
Abstract
Problem-Solving Training (PST) during inpatient rehabilitation is feasible and the results of this study suggest that patients with stroke may have the ability to identify problems, set goals, and develop plans to accomplish goals.
In the United States, 7 million people currently live with poststroke disability, with a projected increase of 4 million by 2030 (Heidenreich et al., 2011), and approximately 70% of the 1 million people who experience stroke annually are discharged home (Reeves et al., 2017). This transition to the community is associated with multiple emotional, social, and health-related challenges that are intensified by abrupt lifestyle changes for stroke survivors and their caregivers (Grant et al., 2004). Stroke survivors often report feeling ill equipped to manage challenges that come with their transition from the hospital to the community after stroke (Grant et al., 2004). Information alone does not adequately prepare them to manage this transition (Laver et al., 2010). However, patients and families who participate in problem- solving skill building before discharge, compared with those who do not, feel better prepared and have significantly higher self-efficacy during this transition (Portillo et al., 2009). Goal setting is foundational to problem-solving techniques. People identify a problem and learn to set measurable goals that, when met, indicate achievement: overcoming the barrier or barriers that caused the problem (Akama, 2006). Actively participating in goal setting early in the rehabilitation process and possessing the problem-solving skills required to achieve those goals decreases depression and increases self-efficacy, functional independence, and quality of life after a stroke (Skidmore et al., 2015 ; Stroke Foundation, 2017). Current guidelines state that patients with stroke should be actively involved in goal setting early after stroke (Stroke Foundation, 2017), and most patients are able to participate in collaborative goal setting on the acute stroke unit (Laver et al., 2010). However, collaborative goal setting occurs infrequently in the current health system (Wressle et al., 1999). To address this gap for patients with stroke, we examined the feasibility of implementing Problem-Solving Training (PST) during the inpatient rehabilitation unit (IRU) stay, followed by weekly mobile boosters that are designed to support goal setting after discharge.
PST (D’Zurilla et al., 2004) teaches a metacognitive problem-solving strategy by guiding a person through a simple method for evaluating problems; generating and selecting solutions; and developing, evaluating, and revising goals and action plans. PST is rooted in Social Problem-Solving Theory, which proposes that real-world problem solving requires the ability to develop solutions to problems and to implement those solutions. Like PST, Cognitive Orientation to daily Occupational Performance (CO–OP; Ahn et al., 2017) teaches a metacognitive strategy that is focused on skill acquisition, whereas PST is focused on promoting coping skills. Problem-solving interventions such as PST and CO–OP have been studied in several clinical populations—including patients with stroke—to address functional independence, anxiety, depression, productivity, self-regulation, and metabolic variables (Skidmore et al., 2015; Villamil-Salcedo et al., 2018). Among patients with stroke, Skidmore and colleagues (2015) demonstrated that CO–OP during inpatient rehabilitation significantly improved independence in performing activities of daily living. A randomized controlled trial of 166 outpatients with stroke who received PST demonstrated significant improvement in task-oriented coping at 6 mo postintervention compared with controls (p = .008; Visser et al., 2016). Although these studies suggest that problem-solving approaches are learned quickly and maintained over time, ongoing intervention over time may improve long-term use of problem-solving strategies.
Mobile health (mHealth) has the potential to increase health care accessibility, promote self-management, provide evidence-based education, and support the self-monitoring of biometrics in rehabilitation populations (World Health Organization Global Observatory for eHealth, 2011). The increasing availability of smartphones (Anderson & Perrin, 2017) presents a unique opportunity to support the long-term use of problem-solving strategies by providing a scalable way to maintain ongoing contact and boost effects of PST after formal training is complete. This may be particularly beneficial for supporting patients in their use of PST across the transition from hospital to community.
