
Abstract
This study highlights a discrepancy between autistic people’s need for social interactions and the social pain they experience, and suggests directions for intervention programs to improve their coping strategies and promote their self-acceptance and better inclusion in the community.
Typically, humans have a fundamental need to feel connected to others and are motivated to seek and maintain strong, stable, and long-lasting interpersonal relationships (Baumeister & Leary, 1995). Social pain is an unpleasant experience associated with actual or potential damage to one’s sense of social connection or social value in relationships with partners or groups (Eisenberger, 2015; MacDonald & Leary, 2005).
Social pain includes four main sources: exclusion, rejection, negative evaluation, and loss (Eisenberger, 2012, 2015). Social exclusion is a multidimensional process of the progressive breakup of social ties wherein individuals and groups are detached from social relations and prevented from fully participating in normative daily activities (Silver, 2007). Similarly, social rejection typically manifests as a declaration by others that they do not want to interact with or be in the company of the person (Williams, 2007). Another source of social pain is negative social evaluation or social devaluation. Although there is no precise definition of negative social evaluation, its factors and implications are described in the literature. These include social stress resulting from bullying, social marginalization, teasing, or negative stereotypes (Padilla et al., 2019). Negative social evaluation may affect self-value or significance, leading to reduced social identity (Goffman, 1964). The last main source of social pain is social loss, defined as the termination of a meaningful or protective social bond (Eisenberger, 2012).
Previous research has demonstrated that the sources of social pain are linked to loneliness (i.e., Allen et al., 2020; Hajek & König, 2017). Loneliness is a lack of social contact and the feeling of being cut off or separated from other people (Hays & DiMatteo, 1987). These previous studies did not focus on social pain and hence did not characterize the entirety of factors that lead to loneliness. Research on loneliness is also limited and focused on children and adolescents (e.g., Bauminger et al., 2003). In addition, there is a paucity of qualitative data providing firsthand accounts of autistic people regarding their sense of loneliness (Umagami et al., 2022). Research regarding social pain is scarce; most pain research has focused on physical pain and its neural mechanism (e.g., Eisenberger & Lieberman, 2004; Sturgeon & Zautra, 2016). The concept of social pain was developed on the basis of evidence that the social attachment system evolved from more primitive regulation systems, such as those involved in place attachment, thermoregulation, and physical pain (Panksepp, 1998). Later research revealed that the experience of actual or potential damage to one’s feeling of social connection or value shares overlapping neural networks with physical pain (e.g., Eisenberger & Lieberman, 2004; Sturgeon & Zautra, 2016).
People who are involved in social relationships enjoy benefits such as better well-being (Mellor et al., 2008), greater ability to cope with stress (Cohen, 2004; Zaleski et al., 1998), and improved health (Berkman & Syme, 1979). However, challenges in the sense of belongingness may lead to psychological and physical health concerns (Milton & Sims, 2016), including depression (Nolan et al., 2003), impaired self-regulation (Baumeister et al., 2005), and a poorer immune system (D’Acquisto & Hamilton, 2020). Lack of social contact may be experienced as social pain (DeWall & Richman, 2011; Eisenberger, 2012, 2015).
Differences in social interaction and communication skills characterize people with autism spectrum disorder (ASD; American Psychiatric Association [APA], 2013). Considering these differences, autistic people seem more likely than their neurotypical peers to encounter social pain across their lifespan and be more exposed to social devaluation and rejection (Jones et al., 2021; van Roekel et al., 2010). Previous studies have demonstrated the importance of belongingness and social support for developing resilience and coping and as a protective factor against depressive symptoms, suicide attempts, and mental health challenges among autistic people (Ghanouni & Quirke, 2022; Hedley et al., 2017). However, the implications of the lack or absence of social connections for social pain have not yet been studied.
The literature considering social pain among autistic people scarcely addresses sources or coping strategies for social pain. Only Bolling et al. (2011) considered social exclusion a source of social pain among autistic people. Rather, the literature has suggested that their social pain processing in a social context might be unusual (Fitzgibbon et al., 2013). For example, some studies have noted that autistic people exhibit reduced empathy for physical or emotional pain in others (e.g., Krach et al., 2015; Masten et al., 2011) and reduced sensitivity to social fairness as expressed in rule violations (Bolling et al., 2011). However, those studies were conducted in laboratories under experimental terms and not in natural, daily living contexts or from learning the perspectives of autistic people.
