, arthritis, and Alzheimer’s disease were excluded because AOTA has published specific practice guidelines for those conditions (see Braveman & Hunter, 2017; Piersol & Jensen, 2017; Poole et al., 2017; Wolf & Nilsen, 2015). The practice guideline for adults with stroke (Wolf & Nilsen, 2015) did not address interventions for caregivers, so the review question on caregiver interventions includes caregivers of people with stroke.
Systematic Review Questions
This Practice Guideline is based on the following four questions: What is the evidence for the effectiveness of self-management interventions within the scope of occupational therapy practice to improve the performance of ADLs and sleep and rest among community-dwelling adults with chronic conditions (Smallfield et al., 2021)? What is the evidence for the effectiveness of self-management interventions within the scope of occupational therapy practice to improve the performance of IADLs among community-dwelling adults with chronic conditions (Kearney et al., 2021a, 2021b)? What is the evidence for the effectiveness of self-management interventions within the scope of occupational therapy practice to improve the performance of education, work, volunteering, leisure, and social participation among community-dwelling adults with chronic conditions (Kaldenberg et al., 2020)? What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people with chronic conditions to facilitate their ability to maintain participation in the caregiver role (Rouch et al., 2021)?
Goals of This Practice Guideline
Through this Practice Guideline, AOTA aims to help occupational therapy practitioners, as well as the people who manage, reimburse, or set policy regarding occupational therapy services, understand occupational therapy’s contribution in providing services to adults with chronic conditions. This guideline can also serve as a reference for health care professionals, health care facility managers, education professionals, education and health care regulators, third-party payers, managed care organizations, and those who conduct research to advance care of adults with chronic conditions.
This guideline was commissioned, edited, and endorsed by AOTA without external funding being sought or obtained. It was financially supported entirely by AOTA and was developed without any involvement of industry. AOTA supports systematic reviews on adults with chronic conditions as part of its Evidence-Based Practice (EBP) Project. AOTA’s EBP Project is based on the principle that the EBP of occupational therapy relies on the integration of information from three sources: (1) clinical experience and reasoning, (2) preferences of clients and their families, and (3) findings from the best available research.
All authors of the systematic reviews completed conflict-of-interest disclosures, with no conflicts noted. AOTA reviews practice guidelines every 5 years and updates them as needed to keep recommendations on each topic current according to criteria established by ECRI (2020). Guideline topics are evaluated for their currency by a multidisciplinary advisory group consisting of AOTA members, nonmember content experts, and external stakeholders. In addition, a preliminary search of the literature is conducted to determine whether an updated systematic review is warranted. The systematic review questions and search terms used for this Practice Guideline and the Practice Guideline itself were reviewed and revised on the basis of feedback from a group of content experts on adults with chronic conditions; this group included practitioners, researchers, educators, clients and consumer representatives, and policy experts. Reviewers who agreed to be identified are listed in the Acknowledgments section of this publication.
This Practice Guideline reports the findings from systematic reviews of published scientific research addressing focused topic-specific questions; interventions that did not emerge from the published literature or did not meet the inclusion criteria are not included. The occupational therapy practitioner makes the ultimate clinical judgment regarding the appropriateness of a given intervention considering a specific client’s or group’s circumstances, needs, and response to intervention; the practitioner’s own expertise; and the evidence available to support the intervention. The goal of the Practice Guideline is to inform practitioners about the state of the evidence and to help guide them in translating the evidence to practice. We provide examples of how this evidence can inform practice in the “Case Illustrations and Algorithms” section.
Clinical Recommendations for Occupational Therapy Interventions for Adults With Chronic Conditions
Clinical recommendations are the final phase of synthesis of systematic review findings. We graded the findings for each systematic review question in terms of how confident a practitioner can feel that using the interventions presented in the evidence will improve the outcomes of interest to their clients. The grade is based on the specificity of the intervention, number of studies supporting the intervention, levels of evidence of the studies, quality of the studies, and significance of the study findings. Interventions included in the clinical recommendations are specific to a population, and the articles that describe them provide sufficient detail to understand the intervention and the outcome of interest.
Describing the strength of clinical recommendations is an important part of communicating an intervention’s efficacy to practitioners and other users. The clinical recommendations for this practice guideline were evaluated and finalized by AOTA staff, the AOTA research methodologist, and systematic review and practice guideline authors. AOTA uses the grading methodology provided by the U.S. Preventive Services Task Force (2018) for clinical recommendations. The recommendations pertaining to each review question, along with the studies’ level of evidence and supporting details, are presented in Tables 1–4.
Clinical Recommendations and Supporting Evidence: Self-Management Interventions to Address ADLs and Sleep and Rest Among Community-Dwelling Adults With Chronic Conditions
Note. All studies had statistically significant positive outcomes related to the interventions discussed. ADLs = activities of daily living; COPD = chronic obstructive pulmonary disease; PSQI = Pittsburgh Sleep Quality Index.
Clinical Recommendations and Supporting Evidence: Self-Management Interventions to Address IADLs Among Community-Dwelling Adults With Chronic Conditions
Note. All studies had statistically significant positive outcomes related to the interventions discussed. BMI = body mass index; HbA1c = hemoglobin A1c; NR = not reported; SMBG = self-monitored blood glucose.
