
Abstract
The Adaptive Care program is an example of occupational therapy practitioners and other interprofessional team members adapting physical and social health care environments to support the mental health needs of autistic children.
The hospital environment is a threat to autistic children’s mental health. Key characteristics of autism spectrum disorder (ASD), including communication and sensory differences and requiring predictable routines, are often in conflict with the hospital environment that includes loud noises; bright lights; overwhelming interactions with people; and novel, often noxious, experiences (Walsh et al., 2020; Wilson & Peterson, 2018). The conflict between the child’s needs and the environment can lead to anxiety, aggression, self-injury, or other manifestations of distress (Johnson et al., 2014; Neil et al., 2016). Pain, limited sleep, and other physical health concerns can compound behaviors that hospital staff interpret as challenging (Crabtree & Demchak, 2011; Johnson et al., 2014; Walsh et al., 2020). Focused on medical procedures, the hospital is often an inflexible place that does not adapt to the needs of autistic patients or those with other developmental disabilities (Walsh et al., 2020). For example, physical restraint remains a common strategy with autistic patients in the hospital, although intended as a last resort to keep patients safe from self-harm (Salvatore et al., 2021). Autistic children’s parents have reported that hospitals are such noxious environments that they need to carefully weigh the benefits and risks of taking their children to the hospital, even in emergency situations (Davignon et al., 2014; Nicholas et al., 2016).
Health care providers are the primary social environment that can positively or negatively influence children’s hospital experiences and related mental health. For example, health care providers interpreting autistic children’s anxiety or fear as challenging behavior led to negative experiences for children, such as sedation or physical restraint (Kouo et al., 2021). Parents noted improved hospital experiences when health care providers used strategies to engage with autistic children (Wilson & Peterson, 2018). Health care providers report needing additional strategies and support to effectively care for autistic children because of limited knowledge, self-efficacy, and comfort working with this population (Walsh et al., 2020). Enabling health care providers to support autistic children in the hospital may result in positive outcomes for the health care providers and the children (Kouo et al., 2021; Walsh et al., 2020 ; Wilson & Peterson, 2018).
Environmental interventions to enhance how health care providers interact with autistic children and their families can address systemic problems with hospital care for this population. Key factors to enhance health care for autistic children and those with other developmental disabilities include gathering information from family to inform care, adapting communication and sensory strategies to the child’s needs, and ensuring systems for interprofessional collaboration (Nicholas et al., 2020; Wilson & Peterson, 2018). Specific recommendations include identifying patients who require additional support, efficiently gathering key information from families, and individualizing strategies to meet a child’s needs (Samet & Luterman, 2019; Thom et al., 2020). Although framed as enhancing health care and supporting health care providers, these strategies also support the mental health needs of autistic children.
Few studies have evaluated the effects of adapting the health care social environment to address autistic children’s needs (Lucarelli et al., 2018; Mazurek et al., 2020; Wood et al., 2019). These studies included primary care providers, emergency department staff, and outpatient frontline staff and measured staff knowledge, comfort, and self-efficacy in working with autistic children. Among these few intervention effectiveness studies, none studied inpatient hospital environments or nursing staff; moreover, only Wood et al. (2019) included an occupational therapy practitioner as a program team member.
Occupational therapy practitioners can be valuable team members to ensure supportive hospital environments. Occupational therapy mental health promotion with autistic children involves decreasing the stress of the environment (Crabtree & Demchak, 2011). Occupational therapy practitioners can adapt the physical and social environment to match autistic children’s needs and to support mental health in the hospital.
