
Abstract
This systematic review identifies and synthesizes existing research on the relationship between key areas of development and accessible play settings for children with disabilities to inform evidence-based interventions and advocacy work.
Currently, more than three million children in the United States live with a disability (Young & Crankshaw, 2021). The term disability has several definitions resulting from its varied use in medicine, law, and research. For example, the U.S. Census Bureau (2021) considers a person to have a disability if they have difficulty with hearing, vision, cognition, ambulation, self-care, or independence. Meanwhile, the World Health Organization (2021) does not characterize disability as a health condition on its own but rather as the result of a person with a health condition interacting in their personal and environmental contexts. Moreover, people with disabilities frequently experience human rights violations as a result of discrimination and access barriers. This is of particular concern for children with disabilities because environmental and societal constructs frequently restrict engagement and satisfaction (Missiuna & Pollock, 1991). The World Federation of Occupational Therapists (2019) maintains that people have the right to participate in occupations that enable them to flourish, thrive, and fulfill their potential, and any violation of this right is known as occupational injustice (Chichaya et al., 2020 ; Townsend & Wilcock, 2004). For children, play is a primary occupation affected by disability.
Play is a valuable occupation for children because it challenges their minds, stimulates their senses, and tests their muscular strength (Miller et al., 2017 ; Missiuna & Pollock, 1991). It involves decision making and peer interaction, provides insight into how to interact in social and environmental contexts, and aids in the development of cognitive and psychosocial skills. Risky play is particularly beneficial for childhood development. It is defined as a type of play that poses a risk of harm while providing an increased opportunity to engage in problem solving and exploration (Grady-Dominguez et al., 2021; Parker & Al-Maiyah, 2022). Playgrounds offer these valuable opportunities that facilitate motor, play, and social skills, but many are inaccessible to children with disabilities (Moore & Lynch, 2015; Sterman et al., 2019).
In 2010, the Civil Rights Division of the U.S. Department of Justice released the 2010 ADA Standards for Accessible Design. This comprehensive document describes standards that facilities must abide by to be considered accessible, and it is the primary policy dictating how public playgrounds are designed. Accordingly, past research has identified barriers to play, as well as how playground design can inhibit play participation for children with disabilities (Sterman et al., 2020). Engagement in meaningful childhood occupations is paramount to reaching developmental milestones, making occupational injustice a health issue for this population. This injustice in play equity concerns health advocates because playgrounds can hinder childhood development, independence, and freedom for a child with disabilities (Lynch et al., 2018). Occupational therapy practitioners and health care advocates seek to raise public awareness of these issues to facilitate societal change and promote occupational justice (Hocking, 2017).
Background Literature
Social participation is understood as a child’s ability to interact with their peers in their environment (Cosbey et al., 2012). Children who actively engage in social participation exhibit developmental growth in confidence, play, and communication with their peers (Fernelius & Christensen, 2017). Furthermore, physical engagement in play promotes development of necessary motor skills (Carlon et al., 2013). Children with disabilities, however, are often unable to fully engage in social participation as a result of barriers in playground structure and design (Fernelius & Christensen, 2017). The 2010 ADA Standards (U.S. Department of Justice, Civil Rights Division, 2010) outline standards for public play areas for children older than age 2 yr and establish how a play structure should be designed to be considered accessible. An accessible playground requires play components usable by children of all abilities to be integrated into a playground setting, including a transfer platform, ramp, and elevated play components (U.S. Department of Justice, Civil Rights Division, 2010). Despite these guidelines, in 2019, 65% of caregivers for children with disabilities reported that their child could not fully participate because of inadequate adaptations (Stanton-Chapman & Schmidt, 2019).
Physical accessibility is not the only barrier for children with disabilities (Umeda et al., 2017). For example, children with sensory processing disorder (SPD) struggle with modulating, identifying, and categorizing sensory information, which affects their ability to engage in social play (Crasta et al., 2020). In 2012, Cosbey et al. observed play behaviors between children with and without SPD on the playground. They identified differences in play behaviors between participants, such as increased conflict, lack of awareness of social cues, and increased secluded play for children with SPD. These concerns are not as easily addressed by the Americans With Disabilities Act of 1990 (Pub. L. 101-336) and remain hidden barriers to community engagement and accessibility for children with disabilities (Umeda et al., 2017).
