
Abstract
This systematic review explores evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people poststroke and concludes that addressing caregiver needs with problem-solving and support in addition to typical education and training is essential.
Stroke is a leading cause of long-term disability and is among the top diseases contributing to years lived with a disability (Benjamin et al., 2019). It has been identified as one of the most common conditions that may require caregiving (Collinson & De La Torre, 2017). After discharge from an inpatient setting, approximately 74% of people who have had a stroke are cared for by informal caregivers. Informal caregivers are broadly defined as family or friends who assist with activities of daily living (ADLs), instrumental activities of daily living (IADLs), and health management without receiving time or pay in return (Family Caregiver Alliance, 2006; Miller et al., 2010). The most common caregiving tasks performed by informal caregivers include ADLs, such as transfers or dressing; IADLs, such as transportation or shopping; and complex health management tasks, such as medication management, helping with mobility devices, or preparing special diets (National Alliance for Caregiving [NAC] & AARP Public Policy Institute, 2015; Reinhard et al., 2019).
The effects of caregiving on the caregiver have been examined extensively. Positive benefits of caregiving, such as having a purpose in life, strengthening family relationships, fulfilling family obligations, and feeling good about themselves, have been identified (Roth et al., 2015). However, the majority of research has reported negative effects on caregiver employment (Collinson & De La Torre, 2017; NAC & AARP Public Policy Institute, 2015); finances (Collinson & De La Torre, 2017; Schulz & Eden, 2016); physical health, such as injury and cardiovascular changes (Family Caregiver Alliance, 2006); and emotional health, such as depression, anxiety, and stress (Loh et al., 2017). Many studies have also measured caregiver burden or strain, defined as caregivers’ perception of the adverse effects of caregiving on themselves (Zarit et al., 1980). Caregiver burden for the caregiver of a person who has had a stroke is greater if the care recipient has depression, cognitive deficits, poor mobility, aphasia, upper extremity spasticity, dysphagia, or behavioral issues—all common challenges after stroke (Hildebrand, 2021). Zhu and Jiang (2018) found that certain caregiver factors (depression, anxiety, ability to cope with stress) and care recipient factors (ability to perform ADLs, psychological health, anxiety) had large effect sizes on caregiver burden. When the caregiver has negative experiences caregiving and feels increased caregiver burden, adverse effects can be expected for the care recipient, including greater incidence of institutionalization, more frequent and longer hospital stays, and poorer outcomes (Bakas et al., 2014). Because of the potential negative impact of caregiving on both the caregiver and the care recipient, medical professionals must identify interventions that will prevent or mitigate adverse effects and sustain the caregiver’s ability to provide quality care.
The American Heart Association–American Stroke Association (AHA–ASA) guidelines for adult stroke rehabilitation state that the caregiver is an integral member of the stroke rehabilitation team; they recommend that the caregiver receive education about stroke impairments, secondary conditions, interventions, and community resources throughout the continuum of care (Winstein et al., 2016). Stroke guidelines also recommend that caregivers receive social and family caregiver support through education, training, counseling, development of a support structure, financial assistance, and involvement in all decision making throughout the rehabilitation process (Winstein et al., 2016). Caregivers are seen as essential members of the care team in occupational therapy practice, as well. The Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association [AOTA], 2020) states that active participation from both the caregiver and the care recipient makes caregiving a co-occupation, and outcomes, such as quality of life, should also be designed for caregivers.
Given the needs of clients who have had a stroke and their caregivers, the mandate from the AHA–ASA guidelines to include caregivers in rehabilitation, and AOTA’s call to address outcomes for caregivers, we conducted this systematic review to explore the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people who have had a stroke that facilitate maintaining participation in the caregiver role.
Method
This narrative synthesis systematic review is one of four in a series of stroke reviews supported by the AOTA Evidence-Based Practice (EBP) Program. This review was conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and aligned with both the protocol established by the EBP Program, with input from external stakeholders and experts, for stroke reviews and the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA) guidelines (Moher et al., 2009). The process of the review was a collaborative effort that included AOTA staff, the review authors, a medical librarian, and a research methodologist. We used the following research question for this review: “What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people with stroke to facilitate maintaining their participation in the caregiver role?”