The purpose of this study was to determine (1) the feasibility of PST during an IRU stay for patients with stroke and (2) the feasibility of promoting PST strategy use postdischarge using mHealth after PST. To accomplish this, we followed the Obesity-Related Behavioral Intervention Trials (ORBIT) model of behavioral treatment development to guide our study design and objectives. ORBIT is a systematic framework of four phases of behavioral treatment development (Czajkowski et al., 2015). Our study falls under ORBIT Phase IIb (pilot testing), a feasibility pilot in which the goal is to determine the logistical feasibility of a future clinical trial by providing information on screening to enrollment ratios, dropout, acceptability of the intervention to the target population, and estimates of the clinical outcomes (e.g., depression, self-efficacy).
Method
Overview and Design
We conducted a single-group feasibility study of PST during the IRU stay of patients with stroke. A trained interventionist, an occupational therapy student, delivered PST to patients in the IRU. The student was trained by the first author (Candice L. Osborne) using a previously developed training protocol developed by the third author (Shannon B. Juengst), who has led multiple PST studies and developed the training protocol, which will be included in the final training manual (Juengst, Silva, et al., 2019). Interventionist training consisted of a combination of didactic instruction, self-study, and active practice with feedback. A member of the study team used a previously developed checklist to assess fidelity, screening 10% of the audio-recorded sessions. Intervention delivery adherence and competence were measured. A description of the fidelity checklist and calculations used were previously published by Juengst, Silva, et al. (2019). Participants received up to six PST sessions. If they were unable to complete all PST sessions during their IRU stay, the final session was completed over the phone within 1 wk of IRU discharge. Sessions were generally scheduled in the late afternoon in the patient’s room. Only the patient and interventionist were present. Outcome assessments were conducted at baseline, at the completion of PST, and at 3 mo postdischarge (final assessments were completed electronically or by phone). Postdischarge, participants received weekly text messages or emails for 3 mo that contained a link to the RedCap-based goal-setting boosters. Boosters prompted participants to set goals and report goal accomplishments once a week. The University of Texas Southwestern Medical Center Institutional Review Board approved all research procedures, and the participants provided informed consent.
Participants
Participants were patients who had received a primary diagnosis of stroke and who had been admitted to an IRU at an academic or county hospital. Electronic medical records were screened daily, and patients were approached about the study if they met the following criteria: (1) less than 4 wk since stroke, with a planned discharge home; (2) English fluency; (3) age 18 yr or older; (4) a Western Aphasia Battery score of 50 or higher; (5) a Montreal Cognitive Assessment (MoCA) score of 20 or higher; (6) the capacity to self-consent; and (7) the ownership of, and ability to use (independently or assisted), a smartphone.
Measures
To characterize the sample, we collected data on age, sex, race, ethnicity, education, and stroke severity using the National Institutes of Health Stroke Scale. Feasibility data (on discharge from the IRU; Aim 1) included the following: (1) number of participants recruited, (2) number and percentage of patients who consented, (3) reasons for refusal, (4) number of PST sessions completed, (5) length of sessions, and (6) scores on the Client Satisfaction Questionnaire–8 (CSQ–8; Atkisson & Greenfield, 1999), a validated self-reported measure of satisfaction with health- related services. At baseline, on discharge from the IRU, and at 3 mo postdischarge (Aim 1), we collected data using (1) the General Self-Efficacy Scale (GSE), a 10-item self-report measure of self-efficacy as it relates to coping with stressful events, validated with a wide range of rehabilitation populations (Luszczynska et al., 2005), and (2) the Patient Health Questionnaire–8 (PHQ–8), an eight-item questionnaire validated among patients with stroke (Trotter et al., 2019) that measures the frequency of eight symptoms from the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; American Psychiatric Association, 2000) that define a major depressive episode in the past 2 wk. Goal Attainment Scaling (GAS; Kiresuk & Sherman, 1968) was conducted on discharge from the IRU (Aim 1) and weekly for 3 mo (Aim 2). GAS is a method for developing patient-centered goals and measuring goal achievement that has demonstrated validity, reliability, and sensitivity in an IRU population (Malec, 1999). At 3 mo postdischarge from the IRU, we also collected data using the Telehealth Usability Questionnaire (TUQ; Aim 2), a 21-item questionnaire that has been validated across a range of clinical patient populations and measures technology usefulness, ease of use, effectiveness, reliability, and satisfaction (Parmanto et al., 2016).