Because occupational therapy is a client-centered profession, one of the occupational therapy practitioner’s roles is to advocate for their clients’ health needs. The Occupational Therapy Practice Framework (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020b) illuminates the breadth of advocacy possibilities through multiple practice areas, such as the organizational, community and population, and governmental and policy levels. Because children with disabilities face barriers in exercising their rights to play, the OTPF–4 provides examples of how occupational therapy practitioners can intervene as advocates when injustice is present. This is further supported by an official document put out by AOTA (2020a) on occupational therapy’s role in the promotion of health and well-being. This document, Occupational Therapy in the Promotion of Health and Well-Being, provides case examples, one of which describes an occupational therapy consultant hired to assist in the development of an accessible school playground. The occupational therapist’s role includes tasks such as surveying the proposed area, ensuring that requirements are met, and reporting recommendations for equipment and landscaping to ensure that the playground is not only accessible but also fun and engaging.
Currently, research on how accessible playgrounds affect key areas of childhood development for all children is limited. This has led to calls for increased occupational therapy advocacy for children’s play and accessibility of these spaces (Grady & Bundy, 2019; Romaniak et al., 2019; Umeda et al., 2017). Consequently, we conducted a systematic review to better understand the relationship between accessible playgrounds and cognition, behavior, motor skills, play skills, and social skills for children with disabilities. The objectives of this systematic review were to (1) identify and synthesize existing research on the relationship between key areas of childhood development and accessible play settings for children ages 3 to 12 yr with disabilities and (2) create a body of evidence for occupational therapy practitioners to use in advocating for occupational justice and informing evidence-based interventions within pediatric disability populations. For the purpose of this review, play settings include outdoor school and community playgrounds, parks, and play areas.
Method
This systematic review was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Studies were included if they were peer reviewed; written in English; published after 2012; set in a playground, play area, or park labeled as inclusive, accessible, or universal; included participants ages 3 to 12 yr with any disability; and had outcomes related to areas of childhood development, including cognition, social skills, motor skills, play skills, or behavior. Articles were excluded if they were not peer reviewed; written in a language other than English; published before 2012; a systematic review or meta-analysis; not set in a play setting labeled as inclusive, accessible, or universal; did not include any participants ages 3 to 12 yr with a disability; or had outcomes unrelated to areas of childhood development, as previously defined. This age group was selected because these children most commonly use play settings and are continually reaching developmental milestones (Flowers et al., 2019).
The initial research team, consisting of four reviewers (Kelsey Gately, Anna Zawadzki, Alyssia Mosley, and Alyssamarie Badua) completed database searches as a group on January 30, 2021, using Academic Search Complete/EBSCO, CINAHL/EBSCO, Education Research Complete/EBSCO, ERIC, OTseeker, and PubMed. The database searches included articles published from January 2012 to January 2021. The search strategy was developed to align with the Population, Intervention, Comparison group, and Outcome (PICO) model. The search strategy was adapted to meet formatting requirements for each given database’s search function but otherwise remained consistent. The following search strategy was used: (playground OR “play area” OR park) AND (inclusive OR accessible OR universal) AND (develop* OR play* OR social* OR cogni* OR behavior* OR motor*) AND (child* OR school-age OR student* OR adolescen* OR preschool*) AND (disab* OR disorder* OR impair* OR illness OR physical OR mental OR condition OR syndrome OR deficit OR autis* OR sensory* OR limit* OR blind* OR “developmental delay*” OR deaf* OR cerebral palsy OR spina bifida OR muscular dystrophy).