Eligibility Criteria
Studies included were peer-reviewed intervention studies published in English between January 1999 and December 2019 and rated as Levels 1b and 2b evidence on the basis of the Oxford Centre for Evidence-Based Medicine (2009). Other inclusion criteria were that the article described intervention research within the scope of occupational therapy practice (no additional licensure or degree needed) and that the research participants were adult caregivers (age >18 yr) of a person who had a stroke. We included studies that used caregiver outcome measures examining participation, quality of life, depression, anxiety, psychological well-being, burden, stress, or knowledge. We excluded all systematic reviews because of differences in their review inclusion criteria; however, we hand searched each systematic review individually for relevant cited articles that met our inclusion criteria.
Literature Search and Study Selection
The following databases were searched with terms established by the external advisors, AOTA staff, medical librarian, methodologist, and review authors: MEDLINE, PsycINFO, CINAHL, OTseeker, and Cochrane. The search terms are provided in Table A.1 of the Supplemental Appendix (available online with this article at https://research.aota.org/ajot). The literature search results were collected, duplicates were removed, and the remaining results were exported in EndNote format by the medical librarian working on the project. The methodologist for the project did a title review of the search results, eliminating articles that clearly did not meet the inclusion criteria (wrong year, not caregiver, not stroke, not an intervention study). These results were then exported to the review authors in three formats—Endnote, Microsoft Word, and tab-delimited. A search in OTseeker was completed by the medical librarian, and citations from this search were delivered to the authors in Word format.
The two authors and three graduate assistants reviewed abstracts to determine which full articles would be reviewed. Because systematic reviews were not included, one graduate assistant also hand-searched them to identify cited articles that met the inclusion criteria and entered these citations in a master citation table for further review. After the abstract review, the full-text articles were retrieved and reviewed as a team by the two authors. The decision to include or exclude was listed in the master citation table, and final articles included in the review were abstracted in an evidence table (Table A.2 in the Supplemental Appendix). Both tables were reviewed for quality control by AOTA staff and the research methodologist. The authors conducted the final screening, and nine disagreements between them were resolved by consensus.
Data Extraction and Analysis
The authors determined the risk of bias for each article using the Cochrane Risk of Bias Guidelines for controlled trials (Higgins et al., 2019). The authors then conducted a narrative synthesis with oversight provided by AOTA staff members. The articles were grouped by relevant thematic groups, and strength or certainty of the evidence was evaluated using the U.S. Preventive Services Task Force’s (2018) level of certainty evaluation criteria. This evaluation includes the number, level, and quality of the studies in each thematic grouping. The results of this evaluation provide an overall strength of evidence for the thematic groups as strong, moderate, or low (U.S. Preventive Services Task Force, 2018). For all study findings, benefits and harms were considered.
Results
The database search yielded 4,204 articles for review from five databases; an additional 32 articles were identified from hand-searching reference lists of articles included in the original search (Figure 1). Of those articles, a total of 33 were included in the final synthesis. Four articles that met the inclusion criteria were follow-ups to previous studies (Mant et al., 2005; Shyu et al., 2010; van den Heuvel et al., 2002; Zhou et al., 2019). These articles were combined with the primary study (Mant et al., 2000; Peng et al., 2019; Shyu et al., 2008; van den Heuvel et al., 2000) for purposes of analysis. Thus, a total of 29 studies reported in 33 articles were left for data extraction and analysis. Twenty of the studies were Level 1b evidence (well- designed randomized controlled trials [RCTs]), and 9 were Level 2b evidence (lower quality RCTs or two-group nonrandomized studies). Overall risk of bias for each study is included in Table A.3 in the Supplemental Appendix. In this review, none of the studies resulted in harm or had a risk of harm to the participants. Many of the studies examined outcomes for both caregivers and people with stroke; however, for this review, data extraction focused exclusively on the studies’ caregiver outcomes.
