
Abstract
Rohingya refugees experience imbalanced, deprived, and maladapted occupations in refugee camps and should have access to comprehensive health and rehabilitative care, including occupation-based services, to facilitate their social integration.
Rohingyas are considered an ethnic minority, and they represent the most notable percentage of Muslims in Myanmar, with approximately 1 million living in Rakhine State at the beginning of 2017 (Institute of Medicine, 2021). Beginning in the 1990s and escalating in August 2017, Rohingya women and girls have been raped and abused, numerous Rohingya civilians have been killed, and their villages have been burned during military attacks by local Buddhist mobs. The Myanmar government refuses to grant the Rohingya citizenship, and as a result most of them do not have any legal documentation, effectively making them stateless. Because of the severe political and religious violence, almost 800,000 Rohingyas have crossed the border between Myanmar and Bangladesh since the 1990s (Leidman et al., 2018). In May 2018, the World Health Organization (WHO) reported that the Rohingya displacement camps in Bangladesh required about $950 million in funding, but at that time only 6.3% of the targeted health-related funding had been met (United Nations, 2018). This limited access to critical and lifesaving services, such as food, drinkable water, shelter, and health care, turned into a severe humanitarian crisis (Ahmed et al., 2018). In addition, overcrowded makeshift huts have challenged existing health care facilities. These challenges are exacerbated by frequent environmental hazards, such as landslides and flooding, that affect ongoing humanitarian responses. Insufficient resources in the Rohingya camps drew international attention to the everyday health care needs of Rohingya refugees.
The environmental stressors in Rohingya camps, and their impact on everyday life, have not yet been thoroughly researched in Bangladesh (Chynoweth et al., 2020). As a consequence, there is a need to better understand how Rohingya refugees in Bangladesh participate in their everyday occupations despite the health-related consequences of persecution, war, and historical trauma, as well as daily environmental stressors associated with living in temporary shelters at different camp locations. It is also important to understand how participating in everyday occupation influences health and quality of daily life. This knowledge is essential if effective health care and rehabilitation support services in temporary living shelters of refugees, in particular in Bangladesh, are to be developed.
Previous research with Rohingya refugees has identified a correlation between restricted participation and posttraumatic stress disorder (PTSD), anxiety, and depression (Doherty et al., 2020). Research has found that mental health conditions challenge a person’s ability to participate in everyday life (Riley et al., 2017), yet existing essential rehabilitation services in Rohingya refugee camps include screening for only basic health conditions and have failed to address comprehensive mental health and occupation-based care (Khan & Haque, 2021). Additional care services, such as donating blankets or food relief, assisting women with pre- and postnatal care, or providing stoves to decrease air pollution, are offered by charitable organizations. The Bangladeshi government has demonstrated limited health care capacities, with minimal action taken to improve living conditions inside Rohingya camps (Fischer et al., 2021).
The existing literature also shows that Rohingya refugees face challenges in everyday occupations because of violence, limited opportunities to manage everyday needs, lack of proper hygiene, malnutrition, and continuous physical and sexual harassment by neighbors and local community members (Wali et al., 2018). Given such conditions, it is essential to further understand how Rohingya refugees participate in everyday occupations and how they address occupational changes to promote their overall health and well-being. It is also important to note that existing research with Rohingya refugees has not been conducted from an occupational therapy perspective. Occupation-focused research may enable occupational therapy practitioners to offer more impactful and meaningful care for refugees living in displacement camps in an environment with limited resources. Evidence to inform occupational therapy’s contribution to refugees living in low-resource environments during a humanitarian crisis is limited. More research can help identify the support needed for people experiencing long-term displacement to enable them to resume previous occupations and establish new ones within their current environment.
The purpose of this study was to explore how Rohingya refugees experience participation in everyday occupations while living in Rohingya camps in Bangladesh. In this study, participation is the term we use to define the meaning of perceived engagement in everyday occupations. The WHO (2022) defines participation as involvement in life situations. The International Classification of Functioning, Disability, and Health (ICF), created by the WHO, serves as a framework for conceptualizing participation, health, and disability at both the individual and population levels. The ICF further categorizes participation into five domains: (1) self-care (activities of daily living); (2) domestic life (instrumental activities of daily living); (3) interpersonal interaction and relationships (social participation); (4) major life areas (education and work); and (5) community, social, and civic life (play, leisure; Boyt Schell et al., 2014). Although such categories can serve as conceptual boundaries for research involving Rohingya refugees’ participation in daily occupations, it should be noted that the subjective meaning of participation is missing from the ICF (Hemmingsson & Jonsson, 2005). Previous research has highlighted the importance of acknowledging the links among subjective experiences of participation, health, and well-being (Pendleton & Schultz-Krohn, 2013). To emphasize this link, participation in the current research also encompasses subjective and passive participation (e.g., observing others, receiving care, and listening) to capture a holistic understanding of how Rohingya refugees experience participation in everyday occupations while living in refugee camps.
Research Questions
We explored the following three research questions: (1) How do Rohingya refugees experience daily life while living in refugee camps in Bangladesh, (2) what daily occupations do refugees participate in, and how do they make sense of these occupations, and (3) what environmental factors do refugees perceive as supporting or hindering their engagement in daily occupations?
Methods and Materials
Research Design
We used the phenomenological method, which entails application of hermeneutics and selection of participants who have lived experience of the social phenomena of interest, who are willing to talk about their experience and related personal meaning, and who are diverse enough from one another to enhance the possibility of rich and unique stories of their particular experience (Rodriguez & Smith, 2018). Specific social phenomena of interest include the beliefs, interactions, and functions of Rohingya refugees that involve the family and other people in a crisis.