Clinical Recommendations and Supporting Evidence: Self-Management Interventions to Promote Education, Work, Volunteering, Leisure, and Social Participation Among Community-Dwelling Adults With Chronic Conditions
Note. All studies had statistically significant positive outcomes related to the interventions discussed.
Clinical Recommendations and Supporting Evidence: Interventions for Caregivers of People With Stroke to Maintain Their Participation in the Caregiver Role
Note. All studies had statistically significant positive outcomes related to the interventions discussed. CBS = Caregiver Burden Scale; CES–D = Center for Epidemiologic Studies Depression Scale; CSQ = Client Satisfaction Questionnaire; GHQ = General Health Questionnaire; GHQ–12 = Short General Health Questionnaire; GHQ–30 = General Health Questionnaire 30-item version; NR = not reported; PCS = Preparedness for Caregiving Scale; PSI = Problem-Solving Inventory; SF–36 = 36‐item Short Form Survey.
For the purposes of this Practice Guideline, we considered only findings indicating an A, B, or D grade, the grades that best support clinical decision making: A: There is strong evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. Strong evidence was found that the intervention improves important outcomes and that benefits substantially outweigh harms. B: There is moderate evidence that occupational therapy practitioners could routinely provide the intervention to eligible clients. There is high certainty that the net benefit is moderate, or there is moderate certainty that the net benefit is moderate to substantial. D: It is recommended that occupational therapy practitioners not provide the intervention to eligible clients. At least fair evidence was found that the intervention is ineffective or that harms outweigh benefits. In these reviews, we did not find grade D evidence.
These grades are reported in Tables 1–4 and designated with green, indicating should do if appropriate (A), or yellow, indicating consider doing if appropriate (B). We do not report the results of interventions that had low strength of evidence or insufficient research support to determine an A, B, or D grade. None of the studies included in these reviews reported adverse events or harms related to the interventions evaluated.
The complete findings from the systematic reviews can be found in the applicable Critically Appraised Topics (Kaldenberg et al., 2020; Kearney et al., 2021a, 2021b) and articles in the American Journal of Occupational Therapy (Rouch et al., 2021; Smallfield et al., 2021).
Translating Clinical Recommendations Into Practice
The purpose of clinical practice guidelines is to help practitioners translate pertinent research findings from systematic reviews into practice. When making decisions in practice, practitioners should integrate clinical recommendations based on the best available research, which are provided in this Practice Guideline, as well as their own clinical experience and reasoning and the preferences of clients and their families. Algorithms related to the clinical recommendations are provided to facilitate practitioners’ clinical decision making and are presented at the end of each case.
Clinical Reasoning Considerations
Very rarely will practitioners find an evidence-based intervention that perfectly fits their clinical setting and the client’s specific needs. Practitioners need to consider several questions as they evaluate the research and consider whether they can use an intervention, or adapt it in a well-reasoned way, to meet the client’s needs (Highfield et al., 2015): Exactly what intervention do I need to provide? What types of client outcomes am I looking for? Do the studies I’ve located provide enough detail on the intervention so that I know what to do and how to do it? How well do the conditions in which I will provide the intervention match those in the studies? What are the demographic characteristics (e.g., age, gender, diagnosis, comorbidities) of the participants in the research studies? In which setting (e.g., inpatient, home, community, school) did the studies take place? Do any contextual factors (e.g., resources, policies) that are different from those in the studies influence my ability to provide the intervention? How flexible is the intervention, and how much can I modify or adapt it? If my setting or client population differs from those of the studies, can I modify or adapt the intervention without changing its integrity? If I modify or adapt the intervention, what client characteristics (e.g., comorbidities) do I need to consider? Can I be proactive and plan how to modify or adapt the intervention before I start implementing it? Can I make minimal changes to the intervention, such as reordering the content of sessions, or does the need for substantial changes indicate I should select another intervention?
To modify or adapt evidence-based interventions to practice, practitioners must plan ahead and proactively think through the changes they need to make to fit the intervention to the client and practice setting. In addition, they must document how and why they altered the researched intervention so others in their setting know how to implement the intervention and why the changes were made. When practitioners adapt an intervention, it is no longer evidence based, but rather evidence informed. If extensive adaptations to the intervention are necessary, the intervention is probably not right for the client or setting. If the practitioner finds that the intervention does not suit the client, they should not use that intervention. Clinical interventions should be as similar as possible to interventions used in the research.
Case Illustrations and Algorithms
Two case studies are presented to demonstrate how practitioners can use the evidence from the systematic reviews to inform their practice. We developed the cases using the evidence for the effectiveness of self-management interventions to promote performance and participation in occupations among community-dwelling adults with chronic conditions. To support the clinical decision making in the cases and ensure they fully represent current practice for adults with chronic conditions, we also describe other important resources, including the practitioner’s expertise and the client’s values and preferences.