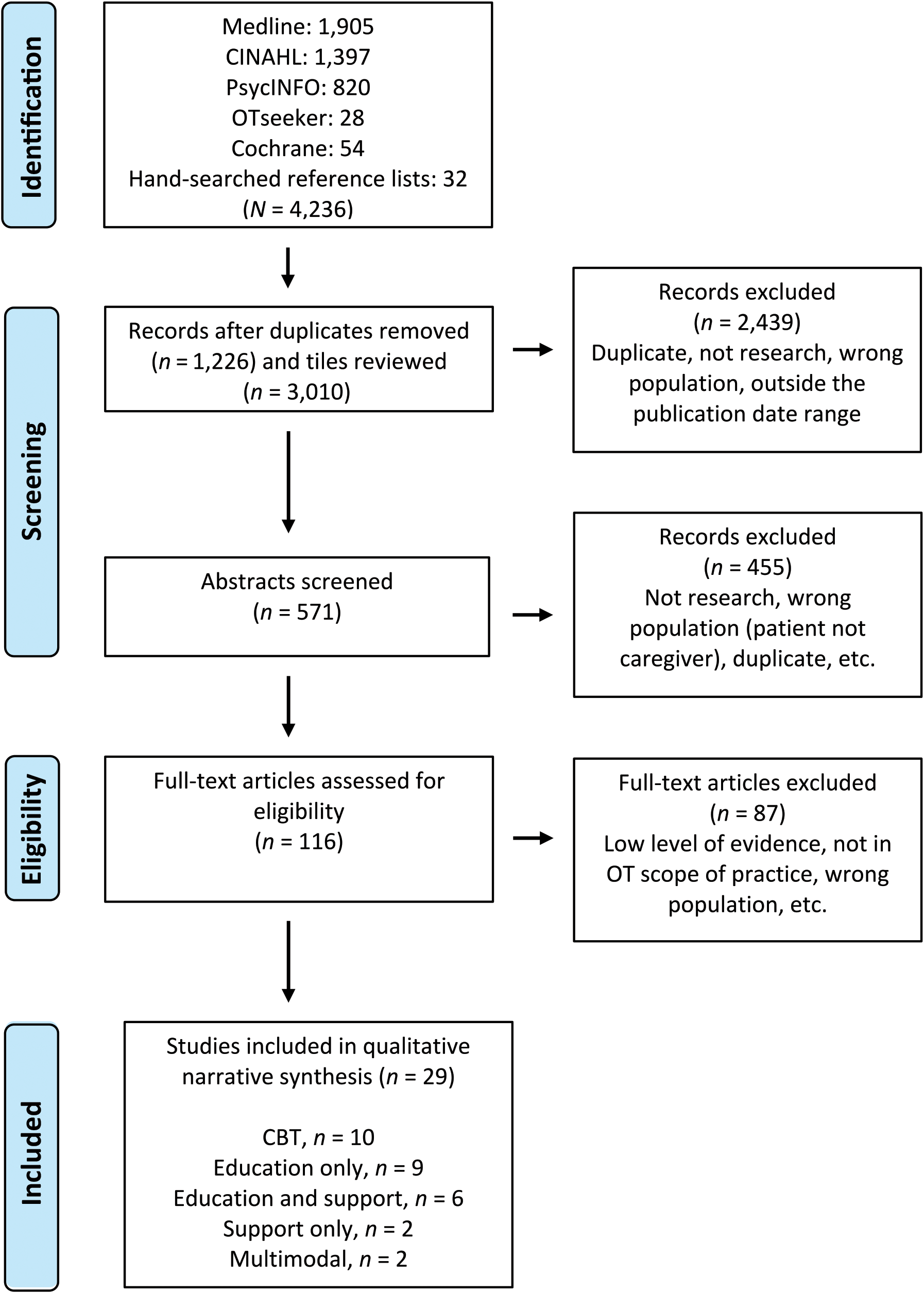
Flow diagram for inclusion and exclusion of studies in the systematic review.
Narrative Synthesis
The included articles were analyzed for themes by the authors, and five themes based on intervention type were mutually agreed upon: cognitive–behavioral therapy (CBT) techniques, caregiver education only, caregiver support only, caregiver education and support, and multimodal interventions. It is important to note that for the education-only and education and support themes, we examined only Level 1b studies because of the large number of studies that met the inclusion criteria at this level of study design. For the other three themes—CBT techniques, caregiver support only, and multimodal interventions—both Level 1b and 2b studies were included in the final data extraction and analysis (Table A.4 in the Supplemental Appendix summarizes the number of studies at each level of evidence by theme).
