
Abstract
This study demonstrates that a three-dimensional printed dynamic upper extremity orthosis, which was designed and fabricated by an interdisciplinary team, can, in combination with occupational therapy intervention, facilitate upper extremity function in children with severe hand impairment.
Children with cerebral palsy (CP) commonly present with upper extremity (UE) impairment affecting one or both extremities (Arner et al., 2008; Klevberg et al., 2017) and are classified using the Manual Ability Classification System (MACS; Eliasson et al., 2006). The MACS defines bimanual hand abilities for children ages 4 to 18 yr in everyday tasks and is a gradient scale, with Level I indicating that the child “handles objects easily and successfully” and Level V denoting that the child “requires total assistance” (Eliasson et al., 2006). Children with unilateral UE involvement, who are categorized as being at MACS Levels I to III, are typically able to participate more fully in activities of daily living compared with those with bilateral UE involvement who are functioning at MACS Levels IV to V (Jackman et al., 2022; Klevberg et al., 2017). However, a subset of children with unilateral UE involvement are classified as being at MACS Levels IV and V (Chounti et al., 2013; Eliasson et al., 2006). A recent literature review found that 8.8% of all participants with hemiplegia were at MACS Levels IV or V (Shierk et al., 2016). This small group presents with more severe unilateral UE impairments for which the true prevalence is unknown.
Children with more severe UE impairment are often underrepresented in UE intervention studies. Validated and reliable assessment tools and therapeutic interventions are limited, and the majority of therapeutic interventions are established for MACS Level II, followed by Levels I and III (Shierk et al., 2016). UE treatments with strong evidence, such as constraint-induced movement therapy, bimanual training, context-focused therapy, goal-directed functional training, occupational therapy after Botox injection, orthoses and taping, exercise and strengthening, and home programs, have been studied in children with higher capability, such as MACS Levels I to III (Figueiredo et al., 2020; Friel et al., 2021; Sakzewski, Gordon, & Eliasson, 2014; Sakzewski, Ziviani, & Boyd, 2014; Shierk et al., 2016). In contrast, examinations of interventions for children at MACS Levels IV and V have been limited to goal-directed functional training, occupational therapy after Botox injection, and exercise and strengthening, with significantly fewer participants enrolled in these studies (Shierk et al., 2016).
The present study focused on the novel design and fabrication of an orthosis for the population of children with severe unilateral UE impairment. The terms orthosis, splint, and brace have often been used interchangeably in UE rehabilitation. Recently, the consistent use of the term orthosis has been suggested to standardize terminology in the field (Coverdale, 2012). In 2002, Fess defined an orthosis as a removable device designed for the support of weak or ineffective joints or muscles. The orthoses used in the rehabilitation for children with CP are variable in terms of their types, purposes, and fabrication methods (Lannin & Ada, 2011). For children at MACS Levels IV and V, orthoses are typically static and nonfunctional, with the purpose of preventing the progression of contractures, whereas functional orthoses are used with children with higher fine motor and manual abilities (Jackman et al., 2014). These static, functional UE orthoses, such as wrist cock-up and thumb spica orthoses, when combined with therapy, have been observed to have a positive immediate effect on UE functioning in children with CP; however, the research evidence is limited (Elliott et al., 2011; Jackman et al., 2014, 2018). Far less evidence exists for nonfunctional orthoses (e.g., resting hand orthoses), and they are often not provided in combination with other goal-directed interventions (Imms et al., 2016). Heterogeneity in study methodology inhibits clear clinical recommendations for any orthosis use.
Limitations exist with traditional UE orthosis fabrication and wear because of issues with accessibility, cost, comfort, cosmesis, and carryover (Jackman et al., 2014, 2018). New technology in rehabilitation has evolved into using three-dimensional (3D) printing to fabricate orthotics, prosthetics, assistive devices, and adaptive equipment (Vujaklija & Farina, 2018). The advantages of 3D printing include low cost, ease of customization and fabrication, and increased patient accessibility. Although several promising functional dynamic electric- and non–electric-powered UE exoskeleton devices have emerged in practice to treat pediatric CP and stroke (Ates et al., 2013; Aubin et al., 2013; Butzer et al., 2019), these devices can be heavy and bulky, lack customization, and are restricted to clinic-based use.