Articles were compiled from the database searches, and duplicates were removed. A total of four researchers (Gately, Zawadzki, Mosley, and Badua) were assigned articles. Two researchers were assigned to each article and independently completed the initial screening of assigned titles and abstracts. These researchers compared the screening results, and unresolved discrepancies were settled by a third independent reviewer, who was also a member of the initial research team. The third reviewer also screened the title and abstract in question, consistent with the two independent reviewers, and decided whether it should move forward to the full-text review. The full-text articles were then reassigned to the four researchers. Each article had two researchers assigned for an independent review of the full text. These researchers compared their results, and unresolved discrepancies were settled by a third independent reviewer who, consistent with the two independent reviewers, read the text in full.
This process was repeated for the extraction of specific variables for the evidence table (see Table A.1 in the Supplemental Appendix, available online with this article at https://research.aota.org/ajot). The following variables were extracted from each study included in the evidence table: author, year of publication, location, level of evidence and study design, participants, children’s disabilities, childhood development outcome measures, and results. The entire research term worked on variable extraction, and final entries were made by consensus. We assessed the studies’ level of evidence using the Oxford Center for Evidence-Based Medicine (2009) levels of evidence. To assess the risk of bias of the included studies, we used the Critical Appraisal Skills Programme (2019) Qualitative Research Checklist for qualitative studies and the National Heart, Lung, and Blood Institute (NHLBI, 2017) quality assessment tool for case–control studies and cross-sectional studies, respectively. Two researchers from the initial research team were assigned to each article and created a level-of-evidence table and assessed the risk of bias. These researchers compared results, and unresolved discrepancies were settled by a third independent reviewer, who assessed the level of evidence and risk of bias in the same fashion as the initial two independent reviewers.
The initial database search identified 561 articles (Figure 1). Of those, 174 duplicates were removed. Title and abstract screening resulted in an additional 322 articles being excluded. After the full-text review, 56 articles were removed on the basis of the exclusion criteria. Nine articles met the inclusion criteria and were included in this qualitative systematic review. Included studies were reviewed for variable extraction and level of evidence (Table A.1) and risk of bias (Tables A.2, A.3, A.4) using the aforementioned validated risk of bias tools.
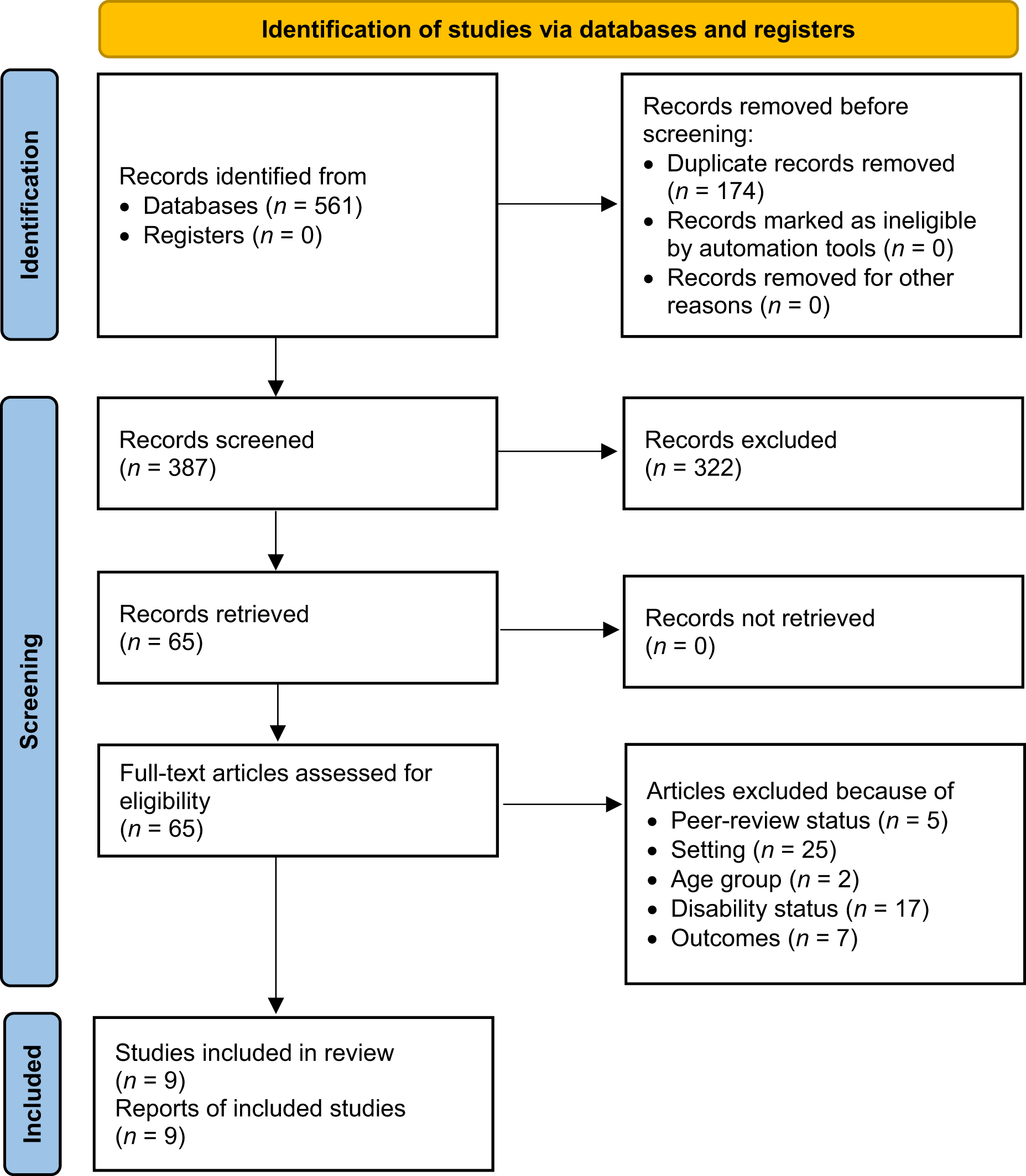
Flow diagram for the selection of studies for the systematic review.
Results