Cognitive–Behavioral Therapy Techniques
Five Level 1b RCTs and 5 Level 2b RCTs met the inclusion criteria. The risk of bias for these studies ranged from medium to high (see Table A.2). These studies were placed under the larger umbrella of CBT techniques and were further divided into the subthemes of problem-solving only, CBT techniques only (not including problem-solving), problem-solving and CBT techniques combined, and problem-solving and stroke education combined. Studies using problem-solving defined it as a method of managing stress by assisting the caregiver to identify problems, generate solutions, and implement solutions as a constructive coping strategy or to build self-efficacy (Grant, 1999; Grant et al., 2002; King et al., 2012; Pfeiffer et al., 2014).
Problem-Solving Only
There is moderate strength of evidence for teaching problem-solving only to caregivers of people with stroke. Two Level 2b studies provided problem-solving instruction, and the intervention groups had statistically significant improvements compared with the control groups (Grant, 1999; Grant et al., 2002). Problem-solving instruction led to significantly better problem-solving skills and preparedness among intervention group caregivers when training was delivered in a 3-hr inpatient session and telephone follow-up sessions (Grant, 1999) and when taught in a 3-hr in-home session with telephone follow-up sessions (Grant et al., 2002).
Cognitive–Behavioral Therapy Techniques Only
There is low strength of evidence for the use of CBT techniques that did not include problem-solving. In a Level 2b study, Robinson-Smith et al. (2016) coached caregiver–care recipient dyads over six home visits in cognitive reframing, a stress reduction strategy that emphasizes recognizing accomplishments and gains and using self-encouragement to continue working on goals for recovery. This resulted in a significant positive effect on dyadic coping for the intervention group compared with the control group, but no differences in depression or quality of life.
Problem-Solving and Other Cognitive–Behavioral Therapy Techniques Combined
Two Level 1b studies (King et al., 2012 ; Pfeiffer et al., 2014) and 1 Level 2b study (King et al., 2007) met the inclusion criteria and provide strong strength of evidence to support a combination of problem-solving interventions and other CBT techniques.
In a combination of in-home visits and telephone sessions for up to 12 mo, the intervention group in the Pfeiffer et al. (2014) study received problem-solving training and other CBT techniques such as role- playing, modeling, shaping, reinforcement, and cognitive restructuring. This study found that the intervention group had significantly lower levels of depression, fewer physical complaints, and higher satisfaction with leisure than the control group. In two separate studies, King et al. (2007, 2012) provided problem-solving training and other CBT techniques such as relaxation training, cognitive reframing, or mood rating via three in-person inpatient sessions and then telephone calls over 3 mo. The intervention groups had significantly improved depression, life changes, and health (King et al., 2012) and significantly lower severity and rate of depression (King et al., 2007) compared with the control groups in each study.
Problem-Solving and Stroke Education Combined
Three Level 1b studies (Cheng et al., 2018; Deyhoul et al., 2020; Perrin et al., 2010) and 1 Level 2b study (Bishop et al., 2014) met the inclusion criteria and provide strong strength of evidence to support interventions with a combination of problem-solving and stroke education for caregivers of people with stroke.
Cheng et al. (2018) began with two inpatient sessions of stroke education and then provided biweekly problem-solving training by telephone for 3 mo. Caregivers in the intervention group had statistically significant improved competence, problem-solving and coping abilities, and satisfaction with social support and lower caregiver burden than the control group. Deyhoul et al. (2020) provided four inpatient sessions consisting of three stroke education and training sessions and one problem-solving training session. Caregiver burden was found to be statistically significantly lower in the intervention group compared with the control group. Perrin et al. (2010) also provided stroke education before discharge and problem-solving training via videophone for 4 wk. Caregivers in the treatment group had statistically significant lower caregiver strain than those in the control group. A pilot study by Bishop et al. (2014) consisted of providing stroke education and information and biweekly telephone sessions to provide problem-solving intervention for 6 mo after discharge. Caregivers in the intervention group had statistically significant better scores on family functioning, functional independence, and criticism of self when compared with the control group.
Caregiver Education Only
Nine Level 1b studies from 11 articles related to caregiver education interventions met the inclusion criteria, ranging from low to medium risk of bias (see Table A.2). Education included topics such as stroke information, skills training (e.g., transfers or ADLs), or community resource information. Subthemes describing the mode or method of education delivery were extracted from the data: in-person education, a hybrid or combination of in-person and remote education, and remote education only.
