
Abstract
This systematic review adds to the body of literature indicating that people diagnosed with Autism spectrum disorder (ASD) have sensory abnormalities with regard to pain experiences and highlights the need for occupational therapy interventions to focus on pain experiences.
Autism spectrum disorder (ASD) is one of the most prevalent neurodevelopmental disorders (Fetit et al., 2021; Watts, 2008). People with ASD present with a triad of core symptoms: (1) a qualitative impairment in social interaction (an inability to relate to others, often with a lack of eye contact); (2) stereotypical, ritualistic, repetitive, restrictive patterns of interests, behaviors, and activities; and (3) major defects in language development and in other communication skills (Hodges et al., 2020). A recent study has further reported that ASD is associated with many systematic comorbidities, such as gastrointestinal dysfunction (9%–91% of people with ASD), autoimmune conditions such as allergies, and sensitivity dysfunction related to pain (Leader et al., 2020).
Previously, in clinic-based research, sensitivity dysfunction has been estimated to affect approximately 69% to 95% of people with ASD (Burns et al., 2017; Moore, 2015; Tomchek & Dunn, 2007). The latest diagnostic criteria for ASD in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association, 2013) describe the sensitivity abnormalities in ASD as having two common presentations, hyposensitivity and hypersensitivity, that interfere with effective learning of daily functioning and with interactions. Occupational therapy researchers use the term sensory processing disorder to describe these sensitivity abnormalities (Ahn et al., 2004; Kern et al., 2006; Tomchek & Dunn, 2007).
Pain perception among people with ASD has been a topic of much discussion over the past few years. It has been suggested that people with intellectual disabilities such as ASD may experience insensitivity or paradoxical behaviors in response to painful stimuli (Ross-Russell & Sloan, 2005). As many as 70% of people with ASD may demonstrate self-injurious behavior at some point in their lives, but this behavior is typically found among more severely affected people and takes many forms, including head banging, scratching, bruising, and biting (Ross-Russell & Sloan, 2005). One of the first accounts of abnormality in sensitivity to pain among people with ASD is that of Mahler (1952), who described a teenager who, after watching their mother use a car cigarette lighter, put the lighter in their mouth, burning their lips, but did not cry out in pain. Assessing pain among people with ASD can be complex; because of their communication and social difficulties, it can be harder for them to express their discomfort, and they may express pain through specific behaviors (e.g., stereotyped and self-injurious behaviors).
Sensory abnormalities among people with ASD have been extensively documented in various literatures (Blanche et al., 2012), and this has resulted in extensive investigation of multiple sensory domains (for a review, see Baum et al., 2015). Likewise, a review of 17 studies (Moore, 2015) of sensory abnormalities with regard to the experience of acute pain among people with ASD concluded that they do not have altered pain responses or altered thresholds to acute pain. In contrast to Moore’s (2015) results, however, a recently published systematic review (Vaughan et al., 2019) analyzed pain processing among people with different psychiatric conditions, including ASD. The authors concluded that there is tentative evidence of sensory abnormalities with regard to altered touch and pain processing among those with psychiatric disorders or ASD.
Although both reviews (Moore, 2015; Vaughan et al., 2019) focused on whether people with ASD experience sensory abnormalities with regard to pain, new studies have been published. New studies on this topic have recently been published, and their conclusions with respect to pain abnormalities among persons with ASD are contradictory.
Therefore, the purpose of this research was to conduct a systematic review of the literature to summarize current evidence from case–control studies comparing sensory abnormalities with regard to pain experiences among people diagnosed and not diagnosed with ASD. Evidence of sensory abnormalities with regard to pain could help occupational therapy practitioners provide appropriate interventions or accommodations to ameliorate these issues among people with ASD.
Method
Protocol
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021) and Meta- analysis Of Observational Studies in Epidemiology guidelines (Stroup et al., 2000). The study was registered with the International Prospective Register of Systematic Reviews in 2021 (PROSPERO Registration No. CRD42021247334).