Problem-Solving Training Intervention
PST is a metacognitive strategy technique, which means that the training focuses on a systematic approach to thinking through the steps of problem solving rather than focusing on solving a specific problem. PST was provided in addition to regular inpatient rehabilitation treatment and consisted of up to six sessions (30–45 min each) that follow a structured format (for session content, see Table 2; Juengst, Silva, et al., 2019). Under the guidance of the interventionist, participants applied the ABCDEF steps of PST (Assess, Brainstorm, Consider and Choose, Develop and Do, Evaluate, and Flex) to develop specific action plans to overcome barriers to the goals they choose. The Discharge Planning Assessment Tool (DPAT; Texas Woman’s University, 2020) was administered during Session 2 to identify specific areas where the patient perceived the potential for problems or barriers that might impede a successful transition from hospital to home.
Participant Characteristics
Note. ADL = Activities of Daily Living; IADL = Instrumental ADL (IADL functions were measured with a modified version of the Caregiver Appraisals of Functional Dependence; scores ranged from 1 [total dependence] to 7 [total independence]); NIHSS = National Institutes of Health Stroke Scale (scores ranged from 0 to 42; 1–5 = mild, 5–14 = mild to moderately severe, 15–24 = severe, >25 = very severe); w/d = withdrew.
PST Session Content
Note. The ABCDEF steps of Problem-Solving Training (PST) are Assess, Brainstorm, Consider and Choose, Develop and Do, Evaluate, and Flex. DPAT = Discharge Planning Assessment Tool.
Electronic Boosters
Electronic boosters consisted of weekly check-ins where participants stated whether they achieved their goal for the week (responses were “yes,” “no,” or free text). If they did not accomplish the goal, they were provided a drop-down menu from which they could select a reason why they did not accomplish the goal, or they could provide a free-text answer. The third prompt asked whether the participant would like to continue working on the previous week’s goal or create a new goal. If the participant created a new goal, they were prompted to describe the new goal using free text. Weekly boosters took approximately 5 min to complete.
Statistical Analysis
To describe feasibility, we report the number and percentage of recruited participants, number of participants who gave consent, reasons for ineligibility, reasons for refusal, and number and length of PST sessions. To identify a change in clinical outcomes, we present the average preintervention–postintervention changes in scores for depressive symptoms (on the PHQ–8) and self-efficacy (on the GSE) for changes both from baseline to discharge and from baseline to 3 mo postintervention. We also present the summary statistics (M ± SD) of participant satisfaction with PST (recorded using the CSQ–8). For Aim 2, we present the percentage of attained goals (recorded using GAS) out of all the attempted goals for each participant’s summary statistics (M ± SD) for technology usability (recorded using the TUQ).
Results
Feasibility of the Intervention
Figure 1 shows the flow of participants through the study, from the total number of patients who were screened between October 2019 and June 2020 to the total number who gave consent, with reasons for ineligibility and refusal. Compared with the patients who were screened, those who gave consent were more likely to be African American and less likely to be Hispanic. Table 1 presents demographic information for participants who consented. Four (27%) participants withdrew: 1 after three PST sessions; 1 after discharge, stating that she did not want to participate any further; and 1 for unknown reasons during the first PST session. We withdrew 1 participant because of worsening medical conditions that affected her cognition before the first PST session. Of those who did not withdraw, 1 was lost to follow-up at 3 mo. Eleven participants completed three or more PST sessions. The PST sessions lasted, on average, 30.46 min.