This systematic review assessed the literature on accessible playgrounds and areas of childhood development, including cognition, social skills, motor skills, play skills, and behavior. We were unable to identify articles that focused on behavior or cognition and met the remaining inclusion criteria. However, we were successful in identifying literature that explored social skills, play skills, and motor skills. Included studies primarily explored these areas of childhood development through the lens of access and engagement. As such, the results were analyzed and divided into three categories on the basis of the outcome measures used in the included articles as they relate to social participation, play participation, and motor skills.
Social Participation
Eight of the 9 studies examined social participation among children with disabilities (see Table A.1): 1 Level 3b matched case–control study, 4 Level 4 studies, and 3 Level 5 qualitative studies. Ripat and Becker (2012) examined school and community playground experiences of children and their caregivers in Canada. Twenty participants, including 4 children with disabilities ages 7 to 15 yr, their caregivers, and siblings, participated in in-depth, semistructured interviews. Families reported that the playground provided opportunities to engage in activities that promote social and motor skills. However, researchers also found that the lack of ramps made many areas inaccessible to children with mobility impairments. Without adequate means to reach all elements of the playground, structural barriers decreased opportunities for social participation by physically preventing access to peers. The risk of bias in this study is low; however, important limitations reported included the study’s small sample size and risk of inaccurate results due to communication difficulties.
Similarly, Stephens et al. (2015) noted that children with disabilities, especially those with impaired mobility, often lose the opportunity to socialize with their peers because of inaccessible equipment. This study examined accessibility and inclusivity at a school playground for children with disabilities in Canada. This mixed-methods study recruited 13 children with disabilities ages 10 to 14 yr for the case series and 406 children with disabilities ages 8 to 14 yr for the cross-sectional survey. Fifty percent of survey participants reported that pathways to playground equipment were often uneven, preventing wheelchair users from safely getting to the playground from the entrance, and leaving them together in a group, isolated from able-bodied peers. Participants (49%) who tried to access the playground despite mobility concerns took an extended amount of time, decreasing the time available for socialization with peers, and 50% of survey respondents found the playground equipment itself inaccessible. The risk of bias for this study is relatively low, and limitations included small and convenience sampling and inadequate population representation resulting from the lack of population estimates in Canada for children with disabilities.