Researcher Positionality, Roles, and Power Dynamics
The first author (Yeasir A. Alve) is a Bangladeshi occupational therapist who has supervised the fieldwork of occupational therapy interns in marginalized communities and coordinated this research project. The second author (Azharul Islam) has 1 yr of experience working in various refugee camps, and the third author (Brittany Hatlestad) is a graduate research assistant who provided assistance in the process of research analysis. The fourth author (Mansha P. Mirza) is an occupational therapist and seasoned researcher with more than 15 yr of experience doing research and community service with refugee communities. Data collection for this study was primarily conducted by Islam under Alve’s guidance and supervision. Data analysis was conducted collaboratively between Islam and Alve, and Hatlestad and Mirza helped with the organization of themes and the development of the study’s implications. All four members of the research team approached their roles and this study with a firm belief that all persons are entitled to human and occupational rights. None of the authors has personal refugee experience, although Mirza has a family history of displacement and refugeehood. All authors acknowledge their privilege as professionals with freedom of mobility and a steady income. During fieldwork, steps were taken to ensure that the resulting power differential between the researchers and the study participants did not coerce or further marginalize the participants. For example, the interpreters in this study were persons with personal refugee experience who had lived in a refugee camp for many years. Their involvement reduced the power imbalance that inherently existed between researchers and participants and created a dynamic that invited participants to express their views freely.
Participants
The participants, people who live in the Rohingya camps, were selected through a heterogeneous sampling strategy (Patton, 2002). The Bangladeshi Office of the Refugee Relief and Repatriation Commissioner approved the research ethics and safety guidelines for conducting this study (Approval No. 2018-2077). The Bangladeshi government granted permission to access refugees from three designated Rohingya camps. Participants were recruited from these camps on the basis of the following inclusion criteria: (1) adult refugees between ages 18 and 60 yr, (2) a minimum of 6 mo to a maximum of 2 yr of living in Rohingya camps, and (3) cognitive capacity to respond to questions during the interview. The specific time frame of 6 mo to 2 yr was selected because that is when displaced people experience the most challenging events, engage in self-reflection or dialogue with themselves, and begin to make decisions that affect the rest of their lives (Davies, 2005). Participants were excluded if they (1) had communication difficulties due to any speech disorders or notable cognitive impairment or (2) had permanent residency in the host country and lived in settings other than the three designated camps. Acting as research collaborators, the data collector (Islam) and native Rohingya interpreters received training from Alve to ensure personal, research participant, and environmental safety during interviews. The first two interpreters who responded to a job ad posted in the camps were selected on the basis of the following inclusion criteria: (1) were natives of Myanmar who evacuated to Bangladesh in 1990; (2) had a legal refugee card that allowed them to visit different camps, humanitarian organizations, and the local community; and (3) were older refugees (age ≥60 yr) with long-term refugee camp experience and consequently had developed skills to minimize any emotional or behavioral consequences during the interview.
Recruitment involved two components: (1) building rapport between the researchers and the potential participants through native interpreters and (2) screening potential participants. In qualitative research, native interpreters are commonly used to efficiently understand specific local languages (Schweitzer & Steel, 2008). To recruit participants, the person in charge of the camp shared the data set of 80,000 Rohingya refugees who lived in the research-permitted camps. On the basis of inclusion and exclusion criteria, the research collaborators identified 10 potential refugees from each camp. They then narrowed the total number of candidates to 20 by prioritizing the heterogeneity of sociodemographic characteristics, such as different gender, living areas, marital status, and types of a family (e.g., two-parent vs. single-parent households). At the initial meeting with participants, the research collaborators emphasized that participation was voluntary, that pseudonyms would be used to ensure anonymity, and that participants would be able to withdraw from the study at any point in the process. After the collaborators received verbal and written consent from the 20 initial refugee participants, the first interviews started. Three candidates withdrew at the time of the second interview and requested that their information be removed from this research. Two other participants were not available during the daytime or while the research collaborators visited their temporary living shelters. The characteristics of the final 15 participants are presented in Table 1.
Participants’ Sociodemographic Information
Note. EQ = educational qualification (for Rohingya people, elementary school = Grades 1–5, high school = Grades 6–10); F = female; G = grade; I = illiterate; JP = multiple-joint pain; LBP = mechanical low back pain; M = male; MIP = main income person; MS = marital status; NFM = number of family members; Nil = no significant occupation during the interview; OA = osteoarthritis; RA = rheumatoid arthritis.
Data Collection Procedure
Data gathering consisted of two interviews with each participant and additional observations to help us better understand the local context through a cultural lens. Two interviews were deemed appropriate to allow for building rapport and collecting foundational data during the first interview and for asking follow-up and clarification questions during the second interview. Islam conducted semistructured, in-depth interviews developed from guidelines outlined by Smith and colleagues (2009). He speaks the Chittagonian dialect, which matches 90% with the Rohingya language; however, the accents are different. Although familiarity with 90% of the vocabulary of a language is substantial, it may lead to some information being missed; thus, interpreters were used to fully comprehend the meaning of participants’ responses, including their local jargon. Questionnaires were developed in Bengali and later translated into the Chittagonian dialect by Islam and the interpreters. All interviews took place at each participant’s shelter. The interpreters initiated the first interviews, and the participants were asked to describe their experiences through an initial open-ended question: “Can you please tell me about daily life activities that you are doing in your small shelter?” Participants then were encouraged to expand their explanations through semistructured questions (see the Appendix). The interpreters explained Islam’s questions to the participants and summarized the participants’ answers for him while providing an additional explanation for unclear jargon or meaning. This helped clarify responses for Islam, who understood the local language, with the exception of some jargon. Because the interpreters translated and clarified the meaning of any jargon in the presence of the participants being interviewed, this process verified the accuracy of translation and helped avoid misinterpretations.