The two purposes of this pilot study of children with unilateral CP, functioning at MACS Levels III to V, were to (1) design and fabricate a customized low-cost, functional, dynamic UE orthoses using 3D printing and (2) examine, using a comprehensive evaluation, the effect of the orthosis on children’s UE functioning.
Method
Pediatric patients attending a hospital-based outpatient occupational therapy clinic were enrolled if they met the following five inclusion criteria: (1) CP with unilateral UE involvement, (2) age 4 to 17 yr, (3) functioning at MACS Levels III to V, (4) active elbow arc of motion of at least 50°, and (5) ability to follow one-step directions. The four exclusion criteria were (1) functioning at MACS Levels I and II, (2) Botox injection or orthopedic surgery within the past 6 mo, (3) elbow flexion contracture >30°, and (4) limitations in full passive digit extension. Informed consent and assent were obtained. The New York University School of Medicine institutional review board approved this study (No. 16-02093), and it is registered at ClinicalTrials.gov (NCT03122171).
Three experienced pediatric occupational therapists carried out the intervention. One occupational therapist was assigned to a given participant and was responsible for all aspects of the study for that child, including pretreatment and posttreatment evaluation, orthosis measurement and fitting, fabrication of forearm thumb opponens orthosis, and provision of treatment. No orthoses were worn during evaluations. In 2001, the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) suggested that a comprehensive evaluation should include three major domains: (1) body functions and structures, (2) activity, and (3) participation. In this study, standardized assessments targeting these domains were used; they included the Melbourne Assessment 2 (MA–2; Randall et al., 2001, Assisting Hand Assessment (AHA; Krumlinde-Sundholm & Eliasson, 2003), Pediatric Motor Activity Log–Revised (PMAL–R; Taub et al., 2012), and the Pediatric Quality of Life Inventory: CP Module (PedsQL:CP; Varni et al., 2006).