In 2016, Stanton-Chapman and Schmidt evaluated the social participation of children with disabilities, from birth to sixth grade, at school and community playgrounds in the United States. Researchers used the Playground Attitude and Perception Survey to gather results from 303 education and intervention professionals (Stanton-Chapman & Schmidt, 2016). A staggering 99% reported their playground as inappropriate for their clients. Across all playgrounds, 96% lacked wheelchair ramps, and 90% lacked ramps that were level. Inappropriate settings and lack of accessibility were found to inhibit social participation for wheelchair users, despite being the playgrounds meeting ADA guidelines. Able-bodied peers found the playground uninteresting, leaving children with disabilities to play alone. When they did interact with peers, children with disabilities had difficulties physically keeping up. The risk of bias for this study is low, and limitations included small sample size, difficulty ensuring the validity of survey responses, and lack of students with hearing or visual impairments.
In 2017, Stanton-Chapman and Schmidt examined social participation again by surveying one family member each from 149 households using the Family Recreational Facility and Activity Perception Survey. The family members included parents, grandparents, and foster parents of children with disabilities ages 2 to 5 yr. Results supported their 2016 study, finding that much of the equipment was inaccessible to wheelchair users. Once more, structural barriers prevented children not only from physically accessing the equipment but from approaching and engaging with their peers as well. Children with SPD and autism also had difficulty socializing in the play spaces as a result of limited sensory stimulation. In fact, 65% of caregivers reported that they were unsatisfied with playground facilities and believed that they were inappropriate for their child’s needs. This study presented a low risk of bias, and limitations included small sample size, potential participant bias, and difficulty ensuring the validity of survey results.
Horton (2017) conducted a mixed-methods study to examine the social experiences of children with disabilities ages 5 to 16 yr. Examples of disabilities that were reported include mobility difficulties, autism spectrum disorder (ASD), and sensory impairments. Parents and caregivers completed a survey about two parks with playgrounds, each including accessible play spaces. This study supports findings that children with impaired mobility are susceptible to decreased socialization because of a lack of accessibility. The top barriers identified by participants included logistical challenges (67%), hazards (50%), and others’ attitudes (48%), which left children with mobility impairments unable to access the same spaces as their able-bodied peers. Participants reported experiencing stress because of discrimination from others. The stigma felt by the participants’ children raised questions of self-worth and resulted in decreased self-confidence in social engagement with peers. The risk of bias for this study was low.
Lynch et al. (2019) identified lack of accessibility as a barrier to social engagement for children with mobility impairments. Researchers examined opportunities for social skills development through walk-and-talk audits, semistructured interviews, and observations at community playgrounds in Ireland. Participants included 14 adults and 12 children, 5 of whom had a disability and were frequent users of five specific playgrounds. Older children with disabilities reportedly felt left out because playgrounds were for younger children. In addition, parents reported the need to watch their children carefully to divert them from dangerous areas resulting from poor design. Both factors were presented as barriers to socialization between children with and without disabilities. Alternatively, results suggested that the playgrounds created opportunities for socialization for children whose disabilities did not affect mobility, and the playgrounds were often viewed as an important component of the community. Through the examination of social skills development, this study adds to the growing body of literature acknowledging accessibility as a barrier to social participation and engagement. Despite the low risk of bias in this study, the small sample size limits its generalizability.
Jeanes and Magee (2012) examined the quality of inclusion of a playground through qualitative interviews with 18 parents and focus groups of 20 children with disabilities ages 4 to 16. This study was conducted at a specific U.K. playground, designed in part by parents, and located on the campus of a school for children with disabilities. Participants were recruited via flyers and word of mouth. Jeanes and Magee (2012) remarked that the availability of fully integrated accessible equipment increased socialization among children with disabilities and their peers, decreasing social isolation. The location of the playground was reported to increase participants’ confidence and social participation, because it was an environment in which children felt comfortable and supported, without fear of discrimination. This study had a low level of bias, and limitations included a small sample size, convenience sampling, and a lack of diversity.
