
Abstract
A task-oriented, home-based Cognitive Orientation to Daily Occupational PerformanceTM (CO-OP) intervention can be effective in helping older adults return home successfully after a hip fracture.
A hip fracture is the most serious osteoporotic fracture among people older than age 65 yr (Rapp et al., 2019), and it is the second most common reason for hospitalization (Brauer et al., 2009). In addition to impairing activities of daily living (ADLs), hip fractures have a severe negative impact on quality of life (Rasmussen & Uhrenfeldt, 2016). Rehabilitation programs are designed to help people who have had a hip fracture reintegrate safely into community life (Leland et al., 2015). However, even people who are independent in ADLs struggle in doing so (Gilboa et al., 2019), and 1 yr after discharge, most patients are not able to sustain their rehabilitation achievements (Hershkovitz et al., 2012). Therefore, an individualized, holistic, progressive, long-term postrehabilitation intervention program to prevent functional decline is needed (Amling et al., 2014). In Israel, rehabilitation was traditionally conducted in inpatient facilities; however, as part of the growing trend of providing health care services in the community, patients now have the option of undergoing rehabilitation at home (Gagin et al., 2020).
In-home therapy provides the opportunity for rehabilitation intervention to be completed within the context of the patient’s natural environment (Stolee et al., 2012), and it has the added value of supporting the patient in finding new routines for performing their everyday activities (Gilboa et al., 2019; Pol et al., 2019). In addition, home-based rehabilitation can help reduce overall costs to the health care system by decreasing the patient’s length of hospital stay without impeding recovery (Stolee et al., 2012). A recent meta-analysis showed that home-based rehabilitative interventions had a positive, although not statistically significant, effect on function after a hip fracture (Chen et al., 2020). However, most studies have focused on the effects of physical exercise, leaving a gap in understanding the effectiveness of a more task-oriented intervention that address individual preferences (Chen et al., 2020; Copanitsanou, 2019).
The Cognitive Orientation to daily Occupational PerformanceTM (CO-OP) approach is a client-centered, occupation-based intervention aimed at improving performance in everyday life activities and by that reflects a paradigm shift from traditionally used rehabilitation exercises to an occupation-centered intervention. The CO-OP approach involves a structured problem-solving framework, using a global strategy of Goal–Plan–Do–Check (Rodger & Polatajko, 2017). The CO-OP approach has been extensively studied and applied to a variety of populations (Scammell et al., 2016), including older adults (Borujeni et al., 2019). Supporting the generalization and transfer of skills is a key aspect of the CO-OP approach. Hence, using this method may enable patients to maintain rehabilitation achievements and prevent deterioration.
To our knowledge, no study has yet assessed the use of the CO-OP approach for patients after a hip fracture. Because poor patient compliance is an unavoidable problem in home-based rehabilitation after a hip fracture (Chen et al., 2020), the purpose of this pilot study was to determine the feasibility of the CO-OP intervention delivered in the home for older adults after a hip fracture and to evaluate its preliminary effectiveness in improving functional outcomes.
Method
Study Design
A single-arm quasi-experimental design was applied.
Participants
Nine participants were recruited from an inpatient rehabilitation ward in a geriatric hospital in a central city in Israel. Eligible participants were age 65 yr or older, were in a chronic stage of recovery after a hip fracture, had been discharged from rehabilitation into a community setting, and were independent in basic ADLs at the time of discharge (FIM® score >90; Keith et al., 1987). 1 Exclusion criteria were severe cognitive impairment (Mini-Mental State Examination score <20; MacKenzie et al., 1996) and the presence of other health conditions that might interfere with participation in the study.
Measures
The medical and personal details were collected on the basis of responses to a demographic questionnaire. The Canadian Occupational Performance Measure (COPM; Law et al., 2014) was used to measure performance and satisfaction with the patients’ level of participation in daily functioning regarding the five most important problems identified, each rated on a 10-point scale (1 = not able to do it at all/not satisfied at all to 10 = able to do it extremely well/extremely satisfied).
The COPM is a widely used tool that has excellent test–retest reliability (≥.75), is well validated, and is sensitive to changes in function in patients recovering from a hip fracture (Edwards et al., 2007). In addition, participants were asked about their general satisfaction with the intervention (scored from 1 = very low to 5 = very high).