Given these discrepancies in the literature, the current study aimed to explore the experience of social pain as perceived by autistic people, including the sources and coping strategies unique to this population. Insight into the inner world of autistic people regarding social pain may promote a better understanding of their experiences and have important theoretical and practical implications regarding the causes of social challenges.
Method
This study was a part of concurrent parallel, mixed-methods research (Creswell & Poth, 2017) that included an inclusive, comprehensive quantitative study and a qualitative study. All 18 interviewees who participated in the quantitative research were purposefully invited to participate in the qualitative research. This article addresses only the qualitative part of the research. The qualitative study used a phenomenological approach to explore how autistic people experience, perceive, and cope with social pain. This approach is well suited to examining perspectives on complex, ambiguous, and emotionally laden issues. Pain is a prime exemplar of such a phenomenon because it is elusive and difficult to articulate (Smith & Osborn, 2015).
Participants
We used purposeful and criterion sampling to select participants who could relate to and describe their pain experiences (Creswell & Poth, 2017). Purposeful sampling is used widely in qualitative research to identify and select information-rich cases related to the phenomenon of interest. Criterion sampling is used to identify and select all cases that meet some predetermined criterion of importance (Palinkas et al., 2015). Our inclusion criteria were as follows: (1) age 18 yr or older; (2) Level 1 ASD diagnosed using the Autism Diagnostic Observation Schedule,™ Second Edition (Lord et al., 2012); (3) verbal performance and full-scale estimate of 80 or higher on the Wechsler Abbreviated Scale of Intelligence, Second Edition (Wechsler, 2011); and (4) linguistic proficiency sufficient to provide in-depth descriptions of life experiences, as determined by the interviewer. The exclusion criterion was any diagnosed chronic pain.
Of the 18 people invited to participate in this study, 2 declined, and 1 could not participate because of technical issues. Thus, the sample consisted of 15 autistic adults (6 men, 9 women; Table 1) ages 18 to 45 yr (M = 28.67 yr, SD = 6.81). Although the female-to-male ratio of ASD diagnosis is 1:4 in the global population (Maenner et al., 2020), we included a larger number of women because they proved more willing to share their experiences and demonstrated better abilities to provide deep and rich descriptions and insights.
Participants’ Characteristics
Note. Participant pseudonyms were coded with initials. Residence descriptions are defined as follows: with family members = living with family members; hostel = housing arrangement designed for those who can use community services and be involved in the community; apartment in the community = housing accommodation for those who can function independently but need support; independent living = housing with no external assistance.
Procedure
The University of Haifa Ethics Committee of the Faculty of Social Welfare and Health Sciences approved this study, and all participants signed online informed consent forms. We ensured the participants’ privacy and confidentiality by coding and removing their identifying details and allowing them to withdraw from the study at any stage.
Participants were invited to in-depth interviews at a location of their choice, online, using Zoom videoconferencing software. They were advised to participate in the interview while sitting in a quiet and private place. Although the participants were not required to turn on their cameras, all did. Each interview lasted 60 to 90 min and was audio-recorded only.
The first author (Merry Kalingel-Levi), an occupational therapist experienced in working with autistic adults, conducted the interviews sensitively and facilitated open and safe communication with the participants. We adapted the interviews for autistic people in several ways. For example, we conducted preliminary telephone conversations with each participant regarding their preferred setting and facilitated communication about any concerns they had; edited the interview guide for simple and concrete language; invited participants to ask for clarifications and breaks; reminded them of the option to avoid unpleasant questions; and conducted two follow-up telephone conversations to ensure they were well after the interview.
Research Tools
We developed an interview guide based on the literature, preliminary quantitative study results, and clinical experience. The guide’s open-ended questions referred to issues relevant to the pain experience (e.g., subjective pain definitions, pain triggers, and pain throughout the lifespan). The questions provided a flexible framework that invited participants to lead the interview according to their perspectives while enabling the interviewer to maintain conceptual and structural focus on issues relevant to all interviewees.
Data Analysis
We analyzed the interviews by examining thematic content based on the participants’ descriptions and examples of their experiences, feelings, thoughts, and perceptions. The analytic process consisted of three stages (Corbin & Strauss, 2015): (1) initial citation analysis, identifying textual meaning units and grouping them into categories; (2) mapping analysis, revealing similarities and divergences, potential meanings, examples, perspectives, and best practices; and (3) focused analysis, conceptualizing findings into themes.