Search Strategy
Using MeSH terms and broad keywords, a systematic literature search was performed in five electronic databases from their inception to December 2021: CINAHL, Cochrane, MEDLINE (PubMed), OTseeker, and Web of Science. The full search strategy for MEDLINE (PubMed) is presented in the Supplemental Appendix (available online with this article at https://research.aota.org/ajot), and a description of the search strategy is presented in Table A.1. A similar search strategy was used for the other databases. The searches began in June 2021 and included all articles that existed in the database until that date, with the final search completed in January 2022. Hand searches were conducted of the reference lists of the included studies to ensure no relevant studies were omitted. Emails to corresponding authors and interlibrary loan were used to obtain access to articles as needed.
Selection Criteria
Selection criteria were set according to the PICOS approach: population or participants (P), interventions or exposure (I), comparison (C), outcome (O), and study design (S). Participants were people with a diagnosis of ASD, including children and adults, according to Leo Kanner’s (1968) description of ASD. Diagnosis was ascertained by use of standardized tools, medical professionals, or International Classification of Diseases codes. Interventions or exposure was deemed not applicable according to the objective of this systematic review. The comparison group consisted of healthy people without ASD. The outcome was any outcome of pain experienced objectively, subjectively, or both, and the study design had to be case–control. Duplicate studies with the same data were excluded. Only records published in Arabic, English, French, or Spanish were included in the systematic review. The exclusion criteria were as follows: (1) participants with a pluripathology, neurological condition, or both and (2) no full-text access.
Selection Process
All the searched citations were stored in EndNote (Version X9). First, two researchers (Irene Torres Sánchez and Araceli Ortiz Rubio) screened the titles and abstracts independently. Studies that appeared to meet the inclusion criteria or those with insufficient data in the title and abstract to make a clear decision were selected for full-text evaluation, which was carried out independently by the same two researchers who determined the studies’ eligibility. Any discrepancies were resolved by discussion with a third researcher (Laura López López). To prevent selection bias, researchers were blind to the name of the authors, institutions, and journal titles.
Data Extraction and Synthesis
Data extraction and synthesis was performed independently by two review authors (Irene Cabrera Martos and Janet Rodríguez Torres) using an Excel spreadsheet and applying a predesigned criterion data collection form. The data collected were study characteristics, such as authors, year, country of origin, sample size, participants’ age, pain measurement instruments or methods, and findings.
Quality Assessment
The quality of the studies was assessed using the Newcastle–Ottawa Scale (NOS), a representative tool developed to evaluate observational studies such as case–control studies that can be used as either a checklist or a scale (Stang, 2010). The NOS is suitable for systematic reviews because of its easy application, and it has been widely used as a result of recommendations from the Cochrane Collaboration. The NOS contains eight items categorized into three dimensions: selection, comparability, and—depending on the study type— outcome (cohort studies) or exposure (case–control studies). For each item, a series of response options is provided. A star system is used to allow a semiquantitative assessment of study quality, such that the highest quality studies are awarded a maximum of 1 star for each item, with the exception of the item related to comparability that allows the assignment of two stars. Scores on the NOS range between 0 and 9 stars; a study with a score of 7 to 9 is considered to be of high quality; 4–6, of moderate quality; and 0–3, of low quality.
Results
Study Selection
The search and screening process based on the PRISMA statement is depicted in Figure 1. Using a combination of keywords and MeSH terms, we identified a total of 2,951 records (CINAHL, n = 47; Cochrane, n = 287; MEDLINE/PubMed, n = 1,442; Web of Science, n = 1,174; OTseeker, n = 1). After duplicates were removed (n = 238), 2,713 records remained. Of these, 1,220 records were removed according to selection criteria. A total of 1,493 records underwent title and abstract screening, and 1,451 were excluded. Full-text screening was then performed on 27 records (21 from the databases and 6 identified through a hand search). These 27 studies met the inclusion criteria, were exported to EndNote, and were subjected to data extraction and quality assessment. All studies were published in English. Study characteristics and data are presented in Table A.2 of the Supplemental Appendix. Meta-analysis was not possible because of the variability in the methods used, the heterogeneity of results reported, and the lack of reported confidence intervals and effect sizes.