In the second interview, the participants were requested, while respecting their personal and religious dignity, to show, explain, and demonstrate their daily living activities inside and outside the temporary shelters. Islam conducted both participant and nonparticipant observations of these activities using a structured guide that included cues to capture the physical and social environments (see the Appendix). He also informally communicated with other family members and neighbors, when participants granted permission, to obtain additional perspectives that could shed more light on the participants’ statements. With multiple generations of family members living in the same shelter, some participants asked to discuss certain topics, such as experiences of domestic violence, a spouse’s extramarital relationships, or unauthorized work, privately, outside the living shelter.
The two interviews were conducted between November 2019 and January 2020, and each interview took 1 to 2 hr. Data were recorded using an IC Recorder (Sony PX470), and field notes were recorded to capture participants’ actions, expressions, and gestures (Sutton & Austin, 2015). Islam and collaborators separately transcribed interviews verbatim in formal Bengali language. Alve resolved the dissimilarities through conversations with Islam and the collaborators in February 2020.
Data Analysis
Interpretive phenomenological analysis (IPA) involves the authors’ sustained engagement in an interpretative relationship with the transcripts and field notes to capture and do justice to the participants’ experiences in their mental and social worlds. The flow of data analysis followed the IPA’s six-step guideline, with flexibility (Smith & Nizza, 2021). The process of interpretation adopted line-by-line analysis to capture quotations and patterns that depicted experiences of participation in daily occupations. Participant experiences were translated to English and are quoted in this article using pseudonyms. All captured quotes were termed, collectively, initial codes. First, Islam transferred all initial codes to an Excel file, after which he and Alve read the initial codes separately to interpret the meaning of each code. This interpretation process involved supporting documents, such as field notes and notes from observations. The notes helped contextualize participants’ verbal comments; illustrate participants’ facial expressions and nonverbal language; and emphasize particular phenomena, such as a feeling of stress because of an unexpected routine or an embarrassment because of involvement in unlawful activity.
After interpreting the meanings of the codes, Alve and Islam engaged in an analytic discussion to eliminate any confusion. The mutual coding process determined a total of 22 selected codes by comparing each participant’s quotations. To aid in categorization, Islam assigned an operational definition to each selected code that was based on the initial codes and quotations. For example, a selected code “feelings of insecurity” was assigned the operational definition “anxiety regarding everyday goals, lack of confidence to maintain relationships, and inability to handle the crisis.” Alve revisited all the draft categories that were derived from the 22 initial codes. Further discussion with Hatlestad and Mirza resolved any remaining disagreements regarding coding and the process of categorizing codes. By comparing the codes and categories, we identified four initial themes, two of which could be further categorized into two subthemes each.
Trustworthiness and Rigor
Strategies outlined by Koch (2006) were used to ensure research quality, consistency, and structure. Islam conducted pilot interviews with two potential participants before commencing formal data collection to modify the interview and observation guides as needed. To establish credibility, interviewers kept field notes during the first and second interviews to record experiences while asking questions and observing everyday occupations in the participants’ natural environment. The research collaborators transcribed, encoded, and analyzed all the data separately in interpreting study findings.
After completing the data analysis, Islam and the interpreters executed member checking and ensured that the draft themes and categories represented the participants’ voices. The interpreters met with the participants and shared all anonymous and individual quotations connected to the drafted themes and subthemes in the form of a flyer. Over the course of the data collection, one-third of the participants were relocated to different refugee camps, and it was challenging for interpreters to locate them. Most of the participants gave their approval of the themes and subthemes. Others disagreed and offered suggestions for potential edits to more accurately reflect their lived experience. Thus, the categories were reevaluated and edited on the basis of the participants’ opinions regarding the themes and subthemes, which ultimately enhanced their trust in the research process. The dependability of the research was increased because two authors were separately involved in the initial coding process, and consultation with Hatlestad and Mirza helped conceptualize the categorization and theme making. In addition, reflexivity helped bring forth any preconceptions that entered the analysis. For example, the back-and-forth process of identifying themes, categories, and initial codes throughout the analysis resulted in a more authentic reflection of experiences shared by the participants.
Results
On the basis of the findings, we identified four notable themes that characterized participation in everyday occupations among Rohingya refugees: (1) mental stress, sleep disturbances, and daily occupations; (2) adjusting to inconsistent daily activities; (3) decreased occupational engagement due to complex relationships and limited social roles; and (4) involvement in precarious occupations that exacerbated severe health risks.
Theme 1: Mental Stress, Sleep Disturbances, and Daily Occupations
Mental health conditions, such as anxiety, depression, PTSD, restlessness, and suicidal ideation, negatively affected sleep routines, which in turn hindered participants’ ability to take part fully in daily activities. Participants engaged in several adjustment strategies, such as modifying routines and spiritual healing, in an attempt to address these problems.
Past incidents, such as human trafficking and genocide, were experiences that interfered with peaceful sleep and rest. Participants mentioned difficulty sleeping at night. The concerns they expressed included sudden wakefulness, wild laments, crying, unusual sweating, and frequent thirst. Participants themselves, or their families, had previously experienced physical torture, such as hearing and seeing weapons being fired, witnessing murders or rapes, and other experiences that eliminated peaceful rest. Participants felt panicked or upset every night and frequently became sick. As a result, sleepless nights interfered with daily occupations, as evidenced by this quote from Begum: I often dream that some bastards are raping me forcefully, crying loudly, and no one came to [my] rescue. . . . I sweated after this nightmare and cried the rest of the night. This situation has devastated my intentions to pay attention to daily activities.