Initially, Merry Kalingel-Levi, Naomi Schreuer, and Eyant Gal independently coded the first three interviews into 29 preliminary categories (later merged into 15) to map the remaining interviews. Four main themes emerged from this brainstorming process with significant example citations.
We stopped interviewing after the 15th participant because of content saturation; no new themes emerged from the data (Charmaz, 2014). The participants’ rich descriptions, demographic data, and contexts ensured study trustworthiness. We continually conducted open conceptual discussions alongside peer review of the data, authors’ familiarity with the phenomena, and the literature.
Results
Four primary themes emerged concerning social pain among autistic people: (1) definition, (2) sources, (3) loneliness as an outcome, and (4) coping strategies. The definition theme explains the social pain phenomenon as perceived by autistic people; the other three themes provide a deeper understanding of it. Themes and subthemes of the experiences of autistic people regarding social pain ensue from each other, as presented in Figure 1. The first component in the flowchart reflects internal and external sources of social pain. The second component, loneliness, is derived from these two pain sources. The last component pertains to the coping continuum of autistic people as it ranges from the inward to outward coping strategies interviewees adopted throughout their life stories.
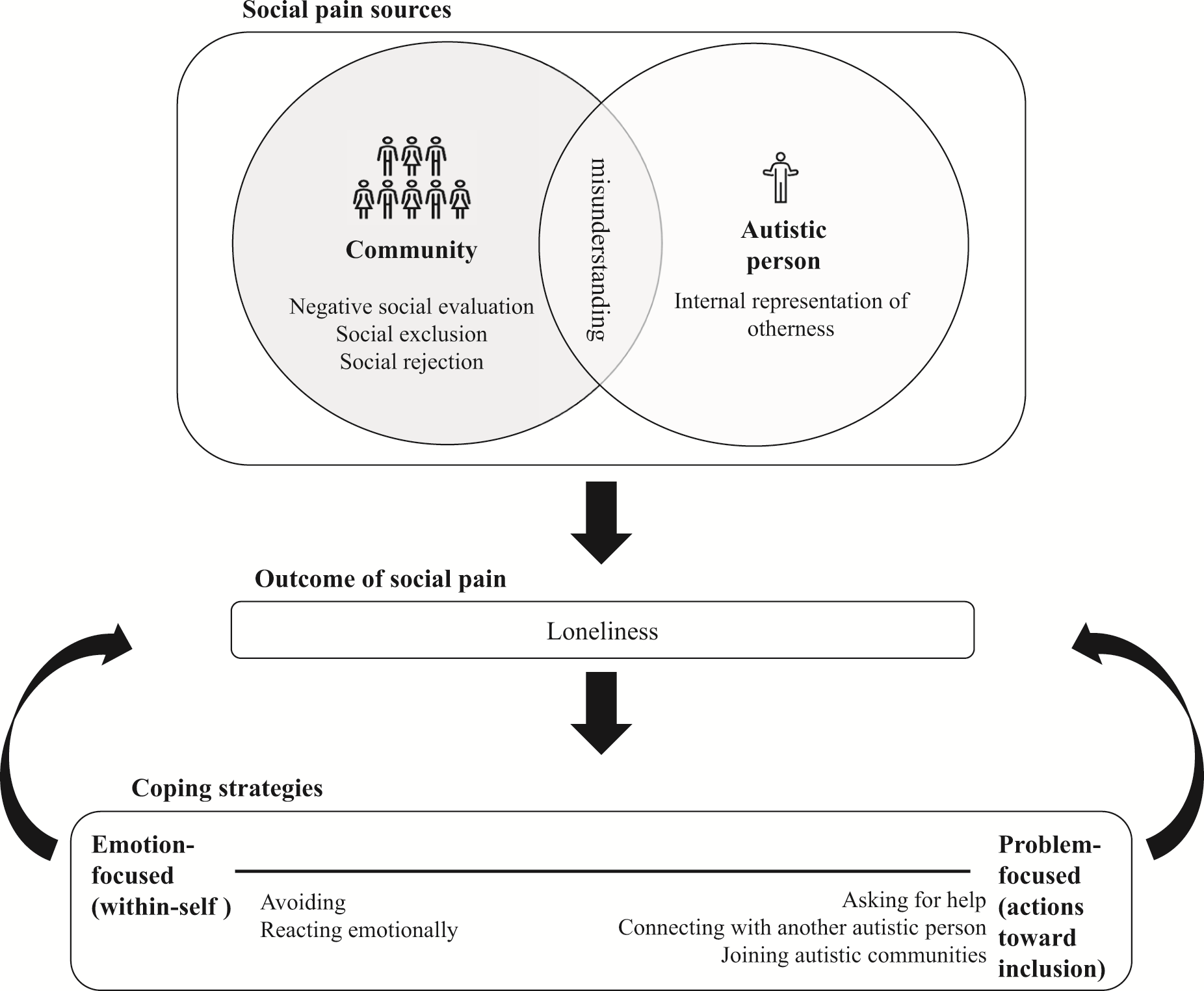
Summary of participants’ perceived social pain.