Algorithms based on the developed clinical recommendations were developed by the authors and AOTA staff to assist practitioners in identifying appropriate interventions for people with chronic conditions. Each algorithm includes decision points and actions for practitioners to take. When using algorithms to inform clinical decision making, it is important for practitioners to consider each potential intervention in relation to the client’s individual goals, interests, habits, routines, and environment. Practitioners should choose interventions that strongly align with or are supportive of these factors in the context of the client’s occupational profile.
Case Study 1: Salomé
Occupational Therapy Initial Evaluation and Findings
Using AOTA’s (2021b) Occupational Profile Template as a guide, Salomé’s occupational therapist conducted an initial evaluation, which revealed the following: Salomé is currently on 1 L of oxygen via nasal cannula. She has a home oxygen concentrator located in the living room with extended oxygen tubing that allows her to move around the apartment. Salomé normally wakes in the early morning when Jan returns home from work. She is often not able to get back to sleep. She reports that on average she sleeps 5 hr or less most nights. Salomé is no longer able to manage paid employment because of her chronic conditions and is on a fixed disability income. She used to work as a cashier at a local grocery store. Jan, who works overnight shifts in environmental services for a large office building, returns to the apartment in the early morning hours. She sleeps until about noon and leaves for work in the early evening. Salomé is not able to leave her apartment as much as she would like because of her low activity tolerance and need for portable oxygen. She reports that she wants someone to assist her when in the community, and Jan expresses discomfort with managing the portable oxygen because she is unfamiliar with it and fears running out of oxygen when they are away from home. Salomé enjoys reading the newspaper each morning while she drinks coffee, caring for her cat, talking to friends on the telephone, reading books and magazines from the library, and watching movies, both at home and in the theater. Because of Salomé’s COPD, she stopped smoking 5 yr ago; however, Jan continues to smoke outside the apartment.
Additional findings from the evaluation are provided in Table 5.
Assessment Findings for Salomé
Occupational Therapy Interventions
Salomé participated in nine scheduled occupational therapy sessions over 2 mo, including the initial evaluation and reevaluation at discharge. After the initial evaluation, the occupational therapist used the activity tolerance algorithm displayed in Figure 1 to develop a plan of care that used a multicomponent approach to enhance Salomé’s self-management of her multiple chronic conditions. This approach included client and caregiver education, health management, resource advocacy, and training in problem‐solving strategies. Goals included improved tolerance for activity within the apartment, sleep, health management, and participation in leisure and social activities. The sections that follow describe evidence-based interventions that could be implemented with Salomé by either an occupational therapist or an occupational therapy assistant.
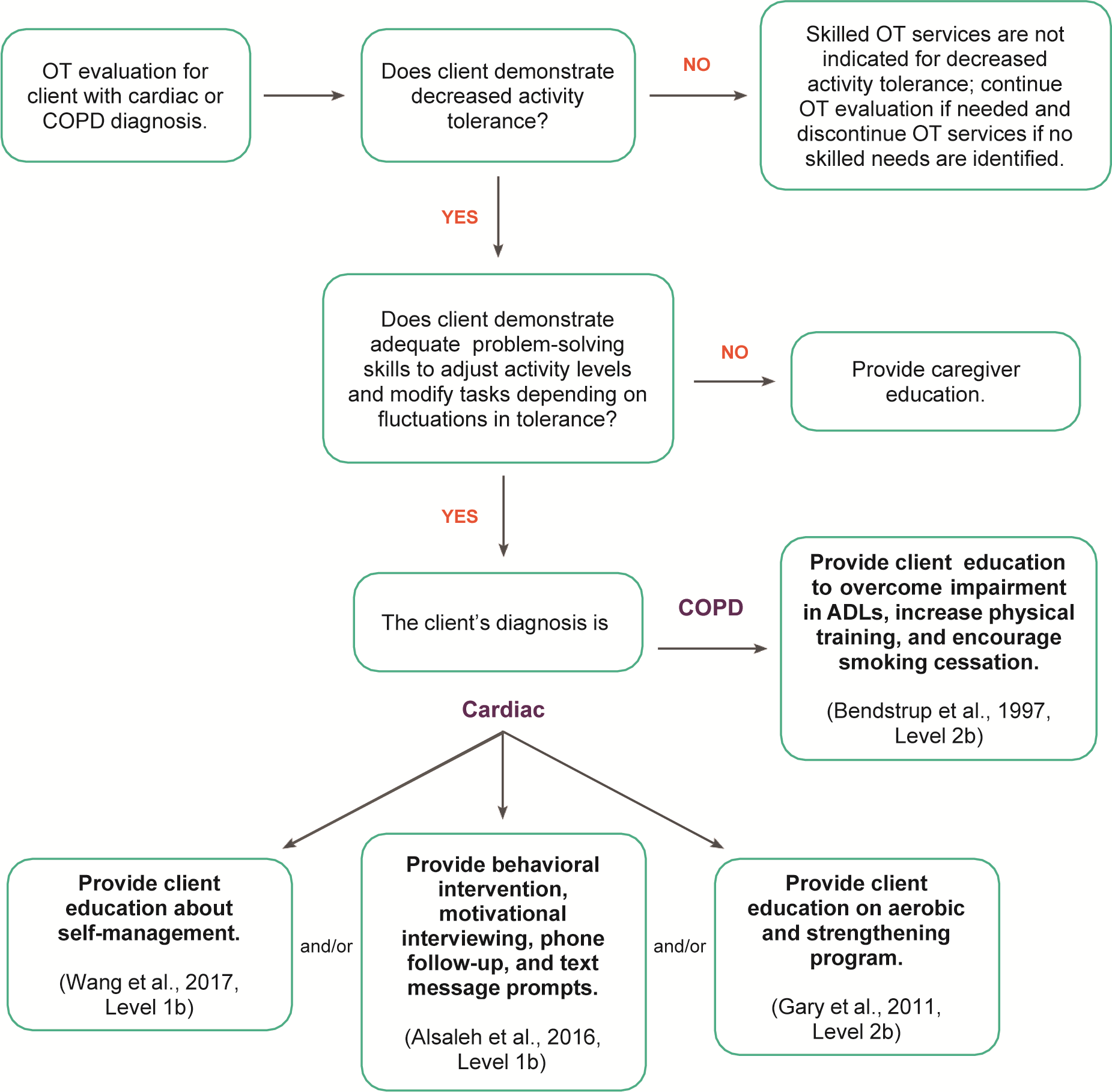
Decision-making algorithm for interventions to increase activity tolerance among clients with heart disease or chronic lung conditions.