In-Person Education
Four Level 1b studies provide low strength of evidence because of mixed results for interventions that consisted of in-person education only. One study (Kalra et al., 2004) provided education before discharge and a home visit after discharge and found statistically significant improvements in some outcomes, including caregiver burden, quality of life, and anxiety and depression. Rodgers et al. (1999) found that an in-person group education program had mixed results, with positive outcomes for stroke knowledge but negative outcomes for social functioning. Two RCTs provided education and training before inpatient discharge only but found no significant benefits for the caregivers (Forster et al., 2013; Smith et al., 2004).
Hybrid or Combination of In-Person and Remote Education
Three Level 1b studies in five articles examined the effects of caregiver education delivered in a combination of in-person and remote methods (i.e., telephone, mail, or videophone; Kuo et al., 2016; Peng et al., 2019; Shyu et al., 2008, 2010; Zhou et al., 2019). These studies provide low strength of evidence to support this method of education delivery and ranged from low to medium risk of bias. Kuo et al. (2016) held an in-home oral care education session and telephone- or mail-delivered education and found a significant improvement in oral care knowledge, self-efficacy, and behavior. Shyu et al. (2008, 2010) provided inpatient education and in-home and telephone visits after discharge and found statistically significant improvements in caregiver preparation scores, caregiver social functioning at 3 mo, and quality of care provided at 6 mo, but no statistically significant results in other outcomes. Peng et al. (2019) and Zhou et al. (2019) reported that they found no statistically significant differences between the intervention and control caregiver groups after providing education and training in the inpatient setting with telephone or videophone follow-up sessions.
Remote Education Only
There is low strength of evidence to support delivering caregiver education only by remote methods such as the telephone or Web. Two Level 1b RCTs with low and medium risk of bias were included in this subtheme. One study found significant improvements in caregiver depression only by delivering education by telephone (Bakas et al., 2015). Pierce et al. (2009) found no statistically significant improvements in any outcome when they provided self-directed, Web-based education about stroke and caregiving.
Caregiver Support Only
There is low strength of evidence because of mixed results from 2 Level 2b studies that examined caregiver support only with no additional intervention methods. Mei et al. (2018) studied the effects of a modified reminiscence group on caregivers, and Yilmaz et al. (2019) provided progressive muscle relaxation training to caregivers. Mei et al. (2018) found statistically significant improvements in the intervention group compared with the control group in positive experience, life satisfaction, and caregiver burden. Yilmaz et al. (2019) found no significant differences between the intervention and control groups on any outcomes.
Caregiver Education and Support
Six Level 1b studies reported in seven articles, ranging from low to high risk of bias, provided moderate strength of evidence for combining caregiver education and support. Three studies used support groups (Draper et al., 2007; Hartke & King, 2003; Larson et al., 2005), and 3 studies provided individual education and support (Lincoln et al., 2003; Mant et al., 2000, 2005; Ostwald et al., 2014).
Education and Support in Group Interventions
There was low strength of evidence because of mixed results for providing caregivers education and support in a group. Hartke and King (2003) examined the use of a telephone support group in which educational materials were provided and stress management relaxation techniques were taught. They found significant improvement in caregiver sense of competence and burden in the intervention compared with the control group. Draper et al. (2007) and Larson et al. (2005) conducted in-person support groups and provided education on skills, communication strategies, and community services plus support for the caregiver, such as relaxation and managing emotions. They found significant improvements in psychological distress for the intervention group. Larson et al. (2005) examined in-person group sessions that addressed stroke information, recovery, and prevention and the psychological and social effects of stroke. They found no significant differences between the intervention and control groups.
Education and Support in Individual Interventions
There was strong strength of evidence for providing caregivers with individual education and support interventions. Individual education and support were provided to caregivers in two studies that used a family support organizer (FSO; Lincoln et al., 2003; Mant et al., 2000, 2005). In both studies, the FSO provided education and support before discharge, at home, and by telephone and acted as a liaison with other services. Mant et al. (2000) found significant improvement in the intervention group in social activity level and quality of life at 6 mo poststroke, but not at 12 mo (Mant et al., 2005). The FSO in the study by Lincoln et al. (2003) provided information, assisted with case conferences and discharge, and conducted home visits. They found statistically significant improvement in caregiver knowledge only. Ostwald et al. (2014) provided stroke information, skills training, coping strategies, and community resources and found statistically significant improvements in the intervention group’s self- reported caregiver health status and ability to acquire social support.