This quote expresses the intensity of suffering after Begum had crossed the border. She did not feel safe in the temporary living shelters. Another participant, Banu, stated being afraid of some people who always peered at her in an inappropriate way: “Some men looked like they were raping me with their eyes. I feared, became restless, and could not pay attention while cooking. . . . Most of the time, I forgot about the sequence of steps to make a meal.”
Banu had difficulty trusting anyone after her experience of genocide in Myanmar, which affected her relationships. She mentioned that her older sister had been raped by eight adults, one after another, and had died before she crossed the Myanmar border. Banu had not experienced deep and restful sleep since she fled.
Like Banu, Ali experienced restless sleep interrupted by mistrust and insecurity: “Look, I have some valuable stuff [shows a gold necklace] here [in his shelter]. I am always afraid of someone stealing my wealth and cannot sleep at all because of a lot of negative thoughts.” As he spoke, he was repairing a fishing net and lost the sequence.
Ali experienced insecurity that was due to his desire to protect his family from snatching (kidnapping) or robbery and was concerned about his adolescent daughters’ safety. He never allowed them to go anywhere alone, and he did not sleep at night as a way to protect them.
For other participants, like Akbor, natural hazards, such as heavy rain, flash floods, and landslides, perturbed their rest and sleep: Look at the slopes of the hill [because of heavy rainfall, the shelters are vulnerable to being buried by landslides]. We are vulnerable to landslides in this monsoon period. I am very anxious to sleep underneath these hills, and the shelter is not strong enough to protect [against] the wind speed. I completely lost interest in living here.
After sharing this, Akbor took a break from the interview.
Participants often went to bed fearful about what was to come the following day. The lack of peaceful sleep and rest caused them to remain upset throughout the day; lose social connections; become disinterested while performing personal, household, and social responsibilities; and be physically unwell. Complicated daily living activities, such as washing clothes (scrubbing, rinsing, and drying clothes manually), cooking (using firewood), bathing children (using a manual water pump), and regular personal hygiene were intentionally overlooked. Because of their restlessness, the participants would quickly become fatigued and thus would put off daily activities on purpose. For example, Sajib, another participant, said that he takes a shower once a week. Overall, the restless and sleepless nights resulting from mental stress and sociocontextual situations prevented participation in everyday activities.
Theme 2: Adjusting to Inconsistent Daily Activities
Inconsistent daily activities created unique everyday routines. Participants used spiritual healing skills to adapt to the constraints and created a routine in daily activities. Most of the time, female participants collected relief supplies (e.g., rations, kitchen items, fuel) instead of their husbands. The male wait line was longer than the one for women, and men were occupied with income-generating work outside the camps, which was often conducted illegally. Despite the shorter lines to obtain relief supplies compared with men, women had difficulty maintaining daily routines and caring for others because of the time commitment associated with collecting necessary supplies and caregiving responsibilities for children, parents-in-law, and younger siblings. Making eye contact, and speaking boldly, Julekha shared the following: The ration collection line was hectic and time consuming, preventing returning home early. As a result, the baby stays hungry, and the partner does not have lunch at the proper time. Most of the time, he does not have lunch and stays hungry. How stressful it is! . . . These days, I get up before sunrise to prepare everyone’s food and bring the baby outside in a backpack.
The women took on additional family and household responsibilities, which created extensive hardship and mental and physical tiredness, especially in extreme weather. The hardship presented physically, through muscle and joint pain around the neck, shoulders, wrists, and heels. Nevertheless, women continued to uphold their duties, even if their extended family responsibilities resulted in their own inconsistent daily routines. During time that should be their rest period, women were noted to complete light chores and chat with family members, direct children’s home education, prepare meals, and oversee household items. Lipi started crying after providing this description: Once, we strived for food when I had a fever, and my partner went fishing in the deep sea without any return notice; there was no one to cook food. . . . I was shocked, messed up, and unable to help. I did not find any meaningful work except praying to God to save my family.
The lack of financial resources in the Rohingya camp limited access to camp-based health care, delivery items, and means of livelihood for those waiting for their refugee identity cards. Refugee participants had much more freedom to access natural and aquatic resources in Myanmar; however, in Bangladeshi refugee camps they were living under conditions of confinement, with limited access to natural resources. Participants reported practicing spiritual activities to adjust to the agitated mindset and uncertainty that accompanied daily activities. As one participant, Roshida, proudly explained, these spiritual activities included praying on time; reciting passages from holy books; and discussing the tragedy, patience, and virtue of their holy prophets: We have 10 family members in our shelter, and I lose almost all energy in the middle of the day by taking care of children and parents. . . . I found that God is healing me after practicing five-times prayers every day. . . . I do not know how did I get the bits of patience to manage everything.
Overall, participants balanced everyday occupations in their hostile sociocultural environment through adaptation, alteration, and spirituality.
Theme 3: Decreased Occupational Engagement Due to Complex Relationships and Limited Social Roles
Participants mentioned complex relationships, such as mistrust of a spouse, other family members, or neighbors, that affected their ability to perform social functions. Fragmented relationships decreased motivation to care for the self and others, but this could be solved by forming new relationships and making connections in shared roles.
Subtheme 3.1: Fragmented Family Relationships
Participants had been separated, intentionally or unintentionally, from family members and relatives after arriving in Bangladesh. They mentioned a sense of disconnection because they lived in different camps, and the lack of cellular phone coverage limited their ability to communicate with others. It was a helpless situation because the neighbors did not like to talk with one another because of mistrustful attitudes that influenced personal and interpersonal relationships in the camps. Mistrustful attitudes were expressed by using an additional lock on one’s belongings, counting savings repeatedly or suspiciously, refraining from borrowing money, and keeping a sharp object or a stick to protect the self in case of any unwanted situation. Most of the participants had previously been in a joint, extended family; therefore, their communal roles were affected after transitioning to the refugee camps. Motin, speaking boldly, shared this information: I took all of the caregiving responsibilities of my father after he had a stroke. . . . I lost interest in communicating with siblings because they escaped from their duties to parents. . . . If my family members can’t be trusted, how could neighbors be trusted? I learned how to live alone.