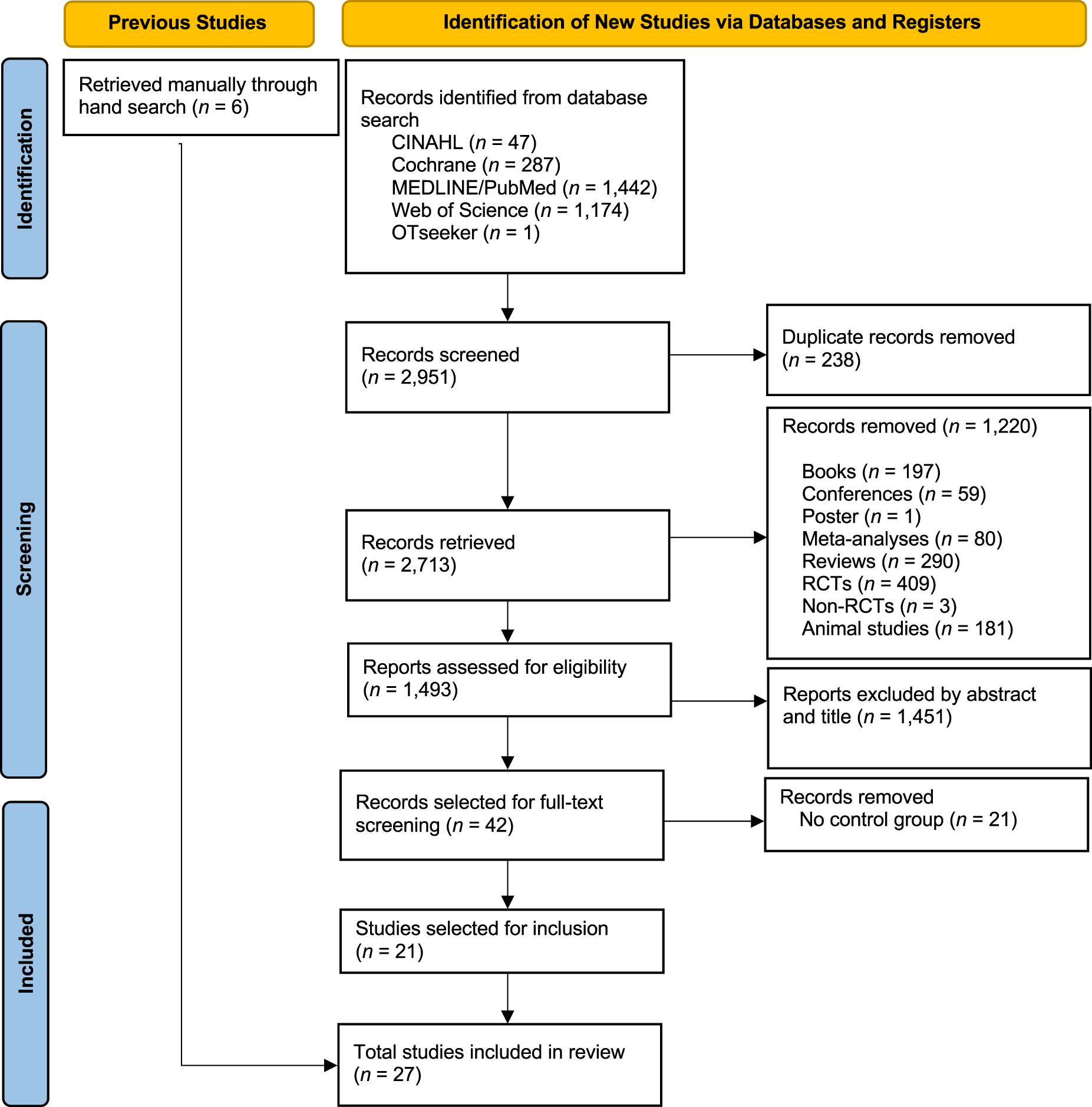
Flow diagram of the study selection process.