Sleep and Health Management Intervention
Three sessions were focused on addressing sleep and enhancing Salomé’s activity tolerance during the day. The occupational therapy practitioner provided education regarding sleep hygiene and the benefits of a regular sleep routine (Kapella et al., 2011; Rybarczyk et al., 2001). Salomé determined that her poor sleep was in part attributable to waking early when Jan returned home. The practitioner discussed the option of sleeping in separate bedrooms to make it less likely that Salomé wakes when Jan returns home. They also discussed the option of Jan using night lights instead of room lights in the early morning hours. Additionally, the practitioner demonstrated a variety of mindfulness and relaxation techniques to Salomé, who provided return demonstration. Salomé selected one of the strategies to implement when she prepared for sleep and when she woke in the middle of the night.
The practitioner also discussed the benefits of a routine physical activity schedule to promote overall well-being. Together, they reviewed a seated aerobic and strengthening exercise program that Salomé could integrate into her daily routine (Bendstrup et al., 1997; Gary et al., 2011). Salomé provided return demonstration of the exercise routine. As they considered Salomé’s daily activities and existing performance patterns, they determined that she would first try the strategy of completing the exercises each day before reading the newspaper and drinking her coffee to integrate the exercise into her routine.
Individual Self-Management Intervention
For the next two sessions, Salomé continued to address her self-management skills (Wang et al., 2017). The practitioner introduced Salomé to keeping an activity diary to aid in tracking her sleep, exercise program, medication adherence, and activity tolerance. The activity diary also included space for reflection on her mood. Once Salomé was oriented to the diary, she participated in a laundry task while self-monitoring her tolerance for the activity. Afterward, she completed her first diary entry, which included reflection on her tolerance for the activity and her overall mood. Between therapy visits, the practitioner consulted with Salomé every other week over the phone during the 2 months of occupational therapy services to review the activity diary and adjust activity levels and time use as needed—for example, adjusting the time of day when Salomé completed her household tasks to best align with her energy level.
Psychoeducation and Problem-Solving Intervention
Two sessions centered on disease-specific education and problem-solving training with Salomé and Jan (Ågren et al., 2012; Toseland et al., 2004). The occupational therapy practitioner provided education on the functional limitations caused by Salomé’s multiple chronic conditions, and the three collaborated on developing a strategy of steps to use when Salomé faced challenges that prevented engagement in occupations. This strategy included writing down the problem, developing a list of potential solutions, selecting the option that is most suitable to try first, implementing the option, and evaluating its effectiveness. Salomé and Jan then applied this problem-solving strategy to several barriers to Salomé’s engagement in activities outside the apartment, including management of Salomé’s portable oxygen and low activity tolerance. After discussing potential solutions, the practitioner guided Salomé and Jan in practicing their selected option of using an oxygen cylinder shoulder bag during functional mobility from the apartment to their vehicle to enable them to plan participating in occasional community-based activities.
Discharge Summary
Salomé met her goals after completing 8 wk of home health occupational therapy services. Salomé reported that she increased her satisfaction with her sleep, which had resulted in more energy to participate in daytime activities, including her seated exercise program. She was also beginning to plan community-based activities with Jan on the weekends, which had improved their social relationship. They planned the activities together in advance to ensure that Salomé built in opportunities to take rest breaks when needed.
By discharge, Salomé and Jan had gone to the movie theater for an afternoon matinee and visited the public library to check out books Salomé could read at home. Salomé found the activity diary helpful for seeing the progress she had made in activity tolerance, and the telephone consultations between therapy visits kept her on track. Because Jan observed the effectiveness of the activity diary in improving Salomé’s activity tolerance, she decided to add it to her daily routine as a strategy to reduce her smoking.