Locke et al. (2016) examined social interactions through a matched case–control study between children with (n = 51) and without (n = 51) ASD during recess. Children were matched by classroom, grade, age, ethnicity, and gender and paired by means of a random number generator. Those with ASD were referred by administrators, and those without ASD were nominated by their teachers. Independent, blinded researchers used the Playground Observation of Peer Engagement to code behavior. Researchers reported that during recess, children with ASD spent less time (40%) than their neurotypical classmates (70%) in joint social participation with peers and more time (30%) than neurotypical peers (9%) engaging in solitary play. In addition, significant differences were found on all measures between children with ASD and their peers. Participants with ASD had significantly fewer successful initiations, fewer total initiations, fewer successful initiations, fewer positive responses, fewer total opportunities to respond, and fewer positive responses. Researchers did, however, find that some children with ASD had high engagement in peer interaction, suggesting that some children with ASD have increased social participation as a result of the playground’s accessibility. This study was assessed as having low risk of bias and reported the small sample size as a limitation.
Play Participation
Seven studies examined the role of accessible playgrounds on play participation among children with disabilities. Jeanes and Magee (2012) examined play participation at a playground partially designed by parents of children with disabilities. Wheelchair users reported that the design of the playground allowed them to try different equipment, whereas its previous design had not. In addition, the 18 families had previously experienced discrimination toward those with disabilities in traditional play settings. The feeling of “otherness” excluded children with disabilities from feeling that they could partake in play, and social barriers inhibited them from engaging in play participation. The inclusivity of this playground design, however, counteracted this social barrier, further promoting play participation. One child proclaimed that at this playground they were not stared at or called names and felt welcomed, and they felt it was a safe environment.
In their mixed-methods study examining accessibility, Stephens et al. (2015) found that 50% of students with mobility impairments experienced decreased play participation because of barriers such as uneven paths and inaccessible equipment. Another 68% reported that they did not always go out for recess when their able-bodied peers did, with the most notable reason being difficulty maneuvering in the playground in the winter because of their disability (57%). Those who went outside were often left on the pavement nearest the school because of overcrowding, leaving them grouped together, limiting the development of social skills through interaction with neurotypical or able-bodied children.
A qualitative descriptive study by Wenger et al. (2021) examined the play experiences of children with and without disabilities on accessible playgrounds in Switzerland. Participants were children ages 7 to 12 yr with (n = 14) and without (n = 18) a disability, who engaged in semistructured interviews. In addition, they were observed during play using a tool based on the PlayAUDIT, which assesses playground design, usability, accessibility, and play value (Wenger et al., 2021). The risk of bias was low, but Wenger et al. (2021) noted that interviews could have yielded stronger evidence. Similarly, Stephens et al. (2015) reported that although children with disabilities expressed positive experiences on accessible playgrounds, there were invisible barriers to play participation; children with disabilities stayed in areas where they felt they “belonged” instead of engaging in the play areas they wanted to.
Stanton-Chapman and Schmidt (2016) surveyed educators and interventionists and found that 99% of participants believed that the playgrounds were inappropriate for their students. Several participants reported a lack of accessible equipment for children with severe disabilities. Wood chips and areas without ramps made it difficult for children with wheelchairs to navigate the playground despite meeting ADA criteria. A year later, Stanton-Chapman and Schmidt (2017) studied caregivers to examine how current playground equipment in their area met the needs of their children. Of those who participated, 55% reported that their child was uninterested in the playground equipment available, 35% were concerned about safety, and 25% reported feeling uncomfortable as a result of discrimination. Unappealing equipment resulted in understimulation and disinterest in play, and safety concerns prevented children from independently participating in play. In addition, the playground structures and equipment were inaccessible for younger children with disabilities because they were too high to reach or difficult to access. Horton (2017) also reported that hazardous bumps and cracks prevented play participation for children with mobility impairments.