Theme 1: Definition
Participants acknowledged distinctions among physical, emotional, and social kinds of pain, and most described similarities and differences between them. For example, AA recognized that social insults cause social pain: “I feel social pain when I am offended or hurt. . . . It’s different from physical pain; it’s a separate category.” Participants referred to social pain experiences as more significant, long-lasting, and challenging to deal with than physical pain: “Physical pain is immediate, . . . ‘here and now,’ but does not last long. In contrast, social pain . . . hurts a lot more inside” (TC).
Although participants emphasized the distinction between physical and social pain, most defined social pain as a subtype of emotional pain. RS related to the context of emotionally hurtful interactions in his definition of social pain: “Emotional pain is divided into . . . pain that comes from emotional difficulty and social pain caused by difficulty communicating and having relations with others” (RS).
In describing the intense and lifelong pain, the participants used terms such as misery, suffering, leaving scars, and heartache. OK added her thoughts regarding social pain’s profound, long-lasting implications: “Words can leave deeper scars than a physical blow. A physical blow can heal; . . . words, on the other hand, offend, stay with you, and then decrease our self-confidence.” Many participants shared OK’s perception that it is easier to overcome physical pain than to live with social pain.
Theme 2: Sources
The second theme classifies social pain into three primary sources: (1) internal, within the autistic person (internal representation of otherness); (2) external, produced by the community (negative social evaluation, social exclusion and rejection); and (3) social misunderstanding (mutual misunderstanding between the autistic person and the community).
Internal Representation of Otherness
Participants reported being motivated to belong to a social group but believed that their ASD characteristics barred them from social inclusion. They internalized their belonging difficulties as representing the “otherness” that always accompanied them. “I look at people around me and realize I’m different. My brain works differently. . . . I don’t belong. Anywhere you put me, that will be my role” (NA).
The sense of otherness resulted in ongoing frustration. EK felt that she went out of her way to make friends to no avail and great disappointment because of her ASD traits and her differences in social skills: Sometimes I asked myself if I am God’s joke. . . . Even though I tried, I had a very hard time with friends my age. It was really frustrating! . . . The ASD is a hindrance. . . . Why is it that anywhere I go, I’m the one who doesn’t fit in? I experienced it as frustration and maybe even self-loathing. Yes, I guess I had these feelings of being defective.
Negative Social Evaluation
Most participants described negative social evaluation— manifested mainly in insults, embarrassing acts, and bullying—as another source of social pain. They emphasized the long-term pain resulting from past experiences of negative evaluation that affected their self-esteem. OM related hurtful words and attributed the amplified pain she experienced to her sensitivity: “It is hurtful when I’m offended. When someone says something unpleasant, it affects me a lot.” AK shared a painful social interaction when other classmates removed her belongings from her chair and sat in it instead of her: If I were someone else, they would not have allowed themselves to tell me to take my clothes away from the chair. I felt harassed. . . . There were not enough chairs so, of course, I was the one without a chair.
Similarly, some participants reported feeling they were easy prey for physical and verbal bullying: I was teased a lot. Boys’ teasing included little hits and blows, not very physically painful; mostly insulting. Girls’ teasing—whispering beyond my back and ridiculing—is a pain that stays with me to this day. They knew I wouldn’t fight back and took advantage of that. (EK)
An extreme example of negative social evaluation is ostracism. Several participants reported they had been ostracized; NC described verbal violence: It is worse than just being ignored; they ostracized me—called me names, talked about me behind my back, spoke with unpleasant tones. It was terrible. A group of girls treated me in the worse possible way. . . . Horrible things were said to me. Every word brought me down, and now I’m completely beaten.
Social Exclusion and Rejection
The participants described experiencing exclusion and rejection. They reported that their surroundings excluded them and kept them at an insulting distance. NA explained, “I just want to belong, but it feels like they put up a wall that I cannot pass.” Moreover, participants described conflicts between their attempts to belong and confronting active rejection in the social environment. OK recounted trying to create social connection, but her peers refused: “I just wanted to connect with my peers, but they said, ‘You do not belong. . . . Find yourself another group.’”