This article describes the impact on nursing staff’s perceptions of an interprofessional environmental intervention designed to support mental health and enhance hospital care for autistic children and those with other developmental disabilities. Occupational therapy practitioners were interprofessional team members, and nursing staff were the first recipients of the Adaptive Care training and resources. The program focused on adapting the physical and social environments to the child’s needs (i.e., adapting care to the child; thus, “adaptive care”). The ultimate goal of the program was to enhance autistic patients’ hospital experiences by supporting the children’s mental health. An intermediary goal was to support nursing staff, who spend the most time with children in the hospital, by ensuring they had the knowledge and resources to support autistic children. This study was used to evaluate the impact of the environmental intervention program on the nursing staff’s knowledge, effectiveness, strategy use, and confidence.
Method
This study used a quasi-experimental, pretest–posttest design to assess the impact of an Adaptive Care program on nursing staff’s perceptions of caring for autistic children in the hospital. Both the hospital and the university institutional review boards approved the study before data collection.
Setting and Participants
The setting for this study was a large pediatric hospital with two campuses in a Midwestern U.S. metropolitan area. Nursing staff, including nurses and nursing aides, with direct patient care in the hospital were included in this study. Researchers invited potential participants to complete the pretest and posttest surveys through emails, staff meeting announcements, flyers, and word of mouth.
Instrument
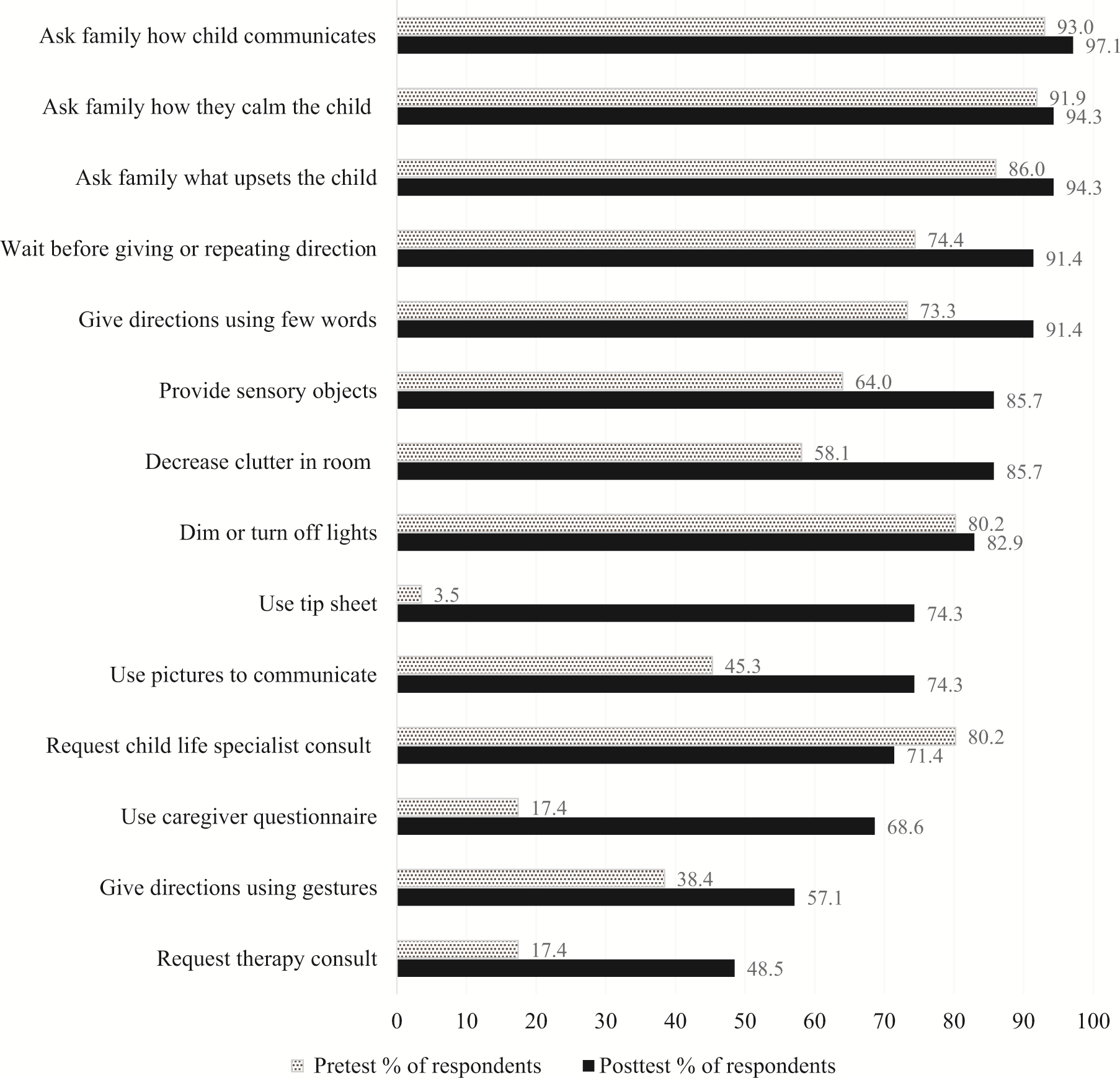
A researcher-developed, pilot-tested electronic survey was the primary outcome measure. Researchers adapted survey items on the basis of published research (Clark et al., 2016; McGonigle et al., 2014). To pilot test and validate the survey, researchers recruited pediatric nurses through online message boards and made minor revisions based on feedback and clarity ratings from 18 participants before the pretest (Mahoney et al., 2021). The final survey consisted of five sections, including demographics (8 items), knowledge (8 items), effectiveness (8 items), training and strategies (8 items), and confidence in implementing strategies from the Adaptive Care program (5 items). Although this article uses identity-first language, the survey language refers to “children with autism,” which included children with ASD or those with similar sensory, communication, or behavioral needs. Table 1 lists survey item examples. The survey provides 14 strategies nursing staff may use in the hospital and an open-ended option to specify additional strategies (Figure 1).