A multidisciplinary team, consisting of a pediatric orthopedist, pediatric occupational therapists, a pediatric physiatrist, and a design team composed of a professor and undergraduate and graduate students, designed and fabricated the dynamic upper extremity orthosis (DUEO) using the Airy Arm 1.0 (Pediatric Epilepsy Surgery Alliance, 2014) open-source design as a starting point. An occupational therapist measured the length and circumference of each participant’s upper arm, forearm, and hand, including only the index, middle, and ring fingers (Figure 1A-D). The design team used these measurements in conjunction with a 3D scan of the individual’s forearm and hand to create a digital model that was used to print the DUEO.
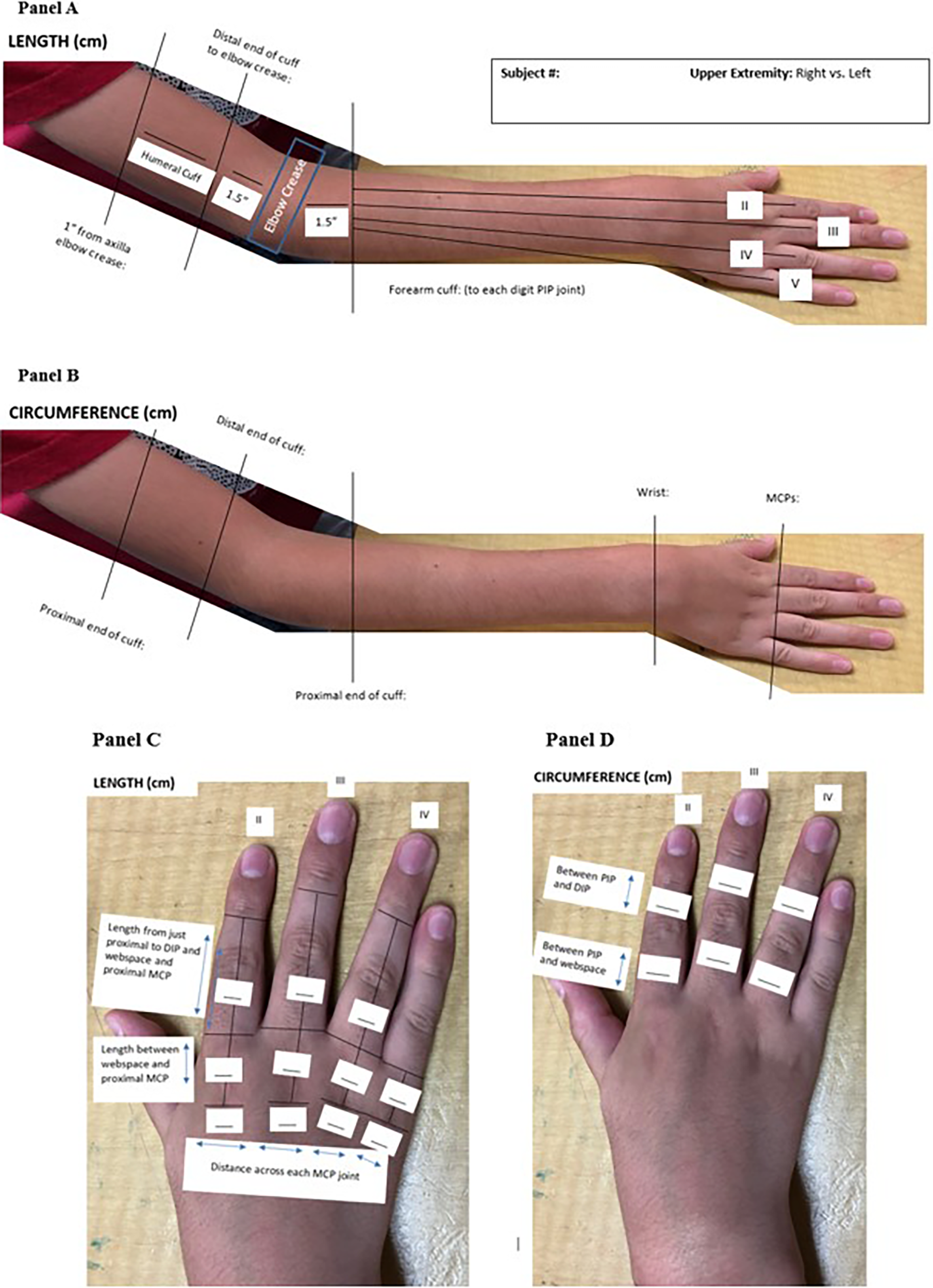
Photographs of the instructions for measurements required for DUEO fabrication. Panel A: Upper extremity length measurements. Panel B: Upper extremity circumference measurements. Panel C: Digit length measurements. Panel D: Digit circumference measurements.
Customized Fabrication of the Dynamic Upper Extremity Orthosis
The three main 3D-printed components of the DUEO included the upper arm, the forearm, and the fingers (Figure 2, Panel A). The upper arm cuff, which encircled approximately 75% of the arm, 1.5 in. above the elbow crease, was fabricated out of polylactic acid (PLA) and secured via a hook-and-loop fastener. The dorsal forearm component extended from 1.5 in. distal from the elbow crease to the distal end of the metacarpal phalangeal joint (MCP) and was secured via a hook-and-loop fastener. The dorsal forearm component, also printed using PLA, included guides that allowed the cables to be centrally threaded to attach distally to the finger components. The hinge between the upper arm and forearm components was composed of a clear vinyl tube with a bungee cord inside to prevent the tube from collapsing during motion. The dorsal flexible finger components, fabricated from polyurethane (TPU), had circumferential strapping over the proximal and middle phalanges. It is important to note that the fingertips were left exposed to allow tactile input when contacting objects. All three components were connected by three continuous fishing line cables, which attached to a tensioner at the proximal end of the upper arm cuff, spanned the length of the DUEO, and attached to the distal end of the finger components.