The participants also mentioned how poverty affected their relationships with their spouses. Some of them were involved in extramarital relationships because their spouse was unable to provide money or food or did not fulfill specific personal and family needs, such as gorgeous dresses, children’s fancy foods, or certain groceries. Extramarital relationships with the authorities were helping some people receive valuable gifts and facilitated affluent living, despite the negative effects on their relationships with family members. In such cases, misunderstandings arose between couples, worsening the marital relationship and causing an imbalance in their mutual roles. With eyes cast downward, Sojib described his situation: Once, I could meet the family’s needs, but now, my wife does not talk and often quarrels. The situation made a wall between us and our married life. . . . We do not care about each other and are separated even though we live in the same shelter.
The participants were missing their connectedness with partners in everyday household activities and were vulnerable to sexual violence. The husbands often beat their wives if they became sick or pregnant. These incidents interfered with their parent or spouse roles. Roshida tearfully described her own experience: My husband was idle and unhelpful. Often, he sells relief items and buys cannabis. I tried to stop this bad habit. . . . Despite being pregnant, he has beaten me so badly. I felt like I would die but could not . . . because of my unborn child.
Participants were missing meaningful occupations because of their unstable relationships. These relationships were not deep, and many partners did not willingly cooperate in the performance of mutual daily activities. Moreover, poverty changed their intention to complete interdependent occupations, such as caring for children and parents, shopping, and washing clothes. However, some participants recognized this imbalanced occupational life and reformed their relationships to create harmony in their everyday life.
Subtheme 3.2: Forming New Relationships to Perform Social Roles
Rohingya families were able to create social bonds despite traumatic personal and communal experiences. Participants started to take care of their families and spend more time with their neighbors, which helped to build trustworthy relationships. Participants realized the need to compromise and support each other. Bilkis, caressing her younger daughter, shared that “Neighbors’ children were cared for here, they come to play with our kids, and I share food and receive love and care from my neighbors as an unexpected reward.”
Children began to attend the temporary school in the camp and discussed goals for the future. Neighbors exchanged their resources with others. Male family members were active in family decision-making and shared some responsibilities with their spouses: “We have our breakfast together, then drop off the children at school . . . Mom and her friend [neighbor] were crafting sheets and woven nets and sometimes prepared meals.” As she said this, Nazma was cooking, feeding the baby, and washing dishes, and she sometimes forgot to complete her remaining tasks.
Participants mentioned their desire to rebuild relationships and social bonds by sharing roles, taking on family responsibilities, and caring for others to enhance occupational and social participation.
Theme 4: Involvement in Precarious Occupations That Exacerbated Severe Health Risks
A vulnerable living environment and limited social and political opportunities influenced the uncertain and risky lifestyles that the participants chose or experienced. The hunger and demands of children forced parents and caregivers to be involved in dangerous and illegal occupations to provide for their families. Participants understood they were participating in unlawful work, but their helpless situation forced their involvement in such occupations.
Subtheme 4.1: Inconvenient and Inaccessible Living Conditions
Participants mentioned that their living environment affected their ability to take part in everyday activities. For example, it was not easy to shower in a public space because of the lack of privacy. In addition, many females showered at night, so their access to hot water was limited, which they believed could cause colds and fevers. Couples often needed to sleep with their parents and children in the same room, which hindered their intimate relationships. Rasel, looking down shyly, said, “A partition with the bamboo sheet divided the living space from my parents. Our 10-year-old girl sleeps with her mom, and we are missing our private space.”
Participants mentioned that the environment was not accessible for older adults with diseases and disabilities. Older adults had difficulty using the squatting-style toilets because of pain in the knees, as they had to keep their knees in a semiflexed position. Other older adults refrained from going outside to the outdoor toilets in the dark and on rainy days because they had difficulty with vision, there was no electricity along the pathway, and the public toilets were far from their living quarters. In addition, physical pain affected their ability to perform activities in a low-resource environment, such as washing clothes manually and lifting heavy loads of laundry on their heads or backs, thus creating additional family burdens. The suffering lasted for an extended period of time because of the unavailability of health care workers. Overall, the inconvenient living environment restrained older adults from the possibility of doing daily activities and converting otherwise-easy activities, such as toileting and self-care, into precarious ones.
Subtheme 4.2: Continuing Unlawful Work to Survive
Daily life was complicated, and the unmet needs of children and other family members caused some people to partake in many risky and unlawful activities. The Bangladeshi government prohibits any paid or unpaid work outside of the camps, thereby compelling Rohingya refugees to engage in unlawful income- generating activities, such as the illegal selling of recreational substances, selling relief items obtained from aid agencies, gambling, and doing labor work outside the camp. Salam, close to tears, shared: Children were crying for new toys and rich foods . . . They wanted fish and meat every day that the relief items could not ensure. So, I am forced to do the work by any means, whether legal or illegal.
Although some Rohingyas sold their relief items because of different family members’ and children’s needs that relief products did not fulfill, others considered it an income-generating activity. For example, a few participants bought daily items from neighbors, such as groceries and toiletries, and sold them in the local market at an increased price. One participant was told by camp authorities to stop his work, but he was helpless. This risk-taking behavior helped him earn money.