Reported strategies.
Knowledge, Effectiveness, and Confidence
Note. NA = not applicable.
Knowledge scale: 5 = strongly agree, 4 = agree, 3 = not sure, 2 = disagree, 1 = strongly disagree. Strongly agree and agree scored accurate for true statements. Disagree and strongly disagree scored accurate for false statements.
Effectiveness and confidence scales: 5 = strongly agree, 4 = agree, 3 = neither agree nor disagree, 2 = disagree, 1 = strongly disagree.
Confidence making Adaptive Care referral added to posttest; referral process did not exist when pretest was launched. This item was excluded from comparison statistics because there was no pretest score.
Adaptive Care Program
The Adaptive Care program was a quality-enhancement project that began on the basis of feedback from the parent of an autistic child who received services at the hospital. The program, consisting of staff training and resources, had two primary goals: enhance autistic children’s hospital experience and ensure hospital staff have sufficient means to support autistic patients’ mental health needs. Hospital administrators formed an interdisciplinary team to develop and implement the program; early and ongoing administrative commitment ensured program sustainability.
Team members included occupational therapy practitioners, speech-language pathologists, physicians, nurses, child life specialists, and behavioral therapists working at the hospital. Occupational therapy contributions centered on environmental modifications, sensory needs, and ensuring the program allowed for individualization based on each child’s needs. The interprofessional team collaboration was a key aspect of the program to such an extent that the team developed a tagline “Many hands working together” to describe the program. Although navigating the logistics of interprofessional team collaboration was challenging, it was essential for program implementation feasibility and sustainability. The program development process occurred over several years with the pretest completed in collaboration with a university partner serving as the final stage of the needs assessment process. Nursing staff were the first recipients of the training aspect of the program because they are the health care providers who spend the most time with children in the hospital.