Locke et al. (2016) found that 30% of children with ASD spent recess unengaged or playing alone, whereas only 9% of their neurotypical peers did the same. Despite the playground being accessible, some children with ASD had decreased play participation compared with their peers. Conversely, the same study found that some children with ASD had high engagement in peer interaction, which increased play participation.
Motor Skills
Only 1 Level 5 qualitative study examined opportunities for motor skill development among children with disabilities (see Table A.1 in the online Supplemental Appendix). Ripat and Becker’s (2012) study of children with and without autism examined motoric playground perspectives and experiences. The results revealed that the playgrounds allowed children to use all equipment despite varying abilities, promoting motor skill development for all children. Specifically, equipment that offered varied use of balance, coordination, and fine motor skills was appreciated by parents and children. However, parents often noted that most playgrounds lacked this type of accessibility for children with impaired mobility. This study had a low level of bias, but its small sample size limits generalizability.
Discussion
This systematic review synthesizes existing research on the relationship between accessible playgrounds and childhood development among children with disabilities, but the literature was limited. Articles that met the inclusion criteria highlighted occupational injustice through common findings of inadequate accessibility and reduced occupational engagement in key areas that promote childhood development. Eight studies reported that children with mobility impairments frequently faced physical barriers to play, despite playgrounds being labeled as accessible (Horton, 2017; Jeanes & Magee, 2012; Locke et al., 2016; Ripat & Becker, 2012; Stanton-Chapman & Schmidt, 2016, 2017; Stephens et al., 2015; Wenger et al., 2021). Uneven pathways, lack of ramps, and inappropriate groundcover inhibited these children from using the spaces. As a result, researchers reported decreased engagement in play, social participation, and activities that promote motor skills development. In fact, only Jeanes and Magee (2012) reported a playground that was easy to navigate with a wheelchair, finding increased engagement in all areas as a result of adequate accessibility. Furthermore, children with mobility impairments in particular encountered physical barriers that prevented access to able-bodied peers, further decreasing opportunities to socialize. These findings indicate an area in which occupational therapy practitioners need to advocate for change in legislation regarding accessibility, especially as it relates to playground design. This is supported by a recent scoping review that identified and described the all-too- common practice of designing playgrounds to meet only the minimum standards necessary to be ADA compliant (Brown et al., 2021). Furthermore, because several playgrounds identified in this systematic review reportedly adhered to ADA guidelines yet remained inaccessible, guidelines need to be reevaluated.
Even on accessible playgrounds, participants across 4 studies reported social stigma as an invisible barrier to play and socialization (Horton, 2017; Jeanes & Magee, 2012; Stanton-Chapman & Schmidt, 2017; Wenger et al., 2021). Parents felt out of place as a result of discriminatory attitudes toward their children from others. Children with disabilities felt they belonged in an area separate from able-bodied or neurotypical children and felt ostracized from peers. Occupational therapy practitioners are poised to address this issue. Integrating education on adaptive coping skills and self-advocacy into school sessions would allow children with disabilities to be better equipped when facing discrimination or having unmet needs. Education on disability and normalizing disability would be meaningful for all children, teachers, and parents.
We have not reported results on the relationship between accessible playgrounds and cognition or behavior because no studies covered these topics and met our criteria. This glaring oversight requires research, the results of which would be incredibly beneficial when working with the pediatric disability population. Although the level of bias across the studies included in this review was relatively low, the evidence consisted of primarily Level 4 and 5 studies. Researchers should aim to conduct higher-level longitudinal cohort studies to better understand how accessible playgrounds affect all areas of childhood development over time.