The refugee families did not have any firewood for preparing meals and thus collected it illegally from the forest beside the camp. To do so, they would sometimes cut the trees from the host village at night. The local people took this issue very seriously. Physical altercations ensued, and one participant was injured and stayed on bed rest for a month. Many refugees were relying on cardboard cartons, polyethylene sacks, and sticks as fuel for meal preparation.
Few participants were often involved in risky and illegal occupations, such as criminal activities, smuggling, and robbery, to make money to support their families; they mentioned that the supports and care they received from the camps were inadequate. They often imported Burmese products, such as cigarettes, cosmetics, cannabis, heroin, and alcoholic drinks. Some participants worked outside the camp as day laborers. Nazma said her husband worked illegally in the nearby brickfield, getting paid $2 for 6 hr of work, without food. Owners sometimes behaved harshly and refused to pay for services because the refugees do not have legal permission to work outside the camp. One of the participants, Sojib, had trouble selling relief products in the local market and was beaten by the local people. Not making eye contact, he said, Sometimes the buyers do not provide enough money and often slap or beat [us] if we argue for the fair payment. . . . I am okay with any payment as the providers did not fulfill my essentials to the refugee camp.
Thus, the participants became involved in risky occupations to meet the needs of their families. In addition, local Bangladeshis were often hostile toward Rohingya refugees. The participants said they often received warnings and punishment from the local community and were threatened with being deported from Bangladesh, and the local government seemed helpless to control such environments. This created precarious conditions in which healthy and happy participation in family and social life was unreliable.
Discussion
In this study, we explored the lived experiences of refugees existing under precarious conditions in the Rohingya camps in Bangladesh. Participants expressed restricted occupational participation because of uncertain changes in occupations, a lack of belonging, difficulty in living conditions, mistrust of others, and risk-taking behavior to obtain essential resources. These factors caused participants to experience various predicaments, such as struggling to execute a consistent routine and difficulty playing dynamic shared roles that affected their everyday lives because of a lack of trust in their spouse, siblings, neighbors, and service providers. In the following sections, we discuss these findings in relation to occupational imbalance, occupational deprivation, and adaptive occupation.
Occupational Imbalance
Occupational imbalance is defined as an inability to engage in satisfactorily diverse occupations because of a lack of balance between valued occupations and necessary or obligated occupations (Wilcock, 2006). Some Rohingya women described feeling overly occupied in roles that involved taking care of extended family members and working outside the home. Conversely, others were underoccupied and reported spending their time seeking a job in the local market or lying in bed. Yet both groups were unable to engage in meaningful occupations of choice to achieve a sense of balance and well-being. The perception of an imbalance in everyday life seemed to have the greatest implication for poor health outcomes, such as sleeplessness, drug addiction, tension, and stress or anxiety. A lack of access to health services, food shortages, and a scarcity of shelters further threatened balanced occupation, health, and well-being (Pocock et al., 2017). Given Rohingya refugees’ descriptions of their experiences in the Bangladeshi camps and the subsequent occupational imbalance, it is crucial to promote adequate occupational engagement and participation to prevent the aforementioned poor health outcomes. When occupational balance was not achieved, the refugees initially engaged in inconsistent activities and later participated in dangerous activities, such as stealing, other criminal acts, and illegal work. Through the interviews, we discovered that occupational imbalance was also derived from dissatisfaction in shared occupations that depend on connectedness between couples and other family members. Previous studies conducted with asylum seekers suggest that occupational imbalance can disrupt gender norms, causing one gender to feel powerless and worthless, which negatively affects relationships, health, and well-being (Ingvarsson et al., 2016). This sense of occupational imbalance might be a contributing factor to the wide prevalence of gender-based violence reported in the global refugee literature (Pires et al., 2019).
Occupational Deprivation
This study reflects the sense of occupational deprivation that Rohingya refugees have experienced as well as the value of participation in occupation to provide avenues to reestablish a sense of worth. Occupational deprivation is a state of being prevented from participation in necessary and meaningful occupations because of factors that stand outside the person’s immediate control, such as after a crisis, disaster, or significant displacement (Wilcock, 2006). We captured a crisis whereby the refugees were deprived of health care, food, education, and social support because they were not able to meet their basic needs while living in the camp. Refugees participated in activities that did not have any inherent meaning (i.e., lying in bed, starving for food) and did not have the opportunity to engage in desired leisure activities. Passing most of their time in the refugee camps resulted in limited social networking and support, a poor relationship with their spouse, and excessive anger and stress. The lack of engagement in paid work inside or outside the Rohingya camp created a feeling of being imprisoned in everyday life, which had the personal and social consequences of occupational deprivation and constrained participation in daily occupation. Kielhofner (2008), when discussing the foundations of human occupation, emphasized how a lack of meaningful time use reflects a sense of hopelessness, a deteriorating sense of efficacy, and a loss of control over one’s occupational choices. These themes were reflected in Rohingya refugees’ experiences in the Bangladeshi camps. In addition, occupational deprivation occurred in the context of precarious living conditions that affected refugees in different ways based on gender and age. Men had to engage in illegal work, women increased their caregiving responsibilities, and older adults were deprived of their daily occupations because of environmental hazards coupled with their own limited mobility. Precarious living conditions, such as inadequate food, an inability to feed children properly, not receiving money from partners, a lack of freedom, a fear of being abused at the shelter and outside of it, a lack of leisure and social activities, a lack of treatment facilities, and mobility impairment all played a role in creating conditions of occupational deprivation.