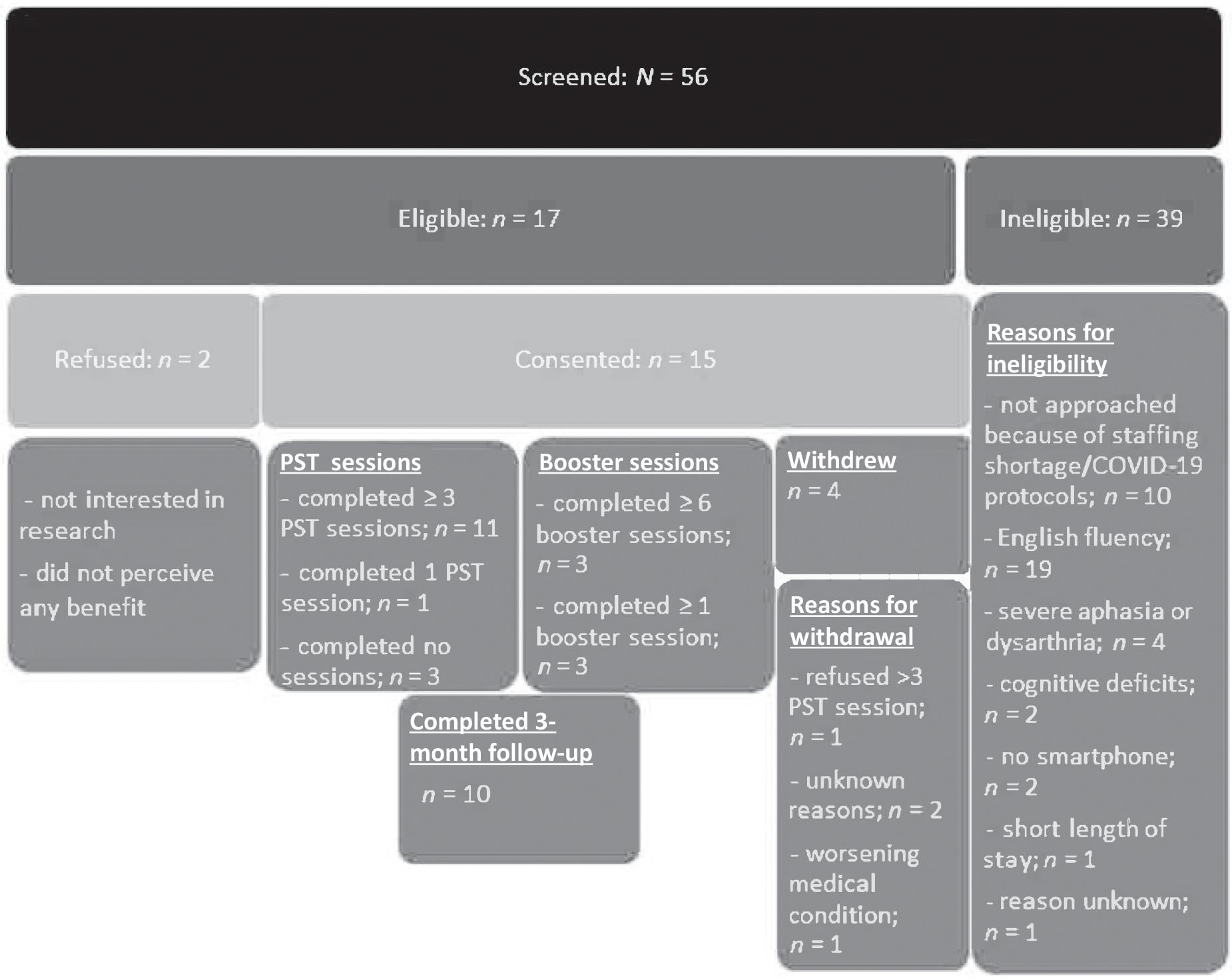
Participant flowchart.