Procedure
The study was approved by the ethics review committee of Herzog Hospital’s institutional review board. Eligible patients were invited by the study coordinator to participate. After signing an informed consent form, an occupational therapist performed the baseline assessment and the intervention. To reduce bias, the postintervention assessment was performed after the last intervention session by a different occupational therapist. In addition, all participants completed the 3-mo follow-up assessment. All assessments were performed at the participants’ homes and took up to 1 hr to complete.
The intervention was administered by a CO-OP– trained occupational therapist (Esther Appleton), including up to 10 face-to-face 1-hr weekly CO-OP sessions. As a basis for the intervention, each participant set five goals using the COPM. Three of the five goals were addressed directly during therapy (trained), and the other two goals were not addressed (not trained). Monitoring performance and satisfaction of untrained goals enabled assessment of generalization and transfer of learning. For each goal, the participant was guided by the therapist to form a plan to achieve that goal. Between each session, the participant was guided to do the plan and report back in the following session—that is, check to see whether the plan worked and the goal was attained. If the goal was not achieved, the participant was guided to analyze what went wrong and to identify a new potential plan, and the process was repeated (Mandich & Polatajko, 2004).
Statistical Analysis
Descriptive statistics on the participants’ characteristics and the acceptability of treatment were obtained. The recruitment rate was determined by dividing the number of participants who started the intervention by the number of participants who were assessed for eligibility. The retention rate was defined as the number of participants who remained in the study at the last wave of data collection as a proportion of the total number of participants recruited at the baseline assessment. The recruitment and retention rates were considered feasible if the recruitment rate exceeded 15% and if the retention rate exceeded 75% (Tunur et al., 2020). We conducted a nonparametric Friedman test with automatic Bonferroni correction to determine whether there were differences in the assessments’ outcome measures from baseline to postintervention and at a 3-mo follow-up. The significance level was set at p = .05.
Results
Feasibility
The flow diagram in Figure 1 provides details regarding the process of enrollment, intervention, and assessments. Thirty-three potentially eligible patients were referred to the study and assessed for eligibility, 11 of whom started the study (recruitment rate of 30%). One participant dropped out during the baseline assessment, and one dropped out in the middle of the intervention after three sessions (81% retention rate). Nine participants completed the intervention program and the postintervention assessments. The participants were 2 to 6 mo post–hip fracture (8 women; M age = 79.55 yr, SD = 7.84, range = 70–95). Three of the participants lived alone. None of the participants received additional occupational therapy during the intervention period.
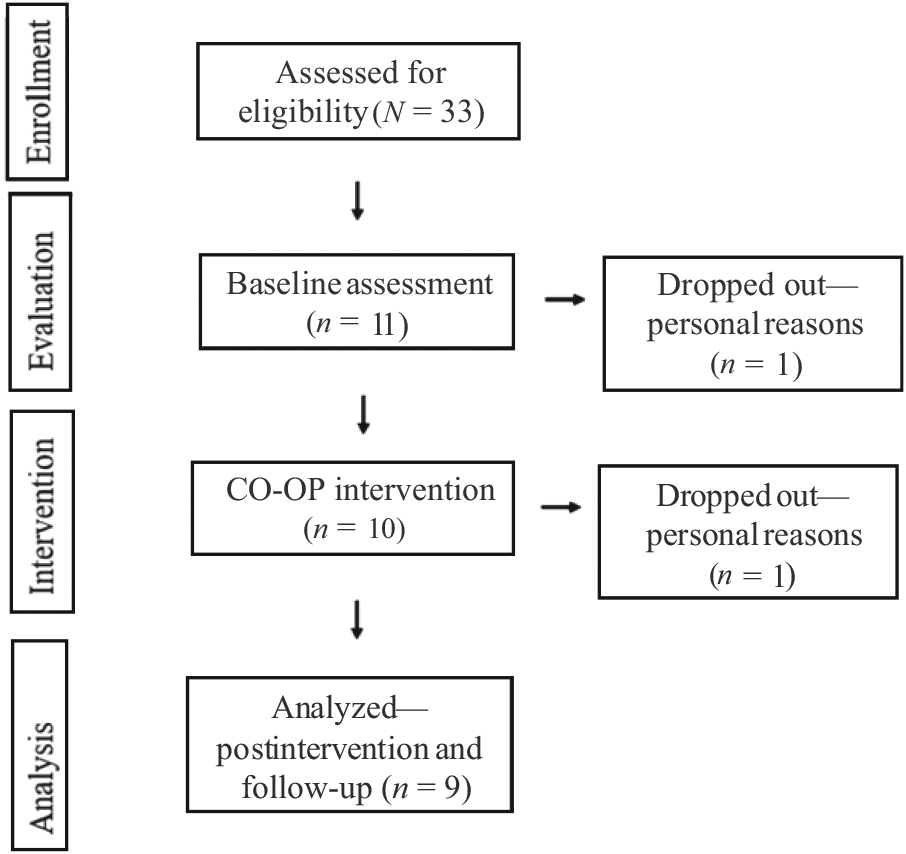
Flow diagram: Enrollment, intervention, and assessment.