Salomé’s scores on the Canadian Occupational Performance Measure improved from 3/10 to 7/10 for Performance and from 4/10 to 7/10 for Satisfaction (Law et al., 2019). Her Geriatric Depression Scale score improved 2 points to a score of 3, indicating no depressive symptoms (Yesavage et al., 1982–1983). Her global score on the Pittsburgh Sleep Quality Index improved from 19/21 to 10/21 (Buysse et al., 1989), indicating improved sleep quality. Salomé reported she was now consistently getting 6.5 hr of uninterrupted sleep each night and felt refreshed when she woke up. She reported completing her seated physical activity program 5 days per week for 30 min at a time with 3 rest breaks. She reported using energy conservation and problem-solving strategies to plan her days and varying her activities throughout the day and the week, to which she attributed her elevated mood. She reached out to her local senior center and was now receiving Meals on Wheels, which she saved for the evening to avoid having to prepare a meal while Jan was at work.
Case Study 2: Jordan
Jordan is a nonbinary 75-yr-old who was referred to outpatient occupational therapy because of the recent progression of diabetic neuropathy in their lower extremities secondary to long-standing Type 2 diabetes mellitus, resulting in a fall. Jordan is a retired university professor emeritus of mathematics. They live alone in an urban neighborhood near campus in a townhome. Jordan manages the home and is not responsible for snow removal or lawn care. Their daily routine includes sleeping in, meeting retired colleagues for coffee, working on scholarly activities for several hours each day at their campus office, and caring for their cat. Jordan’s hobbies include cooking for weekend dinner parties with friends and reading. Before the diabetic neuropathy worsened, Jordan enjoyed walking to campus when the weather allowed. Jordan was referred to occupational therapy for self-management of their diabetes and diabetic neuropathy.
Occupational Therapy Initial Evaluation and Findings
Using AOTA’s (2021b) Occupational Profile Template as a guide, Jordan’s occupational therapist conducted an initial evaluation, which revealed the following: Jordan is independent in functional mobility, dressing, eating, and showering. They have been sedentary since the recent fall. Jordan does not have issues with balance or home safety. They describe their home as being very accessible. They had purposefully purchased the townhome 10 yr previously to allow them to age in place. The townhome has one level with a no-step entry and has decorative grab bars installed near the toilet and in the walk-in shower. Jordan enjoys entertaining friends by making fun cocktails and cooking extravagant meals.
Over the past several months, Jordan has noticed numbness and tingling in their feet. Jordan recognizes the need to take better care of their feet and would like to learn strategies for preventing further foot complications. They also want to find ways to exercise but prefer to do it in a group. Additional findings from the evaluation are provided in Table 6.
Assessment Findings for Jordan
Occupational Therapy Interventions
Jordan attended six occupational therapy outpatient visits over 6 wk. All visits were delivered in person at the clinic. Using the diabetes foot care algorithm displayed in Figure 2, the practitioner and Jordan collaboratively focused their plan of care on diabetic foot care strategies and group-based education and exercise. The sections that follow describe evidence-based interventions that could be implemented with Jordan by either an occupational therapist or an occupational therapy assistant. Target outcomes included improved performance of ADLs and participation in leisure and social activities.
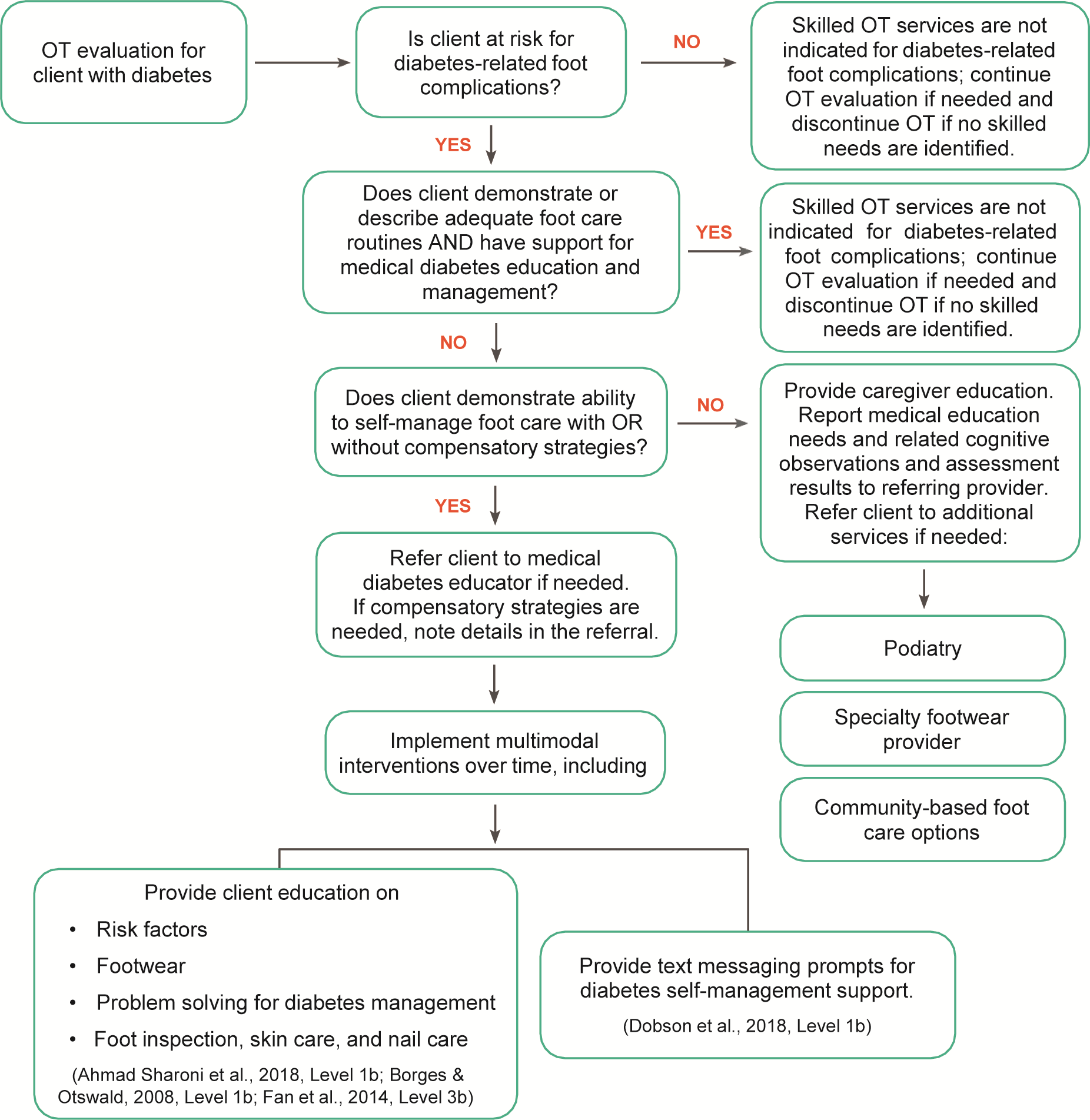