Participants (n = 10) were generally very satisfied with PST (CSQ–8, M = 29.3, SD = 4.4). Participants reported moderate depression, on average, at baseline (PHQ–8; M = 11.0, SD = 6.1), decreasing to mild depression at the time of discharge (M = 5.6, SD = 3.8) and at 3 mo postdischarge (M = 8.3, SD = 5.5). Participants rated their self-efficacy at baseline as moderately high (GSE; M = 31.1, SD = 7.3), with an increase at the time of discharge (M = 36.2, SD = 3.3) and at 3 mo postdischarge (M = 34.1, SD = 4.2). Figure 2 shows changes in depression and self-efficacy scores from pre-PST to post-PST for each participant. All participants were able to set measurable goals with guidance from the interventionist, and 81% of the participants (n = 11) who set at least one goal during the hospital stay achieved at least one goal.

Individual participant change in depressive symptoms and self-efficacy.
Feasibility of Electronic Booster Follow-Up
Five participants (54%) used electronic boosters at least once. Overall, the participants who used boosters were satisfied with them (85%; TUQ–Satisfaction, M = 6.0, SD = 1.4; range = 1 [disagree] to 7 [agree]), although they found boosters to be only moderately useful (67%; TUQ–Useful, M = 4.9, SD = 2.9). Most participants found it easy to use (85%; TUQ–Ease of Use, M = 6.3, SD = 1.2), were satisfied with the level of interaction with the interventionist (85%; TUQ– Interaction with Therapist, M = 6.6, SD = 1.6), and were satisfied with the interface quality (85%; TUQ– Interface Quality, M = 6.3, SD = 1.5).
Discussion
The high consent rate, successful completion of PST sessions, high participant satisfaction, and positive change in clinical outcomes (depression and self- efficacy) in this study support the feasibility of PST during inpatient rehabilitation for stroke. We also identified several areas for improvement for future study and clinical implementation. Because this was a feasibility study (Phase IIb; Czajkowski et al., 2015), it was not designed to test the efficacy of PST. Improvement in depression and self-efficacy in this study could be attributed to the passage of time, and participants may have adjusted to their new situation and felt more confident in their ability to function over time. Our findings provide the evidence needed to justify and support conducting a Phase III study to determine the efficacy of PST during inpatient rehabilitation for patients with stroke.
Participant Eligibility
The most common reason for ineligibility was lack of fluency in English. Most of the patients who were excluded spoke Spanish, reflecting the growing number of Spanish speakers who live in and receive rehabilitation services in the United States. To prevent ongoing health disparities that the lack of Spanish-language services may create, we have translated PST into Latin American Spanish (Vega et al., 2020), with pilot testing and cultural adaptation underway.
Feasibility of Participant Retention
We aimed to enroll 15 participants with a goal of each completing at least three PST sessions before IRU discharge. Although PST is generally provided in six sessions, previous studies with other populations demonstrated efficacy after only three sessions and also demonstrated that neither the number of hours devoted to PST nor the length of follow-up was associated with treatment effect sizes, suggesting that the core principles of PST may be rapidly incorporated into daily life and that the effects are maintained over time (Elliott & Berry, 2009; Juengst, Osborne, et al., 2019). Most of the patients we approached consented to participate (88%), and most completed three or more PST sessions during their IRU stay. The main reason for withdrawal from the study was feeling overwhelmed or too tired to participate after a day of therapy. Although patients generally reported high satisfaction with PST, it may be beneficial in the future to include their care partners in a dyadic PST intervention, leveraging the previously documented benefits of collaborative problem solving (Portillo et al., 2009). Patients may feel more supported in the problem-solving process if a care partner is also participating. We previously assessed the feasibility of PST in care partners during the patient’s IRU stay, with promising results (Juengst, Osborne, et al., 2019).
Participants who withdrew were younger, more often female, and reported less independence with ADLs before the stroke than those who completed the study. Notably, all who withdrew had a right-sided hemorrhagic stroke and were all of the participants with hemorrhagic stroke who had been recruited. Although the sample is small, this suggests that those with poorer awareness of their deficits—which is most common in the early stages of recovery after a right-sided stroke (Jehkonen et al., 2006)—may not see the potential benefit of this type of intervention.