Multimodal Interventions
Two Level 2b RCTs reported in three articles implemented multimodal interventions for caregivers; had moderate and high risk of bias, respectively; and provided moderate strength of evidence for this approach. These studies included a combination of at least three types of interventions that have previously been discussed, such as education, training, problem-solving, CBT techniques, and support. Van den Heuvel et al. (2000, 2002) examined the results of an intervention that provided ADL training, community resources education, written stroke information, problem-solving, coping strategies, and caregiver counseling. Two intervention groups received the same interventions but in two venues: in a group setting or in their homes. No significant differences were found between the two intervention groups, but when compared with the control groups, the combined intervention groups had significantly better confidence and increased use of coping strategies and amount of social support.
Wilz and Barskova (2007) conducted group sessions over 8 mo in which they provided stroke education and rehabilitation information, cognitive restructuring, problem-solving, relaxation techniques, and professional support. The intervention group had significantly better psychological, social, and environmental quality of life and decreased depression levels than the control group.
Discussion
This systematic review evaluated the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people who have had a stroke, with the goal of helping caregivers maintain participation in the caregiver role. Twenty Level 1b studies evaluating interventions within the scope of practice over the past 20 yr demonstrate that occupational therapy has a well-supported role with this population. In total, the evidence provides strong support for occupational therapy practitioners to provide meaningful interventions to this population, although the strength of evidence for the effectiveness of individual intervention techniques and approaches varied.
Problem-solving training emerged as providing strong strength of evidence and the best outcomes for caregivers, particularly when paired with stroke education. This is a logical combination, because before problem-solving interventions are provided, caregivers need education about stroke to understand the problems that they may need to solve. Moreover, problem-solving alone and in combination with other CBT approaches had moderate strength of evidence. According to a 2015 survey of therapists who worked with caregivers of people with stroke (Lawson et al., 2015), all therapists provided education and training to caregivers, yet only 50% of occupational therapists addressed problem-solving skills, and 72% addressed cognitive strategies across all practice settings. A greater number of occupational therapy practitioners should add problem-solving training and CBT techniques to the caregiver education they currently provide. This is further supported by a systematic review conducted by Panzeri et al. (2019), who found that psychologist and nursing interventions that included CBT, problem-solving training, and coping skills training significantly improved depression, anxiety, caregiver burden, well-being, and social support among caregivers of people with stroke.
Interventions using a combination of individual support and education for the caregiver also provided strong strength of evidence, and those providing caregiver support and education in groups had moderate strength of evidence. This suggests that working one-on-one with the caregiver and providing personalized interaction rather than performing an intervention that is solely group based or self-directed has better outcomes. Occupational therapy practitioners primarily provide face-to-face, one-on-one education when working with caregivers of people who have had a stroke, but few address the support needs of caregivers, with only 46% referring caregivers to support groups, 29% addressing stress management, and 14% addressing financial management (Lawson et al., 2015).
Most of the studies examined for this systematic review used a variety of intervention components. This is also a logical approach: Caregivers have numerous needs, and there are multiple approaches and theories from which to draw. Occupational therapy practitioners must provide multipronged intervention approaches over time. Caregivers of people who have had a stroke may require a package of services, including information, skills training, support, cognitive strategies, or problem-solving training. The Family Caregiver Alliance (2006) has recommended that health professionals perform a comprehensive assessment tailored to each caregiver in multiple domains (e.g., assessments of context, values, well-being, skills, knowledge, potential resources). Thus, thorough assessment of caregivers before initiating intervention is essential to ensure that practitioners align the intervention with each caregiver’s individual requirements.