The interprofessional team developed training on the new program in a variety of formats: (1) 6-hr, in-person training that used a train-the-trainer approach in February and March 2019 (one at each hospital location); (2) 1-hr overview presentation during a large staff meeting in March 2019; (3) 15-min orientation to the program from March to June 2019 led by nursing staff who completed the 6-hr training; and (4) online, asynchronous orientation training module from April to June 2019. Participants were included in the posttest if they completed any one training option, because each presented similar information with varying depth. The 6-hr session, the most extensive training, was led by an Adaptive Care team that included occupational therapy. On the basis of input from hospital administration, the 6-hr training used a train-the-trainer approach so that those who completed this training shared their knowledge with nursing colleagues through the 15-min overview sessions. These two formats (6-hr train-the-trainer and nurse trainer–led 15-min orientations) were the primary training methods for the new program. The Adaptive Care team was available for ongoing consultation. Topics covered in the trainings included (1) information about ASD, (2) communication strategies, (3) sensory needs and strategies, (4) who qualifies for Adaptive Care, (5) Adaptive Care resources, and (6) Adaptive Care referral process. All training except the 15-min orientation included at least one case example.
Adaptive Care program resources available at nursing stations included caregiver information sheets, sensory and communication tools for the child, and interprofessional communication tools. Resource development occurred over time with changes made on the basis of user feedback. For example, the team developed a “
Procedures and Analysis
The pretest survey was available from July to September 2018, and the posttest survey was available from June to October 2019. Survey responses were collected via research electronic data capture (REDCap), an online survey management system (Harris et al., 2009). Researchers included incomplete surveys if respondents completed more than demographic questions.
Researchers used Microsoft Excel 2016 for descriptive statistics. To describe knowledge results, researchers converted data to accurate–inaccurate responses (with unsure coded as inaccurate) and calculated accuracy percentages (see Table 1 note). Researchers used IBM SPSS Statistics (Version 27) for comparison statistics. Researchers matched pretest– posttest data on the basis of email addresses that respondents provided for paired comparisons using Wilcoxon signed rank comparison. Because of the small number of participants with paired comparisons, researchers also completed comparisons with Mann–Whitney U after removing pretest data for participants with paired comparisons to ensure independent groups. Before completing comparison statistics, researchers reversed the scale for false items on the knowledge scale for consistency across the scale; with this reversal, higher scores corresponded to more correct responses. Researchers used the IBM SPSS Statistics output to manually calculate effect sizes using the formula r = z/√N (with N = number of observations) and Cohen’s interpretation of effect sizes (small, r > .1; medium, r > .3; large, r > .5; Portney, 2020).
Results
Approximately 300 nursing staff received training on the Adaptive Care program from February to June 2019. Of these nurses and nursing care technicians, 107 met the inclusion criteria and provided program evaluation survey data: 90 completed the pretest survey, 35 completed the posttest survey, and 18 completed both the pretest and the posttest surveys for paired comparisons. To ensure independent group comparisons for Mann–Whitney U comparisons, researchers removed pretest data for the 18 participants, resulting in up to 72 participants in the pretest comparison group (demographic characteristics of the posttest participants can be found in Table 2). Most participants were registered nurses with extensive experience; the average experience in pediatric nursing was 8.1 yr (SD = 7.2; range = 0–≥20 yr).
Participant Demographic Characteristics
Multiple responses for training type(s) allowed (total more than 100%).
Participants exhibited accurate understanding of characteristics of ASD before and after program dissemination (see Table 1). Before the program, nursing staff with paired comparisons demonstrated 91.67% accurate knowledge of ASD; after training, this rate increased to an average of 95.14% accuracy. Although a trend was found toward improved knowledge, no considerable change occurred from pretest to posttest for those with paired comparisons or between independent groups (Table 3).
Pretest–Posttest Comparisons
Note. Researchers reversed false knowledge items (i.e., converted 1 to 5 and 2 to 4) for scale consistency before comparisons. Pretest n varied because incomplete surveys were included. Wilcoxon signed rank was used for the paired comparison; Mann–Whitney U was used for the independent group comparison. NA = not applicable; ns = not significant.
a Effect size.