Feasibility of the Problem-Solving Training Intervention on an Inpatient Rehabilitation Unit
A short length of stay was the primary reason why patients received fewer than six sessions. This could be mitigated in the future if the PST sessions are continued throughout the transition from hospital to home by means of phone or video calls. Previous work in this area supports the efficacy and feasibility of a phone-based PST intervention for patients with acquired brain injury (Bell et al., 2011).
The DPAT was used as part of the PST intervention to identify and assess potential problems. We found that it provided a structured and comprehensive format for patients to consider and evaluate the problems they anticipated upon returning home. Patients set goals to address the following areas: driving, grooming, transferring to and from the shower, passing through narrow doorways, carrying items while using a walker, and sit-to-stand transfers.
Feasibility of Problem-Solving Training Mobile Boosters
The mHealth booster sessions, which were designed to encourage participants to continue setting goals and implementing PST steps after discharge, were less well received. Only half of the participants tried the booster at least once. Those who used it were mostly satisfied but found it only moderately useful. We trained participants to use boosters during their last in-person PST session. Introducing boosters earlier may reduce confusion and encourage participants to establish a routine. Reminders may also increase compliance. Past studies using similar mHealth platforms trained participants for 2 to 4 wk and closely monitored compliance, assisting with any issues that arose during the training (Nussbaum et al., 2019; Powell et al., 2016). Implementing these changes may encourage more consistent use of boosters throughout the transition from hospital to home and may provide more one-on-one support for booster use. Patients with stroke may also face unique challenges in using mHealth, and although developments in wireless technology have addressed some key factors (e.g., enlarged text, screen brightness, voice dialing), patients with stroke report having difficulty using small screen displays and buttons, as well as confusion because of unclear symbols and complex features (Morris et al., 2010). Developing more user-friendly boosters may also increase compliance.
Study Limitations
Although our results support the feasibility of PST during the IRU stay for patients with stroke, this was a pilot study in a single setting; therefore, the findings cannot be applied across all settings. We could greatly expand our recruitment pool and extend the application of our results by including Spanish speakers, using a validated translation of PST. Twenty percent of the participants withdrew from the study (we withdrew 1 participant). Those patients tended to have greater functional impairment before the stroke and felt overwhelmed by the intervention after a long day. A dyadic intervention that includes the patient and their care partner could provide additional support for the patient during the intervention in the future. Although mHealth boosters were well received by those who used them, compliance was low. We identified several strategies to combat this issue in future studies, including earlier training and supervised implementation. More research into how to best leverage smartphones to support patients throughout the transition from hospital to home is warranted. Last, volunteer bias may have positively skewed the results, because those who are more motivated to participate may also be more motivated to complete proactive problem-solving tasks.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: ▪ PST during inpatient rehabilitation is feasible. The results of this feasibility study suggest that patients with stroke may have the ability to identify problems, set goals, and develop plans to accomplish goals while on the inpatient rehabilitation unit. ▪ In this feasibility study, patients with stroke who used mHealth to maintain problem-solving skills after discharge from the hospital were satisfied with their mHealth experience but found it only moderately helpful.
Conclusions
PST during inpatient rehabilitation for patients with stroke is feasible and positively affects clinical outcomes, although several barriers to PST participation and adherence to mHealth boosters should be addressed in future studies. Strategies to overcome these barriers include translating and adapting PST into other languages, specifically Spanish, and extending sessions over the transition from hospital to home to address short lengths of stay. Including a care partner in PST may offer additional support, and early training and implementation of boosters may increase compliance. Future studies should focus on the timing and efficacy of PST, booster implementation, and the feasibility and efficacy of including both the patient and their care partner in PST.
Footnotes
Acknowledgments
This work was funded by the American Occupational Therapy Foundation.