Quality Assessment
The results of the quality assessment of the included studies using NOS are shown in Table A.3 in the Supplemental Appendix. In the majority of studies included in this systematic review, the control group was matched on at least age and gender. Other confounding factors, such as alexithymia scores, intelligence, or race, were also considered in some of the included studies. The quality score for the included studies was moderate.
Study Characteristics
The characteristics of the studies included in the systematic review and their results are summarized in Table A.2 of the Supplemental Appendix. The majority of the 27 studies included in this systematic review were conducted in the United States (n = 7; Cascio et al., 2008; Failla et al., 2018, 2020; Fan et al., 2014; Gu et al., 2018; Kern et al., 2006, 2008) and Canada (n = 4; Bandstra et al., 2012; Dubois et al., 2020; Minshew & Hobson, 2008; Nader et al., 2004).
In 10 studies, ASD was confirmed according to the Autism Diagnostic Observation Schedule (ADOS; Bandstra et al., 2012; Bird et al., 2010; Cascio et al., 2008; Duerden et al., 2015; Failla et al., 2020; Gu et al., 2018; Lassalle et al., 2018; Minshew & Hobson, 2008; Rattaz et al., 2013; Vaughan et al., 2020). In 19 studies, the diagnosis was confirmed using the Diagnostic and Statistical Manual of Mental Disorders (Bird et al., 2010; Blakemore et al., 2006; Cascio et al., 2008; Chen et al., 2017; Failla et al., 2018, 2020; Fan et al., 2014; Fründt et al., 2017; Gu et al., 2018; Güçlü et al., 2007; Kern et al., 2006, 2008; Lassalle et al., 2018; Militerni et al., 2000; Nader et al., 2004; Riquelme et al., 2016; Sener et al., 2017; Tordjman et al., 2009; Yasuda et al., 2016); however, different editions of the manual were used. Finally, 4 studies (Dubois et al., 2020; Rattaz et al., 2013; Thaler et al., 2018; Tordjman et al., 2009) used the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD; World Health Organization, 2015). A total of 1,729 people participated in the studies included in this systematic review (865 persons with ASD and 864 control persons). Study sample size ranged from 12 to 208. A total of 10 studies were conducted with children and adolescents, but the majority were conducted with adults (n = 16). Only 1 study included both children and adults, whose ages ranged from 8 to 54 yr.
Several methods were used to explore sensory abnormalities with regard to pain experiences. These methods included clinical observations, self- and parent reports, or sensory testing using threshold detection (thermal, vibratory, mechanical) or pain threshold (pain pressure or electrocutaneous). The method used most often was thermal detection threshold (n = 8; Cascio et al., 2008; Dubois et al., 2020; Duerden et al., 2015; Failla et al., 2018, 2020; Fründt et al., 2017; Güçlü et al., 2007; Vaughan et al., 2020). Five studies used pain pressure threshold (Chen et al., 2017; Fan et al., 2014; Fründt et al., 2017; Riquelme et al., 2016; Vaughan et al., 2020), 4 used electrocutaneous pain threshold (Bird et al., 2010; Gu et al., 2018; Güçlü et al., 2007; Thaler et al., 2018), 4 used mechanical pain threshold (Cascio et al., 2008; Fründt et al., 2017; Riquelme et al., 2016; Vaughan et al., 2020), and 3 used vibratory detection threshold (Blakemore et al., 2006; Cascio et al., 2008; Fründt et al., 2017).
Other methods used to explore pain experiences among people with ASD were objective instruments such as electroencephalogram, event-related potentials, and self- or parent-report instruments such as the Brief Pain Inventory, Charleston Pediatric Pain Pictures, or Face Pain Scale. Controversial findings were reported; a minority of case–control studies (n = 8) suggested people with ASD show no sensory abnormalities with regard to pain when compared with control participants (Bandstra et al., 2012; Bird et al., 2010; Dubois et al., 2020; Fründt et al., 2017; Güçlü et al., 2007; Thaler et al., 2018; Tordjman et al., 2009; Yasuda et al., 2016).