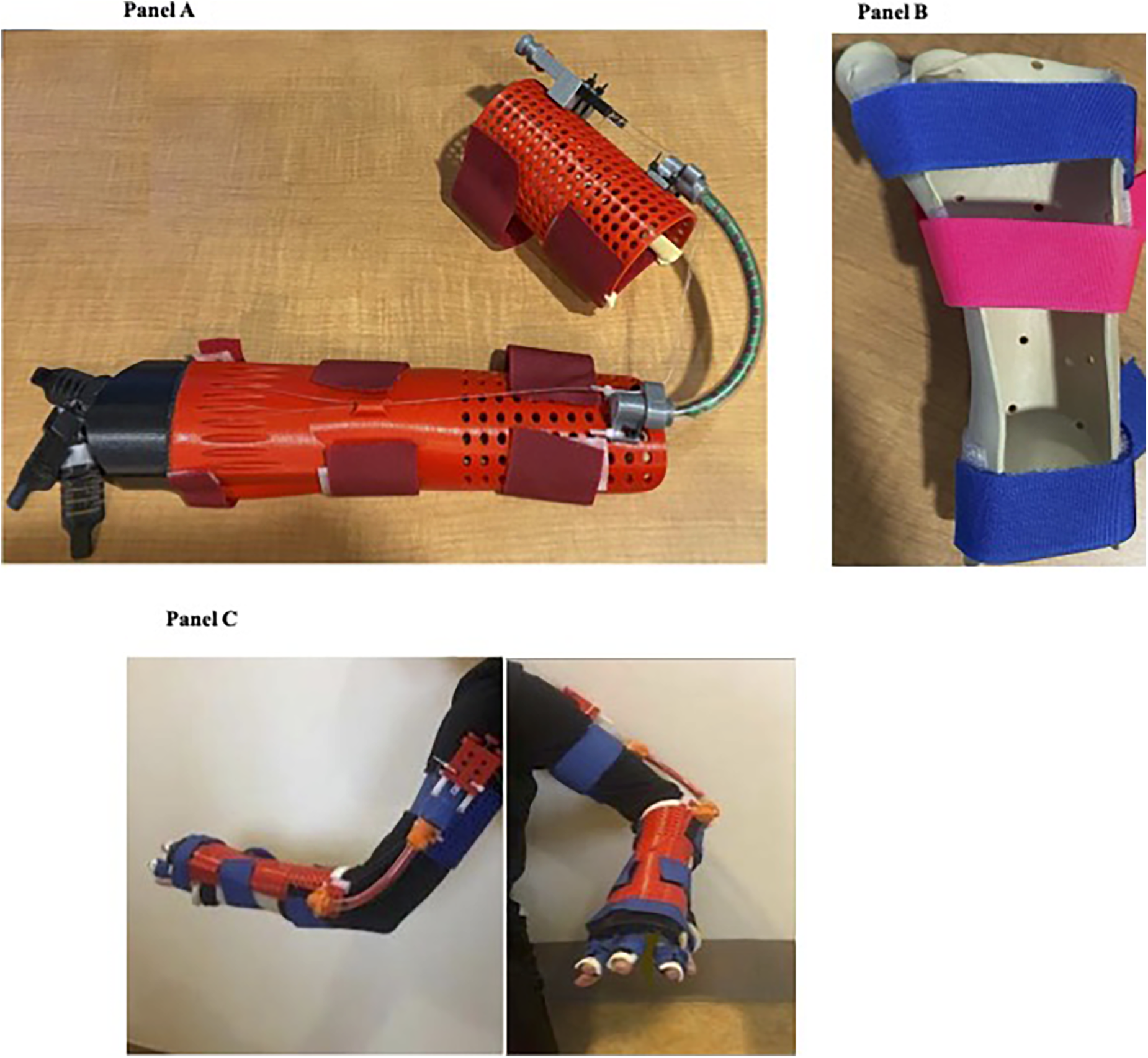
Photographs of devices before and after donning. Panel A: Assembled DUEO. Panel B: Custom forearm thumb opponens orthosis. Panel C: A participant wearing DUEO and thumb opponens orthosis.
An occupational therapist fabricated a separate static, custom forearm thumb opponens orthosis from thermoplastic material (Figure 2, Panel B). This custom orthosis maintained thumb opposition and placed the wrist in a degree of extension that still allowed for full passive digit extension for each participant. The forearm thumb opponens orthosis was donned first, under the DUEO. Panel C of Figure 2 shows a participant wearing the DUEO with the forearm thumb opponens orthosis.
At a minimum of two fitting sessions, the occupational therapist determined the appropriate alignment and positioning of the components on the participant. The occupational therapist then adjusted the tension in the cables so that with active elbow extension the cables became taut and extended the participant’s three fingers at the proximal and distal joints. During active elbow flexion, the cables slackened and allowed the participant’s fingers to actively flex.