Respondents reported increased effectiveness supporting autistic children’s mental health in the hospital after program implementation (paired comparison z = 2.99, p = .003; independent groups U = 65,502.5, z = −4.42, p < .001; see Tables 1 and 3). Nursing staff reported feeling more effective in understanding children’s communication and behavior, gathering and sharing information with autistic children, and calming autistic children. A small effect size was found in how much their effectiveness increased between pretest and posttest (paired comparison r = .18; independent groups r = .15; see Table 3).
Participants also reported increased confidence using Adaptive Care resources, such as picture supports, caregiver questions, and sensory objects (paired comparison z = −4.59, p < .001; independent groups U = 18,923.0, z = −3.85, p < .001; see Tables 1 and 3). A small to moderate effect size was found in how much nursing staff’s confidence increased between pretest and posttest (paired comparison r = .38; independent groups r = .18; see Table 3). During latter stages of program development, the Adaptive Care team created a referral process for nursing staff to request individualized resources; therefore, the team added a posttest question about confidence making a referral to Adaptive Care (see Table 1). Posttest participants felt moderately confident with the Adaptive Care referral process (M = 4.03, SD = 0.72).
Respondents reported using significantly more strategies to support autistic children’s mental health after program implementation (paired comparison z = −2.89, p = .005; independent groups U = 490.0, z = −4.90, p < .001; see Table 3). The effect size was moderately large (paired comparison r = .47; independent groups r = .48; see Table 3). More than 70% of posttest participants reported using 11 of the 14 Adaptive Care strategies (see Figure 1). Most posttest participants (n = 25 of 35; 71.4%) agreed that they had adequate tools and resources to work with autistic children in the hospital, with a moderate effect size among independent groups (U = 738.5, z = 3.30, p < .001; r = .33), although a statistically significant difference was not found for paired comparisons.
Discussion
The ultimate goal of the Adaptive Care program was to enhance autistic children’s hospital experiences by ensuring hospital staff had sufficient resources and training to support autistic patients’ mental health. This study focused on nursing staff knowledge, self- efficacy, confidence, and strategies as indicators of the initial impact of this environmental intervention. Although the nursing staff’s knowledge did not change after program implementation, it was relatively high before intervention. This finding is consistent with literature showing that health care providers with relatively high knowledge about ASD may still exhibit limited confidence or comfort supporting autistic children in health care settings (Mahoney et al., 2021; Mazurek et al., 2020).
The small improvement in nursing staff’s self-efficacy supporting autistic children is not unexpected soon after program implementation. It is promising that a statistically significant improvement was found in perceived effectiveness, and this outcome may continue to improve with opportunities to practice using Adaptive Care resources. Participants reported moderately increased confidence using aspects of the Adaptive Care program, a key focus of the trainings.
The largest impact of the Adaptive Care program implementation was the increased number of strategies that nursing staff reported using to care for autistic children in the hospital. Strategies specifically associated with the Adaptive Care program, such as the tip sheet and caregiver questionnaire, demonstrated large increases in reported use from pretest to posttest. The caregiver questionnaire was a resource that underwent substantial revision during program development on the basis of input from nursing staff. Adaptive Care strategies involve changes in the physical and social environments to support autistic children’s mental health.
The variety in training formats was both a strength and a limitation of this study. There were not enough participants to analyze differences across training formats, so the amount of training necessary to demonstrate effectiveness is unknown. Overall, participants demonstrated increased effectiveness, confidence, and strategy use after Adaptive Care program training and resource dissemination. The train-the-trainer approach emerged after negotiation with administration, who deemed that providing all-day training for everyone was unfeasible. Providing in-depth training to nurses to subsequently train coworkers had the potential added benefits of empowering nurses to implement the Adaptive Care program, reaching a broad audience across multiple shifts and expanding expertise supporting autistic children’s mental health. The combination of training formats resulted in approximately 300 nursing staff receiving Adaptive Care training over a few months.