Social Misunderstanding
All participants mentioned social misunderstanding, including difficulty understanding others and others misunderstanding them. They described social misunderstanding as difficulty interpreting nonverbal communication. BF described, “I didn’t realize that if you hear them inside the house, and they don’t answer your knock, it’s a sign they don’t want you to enter.”
The immediacy and speed that characterize social interactions make them hard for autistic people to follow and understand. Participants reported understanding the social situation retrospectively. GM described, There were a lot of misunderstandings, and I couldn’t get what was going on. . . . Only after . . . I realized there was a gap between what I thought and understood and what the guys I met thought. It was too late.
Several participants mentioned ongoing changes in social rules as a cause of their social misunderstanding. Although others intuitively understand these rules of behavior, autistic people may struggle. EK vividly portrayed, Second grade is like a social turning point. Until then, you weren’t supposed to hit back. Instead, you should seek help from an adult. Then suddenly, in second grade, it is a “big no-no” to do that. Suddenly, if you go to an adult, it’s considered “telling,” which is very bad socially. No one talks about it; all the kids know you must not do that. It’s like everyone received a memo except me.
According to the participants’ accounts, the misunderstanding was mutual. They reported feeling unease when they misunderstood someone and offense when others did not try to understand or accept them: “I tried so hard to speak with new people, to make friends, but they didn’t understand me, they didn’t get me, and it always ended in heartache” (GM).
The participants described misunderstandings as usually beginning with the common misconception that autistic people do not want to be involved in the community and do not have empathy. EK described, When neurotypicals look at this from their perspective, they say, “Oh, sure! Autistic people aren’t empathic.” But that is a distorted interpretation. It’s not that we aren’t empathic; . . . it’s not that we don’t care. We are less aware of these signals. If I could identify that someone is sad, I would feel sad and want to help. Isn’t that empathy?
The gap between ASD characteristics as others interpret them and the inner world of autistic people is a source of social pain: We don’t know how to meet the other’s needs, . . . gain their cooperation and understanding. . . . Since we had so many bad experiences, even with close people, and because relationships are very painful, we don’t, in general, contact others. (BF)
Theme 3: Loneliness
Social pain results in an intense sense of loneliness. The participants’ words reflected that they gave up trying to contact people after painful experiences and somewhat lost their dream of having a friend: Throughout my life, in all my “conscious years,” I remember being lonely. I wanted to have friends; I hoped to be part of a “gang.” It never happened. For most of my life, I barely had one friend. I was alone, and it was extremely painful. . . . Terrible loneliness, yes. I have no friends, no one to visit or call or text. . . . I’m alone, and it’s hard. (GM)
Participants related the experience of being lonely to being transparent while wishing for at least minimal contact with others. “I felt so lonely. None of my friends even noticed I was alone and wanted some attention . . . . ‘Hey, she’s sad.’ But no one saw that. No one saw me” (OK). OK’s description reflected her basic social need for visibility, attention, and a reaching hand—and her great disappointment when it did not happen.
Another basic social need is to feel the close community’s protection. Like others, NC shared how her sense of loneliness resulted in feeling exposed and unprotected: “I had no friends. . . . They were in groups, and I was alone. It made me feel exposed. Anyone who wanted could give me a hard time, and I had no friends to protect me.”
The pain and stress of being rejected generated fear alongside vulnerability among the participants. GM provided insight into the problematic relationship between loneliness and reduced social participation with which participants coped in addition to social pain: School was one long, painful experience. I didn’t have any friends, but everyone around me had fun and were always together. I had no friends at all, although I tried, but no one ever reached out to me and wanted my company. I would stay in the classroom during recess from first grade to my senior year.
Theme 4: Coping Strategies
Participants’ strategies to cope with social pain can be categorized as inward or outward initiations toward social inclusion. Inward relates to negative or positive coping strategies directed toward oneself. At the extremely negative end are behaviors such as avoiding painful social situations, sporadic crying, and long-term depression. At the extremely positive end, the participants described a better self-understanding that affected their pain experiences and their acceptance of their diagnosis. Outward refers to coping strategies directed toward the community. These are active attempts by the autistic person to become part of the social structure by asking for help from people to whom they feel close or belonging to a group of autistic peers. Table 2 shows conceptualized strategies with example citations.