Goal-Directed Occupational Therapy With the Dynamic Upper Extremity Orthosis
The functional aim of the DUEO was to allow the child to use their hand and digits to stabilize items in their hand with grasp or against a surface, such as a tabletop, to participate in bimanual activities. Subsequent to the completed fabrication of the DUEO and the custom forearm thumb opponens orthosis, each participant received eight 1-hr clinic-based occupational therapy sessions consisting of goal-directed therapy focusing on the functional use of the DUEO. The DUEO was worn only during therapy sessions and was not taken home. Before participant enrollment, the occupational therapists discussed and reached a consensus on the progression of the therapeutic goals with the actual activities individualized to each participant’s interests. Initially, the DUEO was used in a unimanual capacity to master opening and closing one’s digits through active elbow flexion and extension. This progressed to the actual grasp and release of items from easy positions, such as from the therapist’s hand or a stable surface, to simulate grasp from their dominant hand, a precursor to bimanual skills. Finally, bimanual training was performed, and the affected hand stabilized objects with grasp while the dominant hand performed the necessary manipulation tasks (i.e., opening the lid to paint containers or holding a plastic bag while retrieving a snack). The inclusion of various sizes and shapes of objects allowed for upgrading of the targeted skills. Clinical activities simulated typical tasks the participants encountered in their daily lives, such as crafts, folding laundry, and washing dishes.
Standardized Outcome Measures
Body Functions and Structures as Measured by the Melbourne Assessment 2
The MA–2, a body functions and structures measure, examines unimanual capacity of movement in the involved UE. Raw scores are reported for the following four subscales: range of motion, accuracy, dexterity, and fluency (Randall et al., 2001). An examination of the MA–2’s psychometric and clinometric properties demonstrated high test–retest reliability, concurrent validity was generally moderate, and responsiveness to change was high. The minimal clinically important difference (MCID) has been determined to be a raw score change of >3 for range of motion, accuracy, dexterity, and fluency and a change of >4 for accuracy (Wang et al., 2017).
Bimanual Activity as Measured by the Assisting Hand Assessment
The AHA, an activity-level measure, assesses the ability of children with unilateral UE involvement to use their two hands together spontaneously in bimanual play activities. Twenty items are scored using a 4-point rating scale. A total score is reported in the form of logit-based AHA units, ranging from 0 to 100 (Holmefur & Krumlinde-Sundholm, 2016). A higher score indicates better bimanual functioning, and a logit-score change of 5 is considered clinically significant (Krumlinde-Sundholm, 2012). Strong internal scale validity, interrater and intrarater reliability, and responsiveness to change have been reported for its use with children with unilateral CP (Holmefur & Krumlinde-Sundholm, 2016).
Overall Activity as Measured by the Pediatric Motor Activity Log–Revised
The PMAL–R, an activity-level measure, is a structured interview in which the caregiver reports “How Often” (amount) and “How Well” (quality of movement) the child uses their involved UE when completing activities carried out in daily life (Taub et al., 2012; Uswatte et al., 2012). A mean score is determined for each of the two scales (Taub et al., 2012). For each rating scale average, the MCID is a change of 0.42 (Lin et al., 2012). Internal consistency and test–retest reliability are good to high when used with children with hemiplegic CP (Uswatte et al., 2012).
Participation as Measured by the Pediatric Quality of Life Inventory: CP Module
The PedsQL:CP, a participation-level measure that focuses on quality of life, is a semistructured interview in which a caregiver and/or the child reports difficulty on seven scales: Daily Activities, School Activities, Movement and Balance, Pain and Hurt, Fatigue, Eating Activities, and Speech and Communication. Higher scores indicate a better quality of life (Varni et al., 2006). This instrument has good construct validity and has been established in many languages and contexts (Varni et al., 2006), but no MCID has been reported for it.
Data Analysis
Descriptive statistics were used to calculate change scores for each assessment from pretreatment to posttreatment for each participant. The frequencies of positive changes in scores and change scores that met MCID levels were determined.
Results
The participants were four boys and one girl, ages 13 to 17 yr. All had unilateral UE involvement, three with right and two with left. MACS levels were III for one participant and IV for the other four. The active elbow arc of motion ranged from 54° to 150° (Table 1).
Participant Demographic Characteristics
Note. L = left; MACS = Manual Ability Classification System; R = right; UE = upper extremity.
The DUEO was modified in small ways to meet each participant’s needs as various means of assembly and design were trialed, an advantage of the modular design. Modifications included adding foam to the underside of the distal end of the forearm piece to block MCP hyperextension and, for finger pieces, changing material from PLA to TPU and constructing it from solid to multislitted to increase flexibility for ease of finger movement. Adjustments during therapy sessions, such as retensioning the cables or repositioning the finger components, were occasionally required.