Decision-making algorithm for interventions to prevent diabetes foot complications.
Diabetic Foot Care Intervention
The occupational therapy practitioner educated Jordan on foot self-care. In particular, the practitioner shared information on risk factors, appropriate footwear, when to call the doctor, and the importance of daily foot inspections. The practitioner taught Jordan problem-solving strategies for avoiding serious foot problems (Ahmad Sharoni et al., 2018; Borges & Ostwald, 2008; Fan et al., 2014). For example, the practitioner instructed Jordan to do a daily skin and nail inspection of their feet. Jordan recognized that their nails were discolored and brittle. To help Jordan understand the problem, the practitioner shared that discoloration could be a result of a fungal infection and encouraged them to schedule a call with a podiatrist and do some online research on available treatments. The practitioner also provided Jordan with information on an automated text messaging program called SMS4BG (Dobson et al., 2018). This program was designed to help motivate people with diabetes to engage in healthy behaviors, such as daily foot inspections. Jordan learned that they could receive the motivational messages for free by signing up for the program online.
Group-Based Self-Management and Exercise Intervention
Every Thursday morning for an hour, the occupational therapy practitioner led a group-based diabetes self-management program focused on goal setting, physical activity, and healthy eating (Gregg et al., 2007; Trouilloud & Regnier, 2013). Jordan decided to participate in the program for five of their six occupational therapy visits. During this time, Jordan connected with others who had diabetes. As a group, they engaged in resistance band exercises and shared healthy recipes (King et al., 2006). The practitioner was familiar with community resources and assembled a list of local support groups for people with Type 2 diabetes to share with the group. Participation in these support groups can create a sense of community and empower people to improve or maintain their health and wellness (Self-Management Resource Center, 2021).
Discharge Summary
After participating in occupational therapy interventions in six outpatient visits, Jordan met their established goals. Jordan’s COPM scores improved from 4/10 to 8/10 in both Performance and Satisfaction. Their Problem Areas in Diabetes score (Polonsky et al., 1995) improved from 37.5/100 to 12.5/100, indicating reduced diabetes distress. Jordan reported that they had resumed walking to campus on a more regular basis. They had also started preparing the healthy recipes they learned from the self-management program for their friends during weekend dinner parties. Although Jordan had not yet joined a support group in the community, they had established a routine of meeting up with new friends from the self-management program at a local YMCA to exercise twice a week. Jordan had also incorporated a daily feet check into their hygiene and grooming routine. They now trimmed their nails regularly, washed and dried their feet every day, and inspected their feet for any sores or changes to the skin.
Strengths and Limitations of the Current Body of Evidence
Strengths
Systematic reviews explore specific clinical questions that are guided by a priori question development and a review process protocol. No systematic review can address all aspects of a topic; systematic review authors make decisions on which aspects to include and exclude before conducting the review. Additionally, the literature search may miss relevant articles; using best practice methodology can reduce this bias. We attempted to follow best practices at every step of the process, in part by getting input at all stages from practitioners, researchers, consumers, and experts in the topic areas included in the review.