Strategies to Cope With and Gain Relief From Social Pain
Discussion
This study’s phenomenological approach achieved its twofold goal: gaining insight into the social pain of autistic people and strategies to overcome it. Participants used intense wording to describe social pain as a prevalent hurtful experience with a longer recovery time than physical pain. Their firsthand accounts are fundamentally important in unveiling the desire of autistic people for social contact and the meaning of social pain, which has barely been studied to date. Moreover, this study’s results also demonstrate that loss was not a main source of social pain, contrary to previous studies among neurotypical people.
Social Pain Model
The outlined model (see Figure 1) echoes the participants’ social pain in three main components: its sources, loneliness outcome, and coping strategies.
Social Pain Sources
Four major social pain sources were identified: internal representation of otherness, misunderstanding between autistic people and the community, feeling negatively evaluated, and feeling excluded or rejected. Although negative social evaluation and social exclusion or rejection are known general social pain sources (Eisenberger, 2012), this study identified the internal representation of otherness and social misunderstanding as unique sources of social pain for autistic people.
Internal Representation of Otherness
Many participants expressed feeling otherness, which caused a sense of not belonging enforced by repeated negative interactions. They were aware of their different information processing and perceived ASD characteristics as obstacles to social relationships. These reports align with previous qualitative research suggesting that autistic people notice that the community labels them as different and has a negative attitude toward them. As a result, they perceive themselves as deviating from the community’s expectations and norms (Ghanouni & Quirke, 2022; Kanfiszer et al., 2017).
This study’s participants used harsh words to describe themselves through the mirrors of their surroundings and self-perceptions. None described themselves with positive words or strengths; all elaborated on their challenges and limitations. This finding might be affected by the fact that the participants knew they were going to be interviewed regarding pain experiences. Hence, this finding does not indicate that the whole autism identity of the participants is negative. Rather, this finding emphasizes the importance of awareness of the pain in self-definition and the need for health care professionals to address this pain.
Previous studies demonstrated that health care providers who assist clients in identifying their strengths promoted quality of life (Wallace et al., 2021). The Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association [AOTA], 2020) emphasizes identifying the client’s strengths as part of a client-centered practice to promote interventions better suited to the client and effect targeted outcomes. Moreover, supporting the identity formation process toward embracing positive and negative features may assist autistic people in improving their self-advocacy skills (Ghanouni & Quirke, 2022), which is a major intervention goal of occupational therapists (AOTA, 2020).
Misunderstandings Between Autistic People and the Community
This study reveals three significant insights regarding misunderstandings between people with ASD and the community. Specifically, autistic people (1) are interested in social relationships, (2) feel prevented from social relationships because of their autistic traits along with their sense of otherness, and (3) feel ongoing frustration caused by others’ incorrect perceptions of them as uninterested in social communication.
Participants described social issues, such as challenges in understanding nonverbal language, initiating communication, and recognizing and adapting to changes in social rules. These challenges have been widely addressed in previous literature (APA, 2013; Cummins et al., 2020; Hus & Segal, 2021). The difficulty in understanding others may relate to the theory of mind (ToM). This theory is controversial and refers to the ability to evaluate others’ behavior on the basis of one’s mental states, causing some degree of “mind-blindness” (Baron-Cohen, 2000; Fernández, 2013). Because of ToM difficulties, autistic people may find other people’s behavior confusing, unpredictable, and frightening (Baron-Cohen, 2000).
Participants also described major difficulties in navigating social rules, which are unspoken and often change across contexts. The dynamic nature of social rules challenges autistic people (Cage et al., 2016), who, by definition, tend to adhere to routines and are less flexible with transitions (APA, 2013).
Previous studies demonstrated inconsistent evidence regarding autistic people’s level of interest in social interaction (e.g., Causton-Theoharis et al., 2009; Deckers et al., 2014). However, in this study, most participants described the presence of deep misconceptions about them as not being interested in social relationships. They perceived this misconception as false and a barrier to creating and sustaining relationships, resulting in social pain.
The participants also addressed the community’s misunderstanding regarding the needs of autistic people. Previous reports from autistic people that highlight the community’s frequent misinterpretations of the behaviors of autistic people and tendency toward inaccurate generalizations about their challenges and abilities support this finding (Ghanouni & Quirke, 2022).