Standardized Outcome Measures
Body Functions and Structures as Measured by the Melbourne Assessment 2
Higher posttreatment than pretreatment raw scores were found for four participants for range of motion, three for accuracy, three for dexterity, and two for fluency. The criteria for MCID were met for three participants for accuracy, one for dexterity, and one for fluency. However, for Participant 4, the change for dexterity indicated a decrease (Table 2).
Change in Pretreatment to Posttreatment Scores by Participant
Note. AHA = Assisting Hand Assessment; Comm. = Communication; MA–2 = Melbourne Assessment 2; PedsQL:CP = Pediatric Quality of Life Inventory, Cerebral Palsy Module; PMAL–R = Pediatric Motor Activity Log–Revised; ROM = range of motion.
Met minimal clinically important difference criteria.
Bimanual Activity as Measured by the Assisting Hand Assessment
Participants 1 through 4 showed a clinically significant improvement in their logit scores, ranging from 8 to 20, from pretreatment to posttreatment (Table 2). Table 3 shows the number of participants who demonstrated improvement for each item of the AHA. The most frequent improvements were found in stabilizes by weight or support and stabilizes by grasp for four of the five participants, and amount of use, orients objects, releases, and grasps for three of the five participants.
Frequency of Participants Who Showed Improvement in Each of the Skill Areas of the Assisting Hand Assessment
Note. AH = assisting hand.
Overall Activity as Measured by the Pediatric Motor Activity Log–Revised
Four participants (1–3 and 5) showed increases in both the amount and the quality of movement for the involved UE, whereas Participant 4 showed no change in either. Participant 2 met the MCID criteria for both the amount and quality of movement (Table 2).
Participation as Measured by the Pediatric Quality of Life Inventory
Parents of Participants 1–4 answered the PedsQL:CP, and Participant 5 self-reported. Three parents reported improvements in Daily Activities, School Activities, and Movement and Balance; two reported improvements in Pain and Hurt; and one reported improvement in Fatigue, Eating Activities, and Speech and Communication (Table 2).
Discussion
This pilot study showed that the DUEO, a 3D-printed orthosis, in conjunction with goal-directed therapy, was associated with positive changes in a sample of children with CP who had moderate to severe unilateral hand impairment. Improvements were seen in body functions and structures as well as activity domains of the ICF in relation to the MA–2 and the AHA. Mixed results were found for participation, as measured by the PedsQL:CP and, despite gains in overall activity, as measured by the PMAL–R, these results were not clinically significant. Along with the novel design and fabrication methods of the DUEO, the following key factors contributed to these outcomes: the collaboration among members of the multidisciplinary team in its design and fabrication; the use of comprehensive outcome measures applicable to this population; and the occupational therapy intervention of goal-directed, bimanual training.
The use of 3D printing in rehabilitation and prosthetics has become increasingly popular because of advancements in computer design software, the low cost of materials, and the potential for custom fabrication (Vujaklija & Farina, 2018). Three-dimensional printed material has come to replace traditional thermoplastic or metal, with a clinician or nonclinician designing and fabricating the device using new technology (Mohammadi et al., 2018; Patterson et al., 2020). Despite the increasing number of occupational therapists using 3D printing to create basic adaptive equipment, most are limited because of the advanced design and technical skills needed to fabricate more intricate objects, such as custom orthoses. Our study design team’s ability to 3D scan, design, and print the components, combined with the physician’s and occupational therapist’s clinical knowledge of diagnosis, anatomy, and biomechanics, produced a dynamic device, the DUEO, which showed potential to enhance the function of the involved arm (Barbareschi et al., 2017).
The selected assessments provided a comprehensive evaluation based on the ICF body functions and structures, activity, and participation domains (Gerber et al., 2016). The MA–2 assessed the capacity of the affected extremity, whereas the AHA examined how the child typically used their affected extremity during bimanual functioning. These two outcome measures were sensitive enough to detect individual changes for this patient population, particularly for skills that were directly facilitated by the DUEO. For example, the DUEO facilitated reaching with digit extension, resulting in improvements in accuracy to target (MA–2) as well as overall amount of use, grasp, and release (AHA) of the involved arm.