Adaptive Occupation
A key characteristic of adaptive occupation is the use of adaptation to alter or change an activity so that the person can perform it successfully (Mosey, 1986). Nevertheless, prolonged occupational deprivation likely diminishes the possibility of adaptive responses to new or crisis environments (Molineux & Whiteford, 1999). Participants in this research, however, adapted both positively and negatively after experiencing occupational deprivation. The substantial psychological issues resulting from displacement and deprivation could constrain refugees from adapting to existing occupations, especially when living in underresourced host countries. Nevertheless, as a temporary solution refugees altered their daily activities and connected and shared their skills with others. They displayed an eagerness to maintain relationships with their spouse, family, and neighbors by expressing a desire to help others. Previous research has noted that refugees derive a sense of purpose from occupational adaptations that focus on “doing for others” or engaging in altruistic activities (Huot et al., 2016; Smith, 2015). Posttraumatic stress interrupted daily occupations, including rest and sleep, but the refugees adapted by balancing daily activities, sharing roles, and using spiritual healing. Involvement in spirituality was a meaningful part of their everyday routines and one of the positive adaptive responses we noted. Participants used their spiritual beliefs and rituals to heal from dissatisfaction, negativity, and occupational deprivation in a complex sociocultural context.
Because the refugees were struggling to meet their basic survival needs, this study reveals that prolonged occupational deprivation can lead to maladaptive responses, such as involvement in illegal businesses, crimes, deforestation by cutting wood, and selling relief products in the community markets. Refugees’ involvement in maladaptive occupations enabled their families to survive under conditions of extreme deprivation. Some refugees believed their occupational performance was elevated by involvement in illegal businesses because doing so satisfied their family needs and allowed them to fulfill their duties as a father, husband, or son. Involvement in illegal businesses and risk-taking behavior may be defined as a maladaptation as a person attempts to rebuild their occupational identity (Huot et al., 2016). Whiteford (2000) examined maladaptive responses as adverse outcomes or failures to alleviate the negative consequence of occupational deprivation (Whiteford, 2000). However, in the present research we found both positive and negative outcomes of such responses. For example, doing unauthorized work helped fulfill family desires but also carried the risk of punishment by the authorities. Despite the fact that this involvement was unauthorized by the camp authorities, the refugees found an income-generating identity that preserved their happiness and dignity within the family. Therefore, from the refugees’ perspective these maladaptive responses were facilitating their occupational participation. The relationship between occupational balance and imbalance, occupational participation and deprivation, and adaptation and maladaptation is depicted in Figure 1.
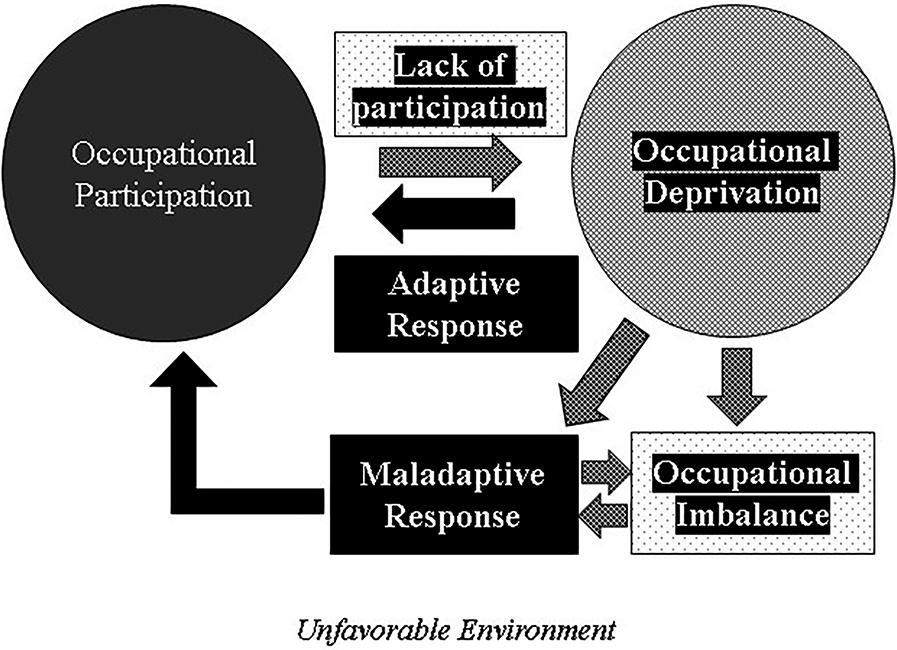
The experience of deprivation, imbalance, and adaptation or maladaptation in occupational participation.
Figure 1 reveals that a lack of participation can lead to occupational deprivation because of a lack of occupations and limited freedom to engage in occupations in an unfavorable environment. Because of occupational deprivation, participants were not able to engage in a variety of preferred and meaningful occupations, thus leading to occupational imbalance. Adaptive responses, such as altering or sharing mutual occupations and spiritual healing, were prompted by occupational deprivation, thus facilitating occupational participation. However, on the basis of research data, prolonged occupational deprivation could lead to maladaptive responses, which is essentially what causes, in part, occupational imbalance. The refugees used their resources, actions, and skills to facilitate occupational participation through adaptive and maladaptive responses. Adaptive and maladaptive occupations emerged from their occupational deprivation, depending on the duration of negative experiences and available resources. Rehabilitation professionals, aid agencies, camp authorities, and governments can all play a role in helping refugees balance their occupational lives, reduce occupational deprivation, and optimize adaptive occupational behaviors.
Study Limitations
Given this study’s aim, the results might not illuminate different strategies for helpful occupational participation that may facilitate refugees’ health and quality of life because the focus was on insufficient occupational participation and complex relationships that were increasingly dangerous to health and livelihood. Although we drew from participants’ perspectives, more research is required to study how families and service providers understand and experience occupational participation. It is also essential to understand how sociocultural factors and social relationships influence the adaptation processes in occupational participation by involving local host community members and camp service providers in future research. Because the participants were selected purposively from government-approved camps, their experiences may not be representative of all Rohingya refugees.