It is noteworthy that there was no consistent length of intervention (weeks to months) or mode of delivery (in-person, telephone calls, etc.) across studies. Studies that provided interventions only in person before discharge from an inpatient setting tended not to have many significant outcomes, whereas studies that provided interventions postdischarge or both pre- and postdischarge yielded better results. Lawson et al. (2015) found that across disciplines, therapists provided only about 45 to 60 min of intervention to caregivers in total. In contrast, Cameron and Gignac’s (2008) Timing It Right intervention framework for caregivers of stroke survivors identifies specific caregiver needs that should be addressed at each phase poststroke, from the initial diagnosis and acute hospitalization to adaptation at home. To address these specific and changing needs over time, practitioners should advocate for policy and payment changes that would allow for the delivery of occupational therapy interventions for more time over a longer period, thus supporting the caregiver and providing training opportunities to revisit and practice skills as needs arise, particularly after discharge home.
Many studies combined multiple delivery modes (inpatient sessions, follow-up in-home visits, regular telephone calls over weeks and months after discharge). In-person intervention did not always result in the best outcomes. In fact, a combination of in-person and remote contact over time (most often via telephone) had better outcomes. This may in part be a result of competing demands on the caregiver’s time and energy that limit their ability to fully participate in in-person sessions. Caregivers of adults reported spending an average of 17 hr per week doing caregiving tasks, and those who performed more complex tasks reported spending twice as much time in the caregiving role (Reinhard et al., 2019). This large time requirement may leave limited opportunity for participation in outside activities, especially if participation requires a commute or finding caregiving coverage from another person. Therefore, practitioners should consider which intervention delivery modes meet the needs of caregivers and should, moreover, consider providing at least some of the intervention remotely after discharge, if appropriate.
Limitations
As with all systematic reviews, there are limitations that should be taken into consideration. Studies that were not published in English were not included in this review, potentially affecting the strength of evidence and creation of themes, subthemes, and conclusions. Most studies included multiple types of interventions, multiple delivery modes, and variable length of intervention delivery, which affects the ability to draw conclusions about specific aspects of each intervention. The risk of bias for the majority of the studies was moderate, with many studies using self-reported outcomes, leading to decreased strength of evidence. There is also the possibility that relevant articles that met the inclusion criteria were inadvertently missed. Finally, most of the included studies were not conducted by occupational therapy practitioners, although the interventions fall within the scope of occupational therapy. This may limit the generalizability of the findings to occupational therapy practice.
Future Considerations and Implications for Occupational Therapy Practice
Further research is necessary with respect to the various modes of intervention, the appropriate length of time, and intervention dosage to determine best practice. Given the multicomponent design of many of the studies, it was difficult to determine the active ingredient that produced improvements among caregivers. Further research is needed to determine which aspects of the interventions result in improvements in caregivers’ ability to continue in the caregiving role, but it is clear from this systematic review that education alone is not sufficient.
Although the interventions fall within the scope of occupational therapy practice, most of them were delivered by other health professionals, with only a few including occupational therapy. To improve generalizability of research for use by occupational therapy practitioners, they must be involved in the research. Moreover, occupational therapy practitioners should measure an intervention’s effect on caregivers’ participation and occupational performance instead of impairments (e.g., depression, burden).
Finally, occupational therapy practitioners and advocacy organizations must work to advance policy and payment systems to support the delivery of interventions to caregivers and stroke survivors over a longer period of time postdischarge and using nontraditional delivery models and settings.
Conclusion
Caregiving is a complex and demanding role that may create physical, mental, social, and financial strain among caregivers of people who have had a stroke (Collinson & De La Torre, 2017; Loh et al., 2017; NAC & AARP Public Policy Institute, 2015; Schulz & Eden, 2016). The literature addressing interventions for caregivers of people with stroke supports the role of occupational therapy in helping caregivers maintain participation in the caregiving role. Despite varying strengths of evidence, occupational therapy practitioners should use problem-solving interventions, CBT, education and training, and support interventions or a combination of these approaches with caregivers. The interventions should be provided before discharge, in person in a health care setting, in the home, and remotely, for example, by telephone. Future studies must examine specific approaches, settings, and timelines to provide empirical evidence that will inform occupational therapy interventions for caregivers.
Supplemental Material
Supplementary material for Interventions for Caregivers of People Who Have Had a Stroke: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050012.pdf for Interventions for Caregivers of People Who Have Had a Stroke: A Systematic Review by Amanda Mack and Mary Hildebrand in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
This review was registered with PRISMA (CDR42020161214).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.