Because patient- and parent-reported outcome measures have recently been identified as important components of the assessment of function in children with CP (Sköld et al., 2011), the commonly used PMAL–R and PedsQL:CP were included to complete the battery of outcome measures. Clinically significant improvements were not noted for the PMAL–R. This may be due to participants continuing to use only their dominant hand for activities, because most activities included in this assessment can be performed unimanually. Caregivers reported improvements on the PedsQL:CP in only a few categories for multiple patients: Daily Activities, School Activities, and Movement and Balance. However, with a measure this broad, it may be difficult to detect changes associated with a treatment directly focused on improving hand use. Additional sessions with the DUEO, whether in the clinic or as part of a home program, may have improved outcomes and should be explored in future research.
Despite this lack of positive findings on these standardized patient- and caregiver-reported outcome measures, caregivers anecdotally reported increased spontaneous use of the involved arm between sessions. A different quality-of-life measure under the participation domain emphasizing bimanual hand use may be a more suitable outcome measure. Therefore, future research should consider the inclusion of the Children’s Hand-use Experience Questionnaire (CHEQ; Sköld et al., 2011), a valid and reliable tool that measures both activity and participation, as a more appropriate patient- or caregiver-reported outcome. The CHEQ assesses more specific tasks typically performed bimanually and how the child feels about their ability compared with others (Sköld et al., 2011).
Finally, bimanual, goal-directed therapy used with the current participants has evidence to support its effectiveness in improving the functional abilities of children with CP (Jackman et al., 2022; Sakzewski, Gordon, & Eliasson, 2014; Sakzewski, Ziviani, & Boyd, 2014; Shierk et al., 2016), with structured skill training further increasing the benefit (Friel et al., 2016). When goal-directed therapy was combined with wearing the DUEO, an improved ability to stabilize and grasp objects in the involved extremity was observed. Similarly, improvements were noted when a functional orthosis was combined with therapy for children with CP (Elliott et al., 2011) and other diagnoses (Ragni et al., 2022). Overall, however, a recent systematic review found insufficient conclusive evidence to support UE improvement associated with the combination of a functional orthosis and therapy (Garbellini et al., 2018).
A limitation to this study is the small sample size and the concomitant inability to perform inferential statistical analysis to make definitive conclusions on the basis of the findings. Another limitation is that having the same clinician provide the treatment and perform both pretreatment and posttreatment assessments might have biased the results. In addition, no assessment was done immediately after a participant donned the orthosis to evaluate the effect of the orthosis alone.
A third limitation is the lack of application of a more appropriate outcome measure (e.g., the CHEQ) to address the ICF participation domain, as part of a comprehensive evaluation, for this population. Future, larger studies should incorporate a comparison group involving only therapeutic intervention without the orthoses, to clarify the role of the DUEO in any changes found in participants’ manual abilities.
The low cost and potential easy access to the fabrication process makes the DUEO a possible alternative to currently available devices. The estimated cost of the 3D portion of the DUEO is less than $50 versus $1,200 for a custom thermoplastic dynamic elbow orthosis, both of which have the added cost of the custom forearm thumb opponens orthosis. If custom forearm thumb opponens fabrication is not possible, then a prefabricated one could be considered.
This pilot study was conducted at a large university that had both a pediatric occupational therapy department with customizable splinting materials and a design team at their engineering school with 3D printers. Neither of these may be available at smaller institutions and hospitals or therapeutic private practices. Therefore, if further research supports the more widespread use of the DUEO, then a facility will need to establish an individualized program within its community or with a larger institution for the fabrication of the 3D-printed orthosis.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ A multidisciplinary team, including occupational therapists, was beneficial for the design and fabrication of the custom 3D-printed DUEO. ▪ Children with unilateral UE involvement, functioning at MACS Levels III and IV, may benefit from the DUEO with an increase in involved UE function if subsequent, larger studies show similar results. ▪ Goal-directed, task-specific training in combination with the DUEO increases use of the involved UE in therapy sessions. ▪ Using both clinician-based and patient-reported outcome measures from all ICF domains provides a more global view of hand function and participation.
Conclusion
For this pilot study, a multidisciplinary team, including a pediatric orthopedist, pediatric occupational therapists, a pediatric physiatrist, and a design team, designed a low-cost, functional, dynamic 3D-printed UE orthosis, the DUEO. When paired with goal-directed occupational therapy, a small group of pediatric patients with CP with unilateral UE involvement, functioning at MACS Levels III and IV, showed gains in UE function.