Participants set goals focused on self-care (e.g., shop for groceries independently and cook meals independently), leisure (e.g., walk to the park once a week with a friend and return to swim in the local pool), and productivity (e.g., return to volunteering or paid work three times per week). Participants who completed the intervention program received 4 to 10 CO-OP sessions (M = 7.33, SD = 2.29). No adverse events related to the intervention were reported. Overall, the acceptability of the intervention was high, with 88% of the participants expressing high to very high satisfaction with the intervention in general.
Preliminary Efficacy
Examination of the total clinically meaningful improvements (indicated by a change of ≥2 points on performance ratings on the COPM) suggested two main findings. First, the performance and satisfaction improvements that were achieved at postintervention were mostly maintained at follow-up. Second, improvement was shown both for trained and untrained goals (Table 1).
Number of Goals That Reached Clinically Significant Improvement on the COPM (≥2 points)
Note. COPM = Canadian Occupational Performance Measure.
As can be seen in Table 2, the Friedman tests results indicated statistically significant improvements from baseline to postintervention in COPM performance and satisfaction scale ratings on trained goals and untrained goals. A post hoc analysis of the COPM Performance and Satisfaction scales revealed statistically significant differences on the trained goals from pre- to postintervention (p = .04) and follow-up (p < .001), but not for the postintervention and follow-up phases. The same trend was found for the untrained goals.
COPM Performance Across the Baseline and Endpoint Evaluation Sessions
Note. COPM = Canadian Occupational Performance Measure; IQR = interquartile range.
Discussion
This pilot study is the first to assess the feasibility of the CO-OP approach in a home-based intervention format among older adults after a hip fracture. The results indicate that it was feasible to deliver the intervention in the home of the participants while adhering to the essential elements of the CO-OP approach. Recruitment and retention rates in the current study are comparable with the rate reported previously in home-based physiotherapy intervention among older adults after a hip fracture (Magaziner et al., 2019) and CO-OP intervention in a telerehabilitation format with adults and older adults after an acquired brain injury (Beit Yosef et al., 2019).
Despite the small sample, statistically and clinically significant gains were achieved postintervention for most of the trained and untrained goals. Significant gains in most goals were found at a 3-mo follow-up assessment. These results have been documented in previous studies, suggesting that the participants successfully transferred the strategies practiced on the trained goals to the untrained goals and that changes were maintained over time (Beit Yosef et al., 2019; Borujeni et al., 2019; Dawson et al., 2014).
The results of this exploratory study need to be interpreted with caution because of some limitations. First, this was a pilot study with a small sample size and no control group, which means that postintervention improvements likely were influenced by other factors and therefore cannot be attributed solely to the treatment. In addition, we used the COPM, which is a self-report tool. Future studies should combine this tool with a performance-based measure to strengthen the results. In light of these limitations, further research is warranted with a larger sample and a control group.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: ▪ The CO-OP intervention appears feasible to deliver at home to older adults returning home after hip fracture. ▪ Home-based CO-OP may improve occupational performance and satisfaction among older adults with hip fractures who are discharged home.
Conclusions
The current findings suggest that home-based occupational therapy intervention is feasible, acceptable, and potentially beneficial for older adults returning home after a hip fracture. Despite the small sample size, clinical and statistically significant improvements in activity performance were found and mostly maintained at a 3-mo follow-up.
Footnotes
1
FIM® is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
Acknowledgments
We thank the participants and their caregivers. This work was supported by funds from the Israel National Institute for Health Policy Research and the Israel National Institute for Health Policy and Health Services Research (No. 2016/191/A). This study was registered at ClinicalTrials.gov (NCT03376750; December 15, 2017).