Of the 8 case–control studies that reported no between-groups differences in relation to sensory abnormalities with regard to pain, only 5 studies used threshold testing (Bird et al., 2010; Dubois et al., 2020; Fründt et al., 2017; Güçlü et al., 2007; Thaler et al., 2018). Two of these studies used clinical observation, such as the Sensory Profile (Dubois et al., 2020; Güçlü et al., 2007), and all of them included self- and parent reports in their evaluation (Bandstra et al., 2012; Bird et al., 2010; Dubois et al., 2020; Yasuda et al., 2016).
Meanwhile, the majority of studies (n = 17) included in the qualitative synthesis suggested that there are between-groups differences in relation to pain experiences (Blakemore et al., 2006; Cascio et al., 2008; Chen et al., 2017; Failla et al., 2018, 2020; Fan et al., 2014; Gu et al., 2018; Kern et al., 2006, 2008; Militerni et al., 2000; Minshew & Hobson, 2008; Nader et al., 2004; Rattaz et al., 2013; Riquelme et al., 2016; Sener et al., 2017; Umesawa et al., 2020; Vaughan et al., 2019).
These 17 studies used several methods to detect between-groups differences in relation to pain experiences. For example, only 1 study showed that persons with ASD have lower tactile perceptual thresholds in comparison with the control group (Blakemore et al., 2006); Cascio et al. (2008) suggested that people with ASD have hypersensitivity for both cold and heat pain thresholds, and 4 studies found lower pain pressure thresholds among persons with ASD than among the control group (Chen et al., 2017; Fan et al., 2014; Riquelme et al., 2016; Vaughan et al., 2020). Duerden et al. (2015) found significant between-groups differences to detect cold–warm stimuli. Finally, Failla et al. (2018) found reduced neural pain signature response during sustained pain and after stimulus offset among people with ASD, and Gu et al. (2018) found lower electrocutaneous pain threshold.
Finally, a reduced ability to modulate sensory stimuli (Kern et al., 2006, 2008), more activation of the thalamus and the right inferior frontal gyrus (Lassalle et al., 2018), and reduced gamma-aminobutyric acid (GABA) concentrations in the left supplementary motor area (Umesawa et al., 2020) were found in persons with ASD. In addition, a statistically significant difference in terms of gene expression was found between groups in a case–control study (Sener et al., 2017).
Discussion
The purpose of this systematic review was to summarize the current evidence from case–control studies comparing sensory abnormalities with regard to the pain experiences of people diagnosed and not diagnosed with ASD. To the best of our knowledge, this is the first systematic review of case–control studies to explore sensory abnormalities with regard to pain in persons with ASD. The results of the systematic review suggest that, despite the controversial literature on this topic, the sensory experiences of people with ASD may be abnormal with regard to pain sensitivity. Data obtained from different case–control studies show that pain sensitivity can present as altered processing of sensory stimuli, altered response to stimuli, or elevated activation in the thalamus and the right inferior frontal gyrus and reduced GABA concentrations in the left supplementary motor area. Although the method or protocol used to assess pain differed across studies, thus limiting the rigor of the review and the validity of our conclusions, this is the first systematic review of case–control studies exploring pain among people with ASD to use PRISMA recommendations and review the quality of each case–control study included.
In the early 1990s, the terms pain insensitivity (the inability to distinguish between different levels of pain stimuli) and pain indifference (the inability to detect the bodily sensations of pain as pain) were used to describe the abnormal experience of pain thought to exist among people with communicative, cognitive, or motor impairments (Biersdorff, 1991, 1994), such as people diagnosed with ASD. In the same vein, it was proposed that people with functional diversity were more likely to present with pain insensitivity or indifference (Biersdorff, 1994) than persons without such diversity. In the past 4 decades, the field of neuroscience has made rapid progress in elucidating abnormal sensory sensitivities among people with ASD (Burns et al., 2017; Dellapiazza et al., 2018; Kanner, 1968; Vaughan et al., 2019). These sensory abnormalities are often present in multiple modalities and include both hypersensitivity and hyposensitivity. People with ASD may display a pattern of exaggerated behavioral response to sensory stimuli (e.g., feeling pain) or a lack or insufficiency of response to sensory stimuli (Posar & Visconti, 2018). In the same vein, findings suggest that people with ASD may have sensory disturbances with regard to pain (e.g., abnormal pain responses, such as hyposensitivity or hypersensitivity after application of a stimulus). However, these results should be viewed with caution because of potential biases in these studies, such as varied instruments and methods or protocols to assess pain sensitivity, different ages of participants, and varying functioning among participants.