Negative Social Evaluation
Participants reported a wide span of negative social evaluations (e.g., manifested in swearing, bullying, and ostracism) that caused them social pain. Previous studies of autistic youth addressed similar experiences but did not consider their implications for social pain (e.g., Hebron & Humphrey, 2014; Trimmer et al., 2017). For example, Hoover and Kaufman (2018) demonstrated that autistic adults were at an increased risk of adverse childhood experiences, including bullying, that can negatively affect physical and mental health.
According to the need–threat model, ostracism among the general population threatens fundamental human needs for belonging, self-esteem, control, protection, and meaningful existence and may lead to resignation, alienation, helplessness, depression, and social pain (Williams, 2009). The research on autistic adults has revealed a gap between physiological arousal and insignificant behavioral and emotional responses to ostracism in questionnaires (Trimmer et al., 2017). This study found that autistic people feel social pain as a result of negative social evaluation. The discrepant responses to negative social evaluations between Trimmer et al.’s (2017) study and ours may be due to the different presentation of questions (i.e., questionnaire vs. interview). Another cause may be the characteristic information-processing features of ASD (i.e., immediate vs. retrospective reports).
To promote better social participation, occupational therapy practitioners should initiate both prevention interventions, to decrease the community’s social devaluation, and ad hoc treatment of autistic people who experience social devaluation (AOTA, 2020)
Social Exclusion and Rejection
Eisenberger (2012) included the social exclusion and rejection component in the social pain definition. Most participants expressed feelings of exclusion and rejection but distinguished between the two. They used exclusion to convey intended distancing from and prevention of social involvement (the autistic person is passive; the community is active) and rejection to express the community’s refusal in response to the participants’ social initiations (both the autistic person and the community are active). Some previous studies have suggested that autistic people have decreased social exclusion and rejection responses compared with neurotypical people (e.g., Bolling et al., 2011; Silva et al., 2020). However, this study’s results suggest that autistic people generally have intense emotional responses to social exclusion and rejection and experience social pain as a result.
As a part of promoting the enhanced social participation of autistic people, occupational therapists should help them improve their strategies for establishing relationships. In parallel, occupational therapists can also support the community to better understand and integrate autistic people.
Loneliness as a Social Pain Outcome
Most participants reported that negative social interactions, including rejection, exclusion, negative evaluation, and social misunderstanding, caused them a sense of loneliness. These findings align with previous studies that have found that autistic people experience loneliness across the lifespan (e.g., Bauminger et al., 2003; Deckers et al., 2017).
Bauminger et al. (2003) found that autistic children spend less time interacting with peers than their neurotypical counterparts. This finding may be linked to several participants’ reports in our study distinguishing between loneliness and solitude. The significant difference is the possibility of choosing whether to be alone. Participants reported a need for solitude from time to time, being alone to regulate and reorganize themselves. However, they felt lonely, helpless, and deeply hurt when facing social neglect or exclusion and rejection. Similarly, but less specifically, Ee et al. (2019) reported a differentiation between loneliness and being alone among autistic people. This study’s result also strengthens and expands Elmose’s (2020) qualitative study. Elmose (2020) reported that the gap between desired and actual social relationships caused loneliness among autistic adults and attributed the gaps to several factors (e.g., the community’s misunderstanding of autistic people) also reported in our study.
Mazurek (2014) associated loneliness among autistic adults with increased depression and anxiety along with decreased life satisfaction and self-esteem. Those findings align with the participants’ descriptions in our study regarding significant emotional implications, including a sense of vulnerability and decreased self-esteem. Previous studies associated decreased loneliness among autistic people with their participation in social skills intervention programs, positive views, and acceptance of themselves (Umagami et al., 2022). The last two factors emphasize the importance of focusing on identity formation alongside classic interventions for social skills improvement.
Coping Strategies
Inward Strategies
Participants articulated four inward (self-directed) coping strategies: (1) experiencing feelings such as embarrassment and sadness; (2) emotional response, including behaviors such as crying; (3) avoidance, expressing extreme emotional control; and (4) self- understanding, an internal process that strengthens individual self-acceptance and promotes self-advocacy. Previously, Bitsika and Sharpley (2014) demonstrated a high frequency of emotional implications as strategies that autistic children used, albeit ineffectively, in response to negative social evaluation (bullying). These included experiencing feelings (e.g., sadness, nervousness, fear) and resultant behaviors (e.g., crying, tantrums, sleep difficulties).