The review questions that form the basis for this practice guideline were developed with an intentional focus on occupation-based outcomes. Because occupation-based outcomes are the goal of occupational therapy, these were the outcomes reported in the reviews. Additionally, AOTA has published systematic reviews and practice guidelines for diagnoses such as stroke, Alzheimer’s disease, and arthritis; we did not include those diagnoses in this review to avoid overlap. Gaps in the research supporting particular interventions does not mean that practitioners should not use those interventions. Rather, it means that the evidence is insufficient to support evidence-based practice and that practitioners should instead rely on expert knowledge to guide practice. Such knowledge can come from practitioners’ own training and experience or from connecting with experts in an area to gather their opinions. In the sections that follow, we pinpoint important gaps in the evidence for interventions that practitioners can consider using as appropriate.
Limitations: Gaps in the Evidence
Gaps in knowledge exist when the information in the literature about interventions is insufficient, imprecise, inconsistent, or biased (Robinson et al., 2011). Gaps also exist when the information in the literature is not sufficient to answer a clinical question. Therefore, practitioners must combine current evidence with expert opinion and their own training and experience to provide the best care possible.
Practitioners need to think about the elements of evidence-based practice as they evaluate this guideline in light of gaps in the literature related to their clinical practice. Practitioners should consider the following questions when they identify these gaps (Gutenbrunner & Nugraha, 2020): What evidence exists? What are the best practices associated with providing services to this client population? What interventions are contraindicated for this population? What outcomes am I hoping to achieve with this client? Does evidence exist in another field or discipline related to interventions and desired outcomes that are within the scope of occupational therapy practice with this client population? What are my client’s preferences and values? Does my client prefer one intervention over another? Are available resources, cost, or time influencing my client’s preference? How might the intervention I am considering affect my client’s performance patterns and roles? Does my client find the intervention I am considering meaningful? What experience and expertise do I have that can help guide my decisions? What types of interventions have I used previously that were effective with similar clients or populations? What types of interventions have I used previously that were ineffective with similar clients or populations? What potential risks does the intervention I am considering pose to my client or this client population? What types of interventions to address this client’s concerns and challenges were part of my occupational therapy education? Will the health care system or organization be supportive of this intervention? How will I document this intervention? How will I document the outcomes associated with this intervention? Is it likely that this intervention will be reimbursed?
Overall, the results from the systematic reviews on chronic conditions support occupational therapy practitioners’ use of a multimodal approach to help adults manage one or more chronic conditions. This approach must include education, goal setting, and problem-solving components delivered over an extended period of time. The clinical recommendations from the systematic reviews may be incomplete because of insufficient, imprecise, inconsistent, or biased evidence. Therefore, the following sections present additional information and suggestions related to occupational therapy’s role in addressing self-management of chronic conditions with adult clients. These sections are based on existing or emerging evidence, expert opinion, or both.
Prevention Approach
Much of the evidence in the systematic reviews is focused on strategies adults can use to improve or maintain health behaviors after diagnosis with one or more chronic conditions. However, the evidence provides no strategies that focus on prevention. The risk of having more than one chronic condition increases with age (Vogeli et al., 2007); therefore, adults must be provided with strategies for preventing not only the progression of their current chronic conditions, but also the onset of additional chronic conditions. Occupational therapy practitioners can intervene at the primary, secondary, and tertiary prevention levels using occupation-based interventions. AOTA (2020a) developed a position statement on occupational therapy’s role in the promotion of health and well-being that provides examples of occupation-based primary, secondary, and tertiary prevention interventions.
Habits and Routines
Much of the evidence in the systematic reviews does not explicitly connect self-management interventions to habits and routines, likely because most interventionists in the literature were not occupational therapy practitioners. Occupational therapy practitioners are skilled at assessing and addressing clients’ performance patterns, which “are the acquired habits, routines, roles, and rituals used in the process of engaging consistently in occupations and can . . . help establish [healthy] lifestyles” (AOTA, 2020b, p. 12). The evidence-based Lifestyle Redesign® program, for example, provides occupational therapy practitioners with practical guidance on helping adults enact a personalized and sustainable daily routine that promotes health and well-being (Jackson et al., 1998). Research on the Lifestyle Redesign program has demonstrated the program’s ability to enhance health and quality of life among community-dwelling older adults (Juang et al., 2018; Uyeshiro Simon & Collins, 2017).
Shared Goal Setting
Much of the evidence in the systematic reviews is focused on helping clients develop individual self-management goals. Studies on goal setting infrequently included family and caregivers in the process. Social support has been found to help adults build “the skills and confidence they need to lead healthier lives” (Agency for Healthcare Research and Quality, 2020, para. 6). Family and caregivers often help adults identify personal barriers and incorporate problem-solving techniques into their daily lives (Jordan, 2014). Occupational therapy practitioners can take advantage of a variety of tools, such as goal-setting worksheets, to help improve clients’ self-management support. The Institute for Healthcare Improvement (2021) has provided a list of tips for setting and documenting collaborative self-management goals for adults with chronic conditions.