Implications for Occupational Therapy Practice
There is no published literature on any occupation-based rehabilitative interventions with Rohingya refugees that can guide intervention strategies for this population in the context of underresourced refugee camps. Moreover, no occupational therapy literature has yet identified how Rohingya refugees can participate in daily occupations during conditions of occupational deprivation and how practitioners can help refugees achieve a balanced occupational life and facilitate occupational adaptation. The findings of this study can inform future programs for promoting health and well-being. Rehabilitation professionals, especially occupational therapists, can help with recovery from trauma, PTSD, and sleep disturbance by providing meaningful occupational opportunities. Some examples of occupational therapist–led programs that address these issues in resource-limited refugee camps include CircusAid (2021) and Human Rights360° (2021). Both programs promote resilience and social connectedness through engagement in meaningful activities such as circus activities, mentoring hubs, and interaction with local host communities. International funding organizations, such as United Nations agencies and national and international nongovernmental organizations, should highlight the necessity of interprofessional team members to facilitate stress-free meaningful daily occupations without physical and environmental barriers. Research indicates that Rohingya refugees need more comprehensive health and rehabilitation care because of the potential health consequences associated with their precarious living conditions (Mirza, 2015). A peer-led support group may help the refugees overcome their mental health challenges and lack of social interaction. However, in Bangladesh there are few trained occupational and rehabilitation therapists and limited financial resources to develop occupational participation programs to remediate occupational deprivation and maladaptation. Moreover, nongovernmental organizations providing services in refugee camps focus on a medical-based health care model and thus do not have an emphasis on engagement in preferred occupations (Blankvoort et al., 2018). This human resource shortage could be addressed through creative strategies. For example, a community-based rehabilitation program has been piloted in Palestinian refugee camps near Amman, Jordan. This program involved prelicensure health profession students in the United States partnering with local Jordanian volunteers to offer direct rehabilitation services as well as training workshops for refugees living in the camps (AlHeresh & Cahn, 2020).
Governments and camp authorities also have a responsibility; for instance, the refugee regulatory committee or other camp authorities could address existing gaps in psychosocial services by promoting initiatives related to need-based income-generating occupations, such as gardening and vocational training. International aid agencies can also sponsor vocational training programs and offer microloans to refugee communities to establish cooperative small businesses. Such opportunities would minimize the refugees’ need to cross camp boundaries and engage in illegal occupations. Occupational opportunities such as crafting, sewing, tailoring, fishing to make money, cleaning camp areas, and loading–unloading work within camp premises may enhance livelihood opportunities and life satisfaction for refugee inhabitants of camps. Occupation-based rehabilitation services should connect refugees and their family members in the camp shelters and include awareness of maladaptive occupations. In the future, a participatory approach model of care that includes family, friends, and others could assist in developing peer- and community-based support systems. The development of such a model of care may ensure more successful transitional progress of occupational participation and enhance long-term health and overall quality of life.
Conclusion
This research increases our understanding of the experiences of participation in daily occupations among Rohingya refugees living in a temporary camp, in particular in underresourced conditions in Bangladesh. Occupational participation was constrained because of the unpredictable and complex environment or involvement in maladaptive and precarious daily activities. Rohingya refugees could benefit from sustainable rehabilitation support services. Given that Bangladesh is a developing country, the government might be unable to sufficiently increase the number of skilled occupational therapists and rehabilitation professionals. As an alternative, community-based resources sponsored by the United Nations High Commissioner for Refugees or international nongovernment organizations could be developed on an urgent basis to increase access to all health care and rehabilitation services.
Footnotes
Acknowledgments
We acknowledge Fatema Kabir Punom, speech- language therapist, for her support during data collection.
Data-Gathering Guide
| Interview Questions |
|---|
| 1. What daily living activities can you do at this settlement [Rohingya camp]? |
| • What does your everyday life look like? Tell us a little more about your everyday life from the time you got to the camp. What are the activities you do from the morning until evening? Why those activities? |
| • Tell me details of your typical 24-hr day, including your atypical daily living activities. |
| • Why was that [the activities] challenging? |
| • How are you managing now? |
| 2. What are the changes in activities that you are doing every day after displacement? |
| • Why so? How are you managing now? |
| 3. How do you deal/adjust/cope with your changing activities? |
| • What are the challenges? How do you deal with the challenges? |
| 4. How are you feeling today? |
| • What challenges prevent you from leading a meaningful daily life? How so? |
| 5. How do you manage your physical and mental health? |
| • Why so? What existing strengths can support you to be happier and fulfilled? How? |
|
|
| 1. Observing the participant: Facial expression, gesture, voice projection and tone, emotions to the particular incidence |
| 2. Observing activity of daily living |
| • Could you please show (demonstrate) how do you do that activity (i.e., doing household activities, washing clothes, feeding the children, collecting goods from humanitarian organizations)? |
| • Could you please show me how you engage in everyday activities outside your temporary shelter? Can we visit together today? |
| 3. Observing the environment (is it facilitating or inhibiting daily activities?) |
| • Structure of living shelters (resources, ventilation, living rooms, etc.) |
| • Facilities, service, supplies |
| ^ Drinking water system |
| ^ Kitchen, gas stove, power supply, and toilet |
| ^ Washing and cleaning areas |
| ^ Living shelters of neighbors |
| ^ Garbage management system |
| ^ Children’s playground and safety |
| ^ Adults’ sports and recreational venues |
| • Family privacy and relationships |
| • Relationships with the neighbors |