The participants in our study reported repeated social pain experiences as their motivation for avoidance, specifically giving up opportunities to be involved in meaningful relationships. The process they described corresponds to the literature regarding physical pain, wherein pain signals prompt, quick responses to terminate threatening stimuli (Eisenberger, 2012). Avoidance often characterizes anxiety disorders, with a heightened focus on possible harm. Anxiety is rooted in fundamental concerns about the possibility of physical harm (thus, physical pain) and social harm (thus, social pain; Beck et al., 1974). This link is meaningful because anxiety is common among autistic people (Nimmo-Smith et al., 2020), increasing their likelihood of choosing social avoidance. Khanna et al.’s (2014) study linked avoidance, as a coping strategy, to lower mental health. Avoidance, which is negatively driven, is opposed to self-understanding, which positively influences the social pain experience.
In this study, self-understanding refers to autistic individuals’ insights and knowledge of their identity. Many participants referred to receiving their ASD diagnosis late in life as a life-altering event. The diagnosis shed light on the reasons for the social struggle and social pain they had been coping with throughout their lives.
Receiving a late diagnosis has been defined as a coping strategy specific to autistic people. Participants in recent studies (e.g., Dachez & Ndobo, 2018; Leedham et al., 2020) reported diverse emotions after receiving their diagnosis, including relief, validation, and self-understanding. Better self-understanding may serve as a starting point for generating and implementing coping strategies and self-advocacy. It may indicate the positive effect of the diagnosis on the social pain experience (Dachez & Ndobo, 2018).
Outward Strategies
Participants in this study reported asking for help, mainly from family members. Only 1 participant mentioned her occupational therapist as a source of support and assistance in the context of social pain. This might be because only a minority of participants reported involvement with occupational therapy treatment or the occupational therapists focused mostly on instrumental activities of daily living, leisure, and employment and less on social interventions for autistic adults.
The participants also reported forming a connection with another autistic person and joining autistic communities as outward coping strategies. Only a few previous studies related this coping strategy; for instance, Dachez and Ndobo (2018) described seeking support from family and friends. Our study points to the need to address occupational therapy intervention programs to autistic people, particularly those aimed at developing or improving the skill of asking for help in the social context to prevent or solve social pain experiences.
Several studies described the preference of autistic people to be involved in relationships with others with ASD. Chen et al. (2021) found that autistic people were more likely to interact with peers who were autistic than with those who were not. They were involved in social interactions characterized by sharing thoughts and experiences and high reciprocity to create and maintain relationships. Such involvement in peer interactions in the context of intervention programs and spontaneously joining autistic communities had positive implications, including an enhanced sense of belongingness, reduced loneliness, and better quality of life (e.g., Lam et al., 2020; Spain & Blainey, 2015). These results support a growing call for peer support interventions for autistic people (Umagami et al., 2022).
Occupational therapists seek to support clients’ participation in daily living, which results from the dynamic intersection of clients and their desired engagements and contexts (AOTA, 2020). Therefore, occupational therapists should pay attention to the fact that autistic adults are less likely to be involved in their social surroundings: They no longer go to school, and many are unemployed (Umagami et al., 2022). It is essential to consider how to elevate their social support and alleviate feelings of loneliness.
Limitations
This study’s sample was relatively small and homogeneous (i.e., cognitively able adults with fewer service needs). Moreover, the sample had a higher ratio of female participants than the current gender distribution among people with ASD. Despite the sample size and gender distribution, participants provided rich experiences and insights that enabled us to suggest a valid conceptualization using a thorough and trustworthy qualitative procedure.
Implications for Occupational Therapy Practice
This study’s findings point to occupational therapists’ meaningful role in promoting bilateral intervention programs to prevent and solve social pain experiences. The programs’ bilateral nature could assist (1) autistic people to improve their coping strategies of self-understanding, advocacy, and social skills and (2) the community to promote understanding and acceptance, including skills for mediating and reducing misunderstanding.
Conclusion
This article adds a novel theoretical model that represents the social pain phenomenon echoed by autistic people and their strategies for overcoming it. The model enforces well-known theoretical concepts related to social pain and adds unique insight into the mutual misunderstanding between autistic people and the community. Their adaptive and less adaptive coping strategies determine how they solve their loneliness and social pain.
This study raises awareness of the gap that some autistic people experience between their need for social interactions and the social pain they experience in its absence. It calls for intervention programs to prevent or solve social pain experiences on two fronts (i.e., bilateral programs): (1) improving the coping strategies of self-understanding, advocacy, and social skills of autistic people and (2) promoting the community’s understanding and acceptance, including skills to mediate and reduce misunderstandings.