Over the past four decades, research on sensory processing in those with and without ASD has enhanced the understanding of how the brain processes sensory input. Research has suggested that people with ASD may have difficulty with the registration of stimuli (signal detection and interpretation of stimuli), modulation of the sensory input (inhibition of high- intensity inputs or propagation of low-intensity sensory inputs), interaction with stimuli in the environment, and the motivation to interact. These sensory disturbances may be caused by a defect in the nervous system that results in sensory stimuli being processed and integrated abnormally (Ayres, 1972; Ayres & Tickle, 1980; Schaaf & Miller, 2005).
Ayres Sensory Integration® (ASI) therapy is frequently requested by caregivers and is often used by occupational therapy practitioners with positive effects among children with sensory processing difficulties such as ASD (Andelin et al., 2021; Clark et al., 2019; Parham et al., 2019; Schoen et al., 2019). The therapy involves the client interacting with a combination of equipment, such as scooters and swings, that provides the opportunity to obtain and process enhanced sensory input and develop normal levels of arousal and security when interacting with their environment. However, despite the high utilization of ASI therapy to explore and treat sensory processing disorder among children and teenagers with ASD, published studies focused on adults with ASD are lacking. In this systematic review, the majority of studies exploring sensory abnormalities with regard to pain were carried out among adults with ASD. However, little information is available regarding the effect of ASI therapy among adults and children with ASD. Future studies are necessary to demonstrate its effectiveness in improving and reducing pain sensitivity among adults with ASD.
The main strength of this review is its novelty. To our knowledge, no previous systematic review has focused on the exploration of pain among individuals with ASD. A broad search strategy was used, complemented by an extensive hand search of reference lists, so the possibility that important published data are missing is low. A relatively narrow clinical question allowed us to focus in detail on the included studies and enabled a clear and meticulous presentation of findings.
Limitations
This systematic review did, however, have some limitations that should be taken into account. The studies included in the review were significantly heterogeneous in relation to sample size, age, methods and protocols used to assess abnormal sensitivity to pain, and heterogeneity of results reported. Participant sample sizes in the studies ranged from 16 to 206; therefore, the sample sizes of the studies are extremely heterogeneous. Different case–control studies used diverse methods and protocols to assess sensitivity to pain, including parent reports, self-reports, and experimental records. These heterogeneities made it impossible to combine the data from these studies in a meta-analysis.
Implications for Occupational Therapy Practice
The findings may have important clinical and research implications, because promoting early intervention among persons with ASD may lead to more adequate development of somatosensory processing and fewer somatosensory anomalies with regard to pain in adult life. Occupational therapy practitioners could design ASI therapy–based interventions to address sensory disturbances such as pain.
Conclusion
The results of this systematic review suggest that people with ASD have an abnormal sensitivity to pain, such as altered pain responses or lower thresholds to thermal or pain stimuli. However, because of the inconsistency in the utilization of comprehensive protocols and the moderate methodological quality of the studies included, these findings should be regarded with caution. This systematic review highlights the need for future studies with higher methodological quality to confirm these findings.
Supplemental Material
Supplementary material for Pain Experiences of People Diagnosed With Autism Spectrum Disorder: A Systematic Review of Case–Control Studies
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050050.pdf for Pain Experiences of People Diagnosed With Autism Spectrum Disorder: A Systematic Review of Case–Control Studies by Araceli Ortiz Rubio, Dulce Nombre de María Romero Ayuso, Irene Torres Sánchez, Irene Cabrera Martos, Janet Rodríguez Torres, Laura López López and Marie Carmen Valenza in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.