ADLs and Medication Management
Much of the evidence in the systematic reviews does not specifically address ADLs beyond diabetic foot care. ADLs in general are commonly addressed in occupational therapy intervention (AOTA, 2020b; Laposha & Smallfield (2020), and yet relatively little evidence in the reviews relates self-management of chronic conditions to improved ADL performance. In much of the research, reported outcomes for ADL and IADL performance were combined; future research teasing ADL and IADL outcomes apart would enhance knowledge and intervention in these areas. Similarly, medication management is an important component of self-management of chronic conditions and is within the occupational therapy scope of practice (AOTA, 2020b; Schwartz & Smith, 2017); additional research is needed that focuses on the distinct value of occupational therapy interventions in promoting medication management for adults living with chronic conditions.
Young Adults
Much of the research in the systematic reviews was conducted with middle-aged and older adult participants. This finding may be attributed to how young adults transition through U.S. health systems (Butler, 2021). Many young adults with chronic conditions must learn to navigate the complexity of medical services and insurance coverage when they move from pediatric to adult care. Many also transition to college, where parents have less oversight and involvement in their health care. To better address the needs of young adults with one or more chronic conditions, occupational therapy practitioners can advocate for the creation of child–adult transitional teams within their settings. They can also participate in the political system by writing or calling members of Congress to promote legislation that covers transition planning and services. AOTA offers practitioners tips and tools for taking action to support this underrepresented population (AOTA, 2021a).
Summary
This Practice Guideline summarizes the current evidence to inform occupational therapy practitioners’ clinical decision making regarding self-management interventions for adults with heart disease, chronic lung conditions, diabetes, and kidney disease. This guideline can also be used to inform occupational therapy educational curricula and professional development and to guide the future research agenda on adults with chronic conditions.
On the basis of the systematic review findings, occupational therapy practitioners are encouraged to routinely use a multimodal approach in interventions with adults with chronic conditions. Multimodal interventions include education, goal setting, and problem-solving components provided over an extended period of time to help clients establish self-management habits and routines. Practitioners should also consider the following when planning and delivering services: Using standardized performance-based assessments in addition to client self-report can capture a more holistic picture of the client’s functional performance and more accurately measure outcomes of services. Including telehealth delivery modes in combination with in-person visits can promote clients’ self-management and development of habits and routines. Collaborating with members of the interprofessional team, which includes health care practitioners, the client, and their caregivers, can help ensure delivery of a comprehensive and integrated plan of care.
Occupational therapy is uniquely positioned to address self-management from a holistic perspective, taking into account clients’ characteristics, occupations, and surrounding environment. This Practice Guideline equips occupational therapy practitioners with a summary of the available evidence along with clinical recommendations for translating the evidence into practice when working with adult clients with chronic conditions.
Footnotes
*
Indicates articles included in the systematic reviews.
Acknowledgments
The authors acknowledge and thank the following individuals for their participation in the content review and development of this publication:
Deborah Lieberman, MHSA, OTR/L, FAOTA, Vice President, Practice Improvement, and Staff Liaison to the Commission on Practice, American Occupational Therapy Association, North Bethesda, MD
Susan Cahill, PhD, OTR/L, FAOTA, Director of Evidence-Based Practice, American Occupational Therapy Association, North Bethesda, MD
Elizabeth G. Hunter, PhD, OTR/L, Assistant Professor, Graduate Center for Gerontology, College of Public Health, University of Kentucky, Lexington
Hillary Richardson, MOT, OTR/L, Practice Manager, Knowledge Translation, Evidence-Based Practice and Practice Improvement, American Occupational Therapy Association, North Bethesda, MD
Emma Burry, BS (consumer representative); Susan Charnley, DrOT, OTR/L, CHT (consumer representative); Jennifer Kaldenberg, DrPH, MSA, OT, OTR, SCLV, FAOTA; Darby Kyler, OTD, OTR/L; Krysta M. Rives, EdD, MBA, COTA/L; Juleen Rodakowski, OTD, MS, OTR/L, FAOTA; Carol Siebert, OTD, OT/L, FAOTA; Chuck Willmarth, Vice President of Health Policy & State Affairs, American Occupational Therapy Association.
The authors acknowledge the following individuals for their contributions to the evidence-based systematic review: Hussain A. Alibrahim, MSOT, OTR/L; Clare Emmert, OTD, OTR; Lea Fang, OTD, OTR/L; Beth E. Fields, PhD, OTR/L; Jennifer Kaldenberg, DrPH, MSA, OTR, SCLV, FAOTA; Pamalyn Kearney, EdD, MS, OTR/L; Darby Kyler, OTD, OTR/L; Natalie E. Leland, PhD, OTR/L, BCG, FAOTA, FGSA; Robin Newman, OTD, OTR, CLT, FAOTA; Juleen Rodakowski, OTD, MS, OTR/L; Stephanie A. Rouch, MOT, OTR/L; Kathleen M. Sutton, PT, DPT, PhD, MPH; Patricia Watford, OTD, MS, OTR/L.
Note: The authors of this Practice Guideline (Beth Fields and Stacy Smallfield) have signed a Conflict of Interest statement indicating that they have no conflicts that would bear on this work.
Appendix: Overview of the Systematic Review Methods and Findings
The systematic reviews completed for this Practice Guideline were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).