Limitations
Studies focusing on outcomes for behavior and cognition specifically among children with disabilities on accessible playgrounds were scarce. In addition, findings on motor skills were limited in comparison with those on social and play participation. Nine studies met the inclusion criteria for this review, which restricted the quality of research included. Most of the studies consisted of Level 4 and 5 research, including cross-sectional surveys and qualitative research. Other common limitations were small sample sizes and convenience samples, lack of a universal definition of an accessible playground, and third-person interviews rather than interviews with children with disabilities, which do not fully illustrate the experiences of this population. Methodologically, there is potential for error in the search terms chosen to identify the relevant literature as a result of missing key terms. However, we used a comprehensive list of terms across development domains with assistance from the university librarian, and advanced Boolean modifiers were used to maximize the scope of the search. There is also always risk of error in each point of assessment procedurally, whether in screening titles and abstracts, reviewing the full text, and assessing level of evidence or risk of bias. However, we abided by rigorous PRISMA guidelines and used validated assessment tools whenever possible and multiple independent reviewers for each assessment in the review process.
Implications for Occupational Therapy Practice
These common findings of inaccessibility are a prime example of occupational injustice for children globally. We suggest that occupational therapy practitioners consider joining the field of playground design to address key areas of need while understanding the developmental and sensory needs of children through consultation. Occupational therapy practitioners are in the unique position to address environmental negligence that bolsters occupational injustice in a variety of both indoor and outdoor play spaces for children (Brown et al., 2021
; Moore & Lynch, 2015). As a result, occupational therapy practitioners should address not only the environmental barriers, but also the political and social contexts that cultivate the unprecedented cultural stigma and exclusion of those with disabilities. As such, occupational therapy practitioners must move beyond their traditional practice settings to radical and pragmatic venues to dismantle the structural and societal stigmas that surround disabilities to create an inclusive environment. We recommend that occupational therapy practitioners engage in nontraditional settings to develop more stimulating and accessible playground equipment, advocate for policy change, implement programs within the school system to increase awareness of children with disabilities and decrease stigma from an early age, provide education on coping skills to students with disabilities to better equip them to handle discrimination they may face, and discuss playground accessibility in occupational therapy educational programs when learning about pediatric environmental contexts to increase awareness and better prepare students for potential community roles in advocacy within the profession.
Conclusion
It is important to further understanding of the value of accessible playgrounds because current research has shown that they affect childhood development for children with disabilities, resulting in occupational injustice. Evidence suggests that social and play participation are significantly affected by inaccessible playgrounds, social stigma, and discrimination. Extensive research is necessary to understand how the development of behavior, cognition, and motor skills are affected, because these topics have not been adequately explored. Future research should implement stronger study designs and include larger sample sizes of children with disabilities to gather findings that can be generalized to this overall population. Therefore, occupational therapy practitioners should conduct longitudinal cohort studies on the effect of accessible playgrounds on all areas of childhood development of children with disabilities. An audit of ADA-compliant playgrounds also needs to take place, because several ADA-compliant playgrounds were found to be inaccessible, and a study evaluating the efficacy of ADA guidelines for play spaces for children should be conducted.
Occupational therapy practitioners would greatly benefit from additional research on this topic because it would enhance their evidence-based practice knowledge of elements that influence childhood development among children with disabilities. Also, further research may expand knowledge of the occupation of play for this population, which would better equip occupational therapy practitioners to serve as advocates for occupational justice. The narrow research that is available should bring awareness to future playground developers and encourage them to strategize and construct playgrounds that meet the needs of children of all abilities.
Supplemental Material
Supplementary material for Occupational Injustice and the Right to Play: A Systematic Review of Accessible Playgrounds for Children With Disabilities
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050035.pdf for Occupational Injustice and the Right to Play: A Systematic Review of Accessible Playgrounds for Children With Disabilities by Kelsey A. Gately, Anna H. Zawadzki, Alyssia M. Mosley, Alyssamarie K. Badua, Jennifer E. Swanberg and Samantha R. Rosenthal in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
The preparation of this article was partially supported by the 2021 Provost Incentive Funds, Johnson & Wales University. We thank Erika Gearing and Eileen Medeiros for their research and writing assistance during the preparation of this article. We declare no conflict of interest. No ethics approval was needed for this systematic literature review, and all PRISMA guidelines were followed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.