Resources designed to support autistic children’s mental health improved nursing staff’s self-efficacy and confidence caring for this population. These intermediary outcomes may benefit nursing staff’s mental health. Previous research showed that fostering healthy patient relationships can support nursing staff’s mental health and job satisfaction (Walsh et al., 2020). Hospitals are stressful environments; thus, improving the social and physical environment may have a positive impact on the mental health of the autistic child, the child’s family, and the health care providers (Kouo et al., 2021; Walsh et al., 2020 ; Wilson & Peterson, 2018).
Health care providers are increasingly recognizing the value of adapting medical environments to meet the needs of autistic people and those with other developmental disabilities (Straus et al., 2019). Occupational therapy’s consideration of mental health promotion and environmental modification is ideally suited to such interventions.
Limitations
Although the overall response rate across the program evaluation was 35.67%, it was 11.67% for the posttest and only 6% for those who completed both the pretest and posttest. It is unknown how much the participants’ perceptions matched the perceptions of others who completed training or accessed resources. Although paired comparisons provide stronger evidence for program effectiveness, the small number led the researchers to also create and compare two independent groups at pretest and posttest. The similar results across both types of statistics provides additional support for program effectiveness. The pretest served as a needs assessment for the Adaptive Care program, and nursing staff appeared more invested in completing that survey (30% response rate). Future research may need to consider incentives for participation to encourage more responses.
The time between training and the posttest survey period was short, so participants had limited opportunity to use the Adaptive Care program before completing the survey. Participants’ ratings demonstrate the positive initial impact of the program. Although a longitudinal study could show potential long-term changes, it is unlikely to be feasible given the low response rate soon after the training.
In future studies, researchers may examine the effectiveness of program implementation through additional means, such as patient satisfaction surveys, gathering intervention perspectives of autistic children or their families, or tracking incident reports. Ongoing assessment may be helpful as environmental interventions are implemented with additional health care providers.
Implications for Occupational Therapy Practice
When applying the results of this study to practice, occupational therapy practitioners should consider the following factors: Key features to support autistic children’s mental health in the hospital were interprofessional program resources developed with feedback from users, training to introduce resources, and ongoing collaboration for individualized support. Team development and ensuring administrative support are essential for long-term sustainability. Multiple means of program dissemination may be necessary to support autistic children’s mental health in hospital settings. The train-the- trainer approach is feasible for interprofessional teams and may foster administrative commitment. Health care resources to support autistic children’s mental health must be practical and user friendly for health care providers. In the fast-paced hospital environment, resources need to be short, easy to use, and clearly connected to key issues for health care providers, such as supporting relationships with patients and providing quality medical care.
Conclusion
The need to support autistic children’s mental health in hospitals is well documented in the literature, although it is often framed in terms of enhancing health care. This article builds on the literature on how to adapt physical and social environments to address this need; in addition, it demonstrates how occupational therapy within an interprofessional team created systemic change within the hospital setting. This interprofessional program enhanced nursing staff’s perceived effectiveness, confidence, and strategies to support autistic children’s mental health in the hospital.
Footnotes
Acknowledgments
We thank Colleen Hammond, former registered nurse at Advocate Children’s Hospital, for research collaboration; Linda Schore, former Secretary II, Outpatient and Acute Pediatric Therapy at Advocate Children’s Hospital, for administrative assistance; Margaret Sompolski, OTR/L, Brittany Iwanski, OTR/L, and Alyssa Charman, OTR/L, occupational therapy graduates from Midwestern University, for assistance with survey development and pilot testing; Lindsey Shepardson and Paige Francis, occupational therapy students from Washington University, for research assistance; and Amy Stein, PhD, Midwestern University biostatistician, for initial statistical consultation. We also thank the Advocate Children’s Hospital Adaptive Care Program Committee for their collaborative work in designing and implementing the program.