
Abstract
Occupational therapists can provide assessment using the Integrative Medication Self-Management Intervention (IMedS) to positively influence medication adherence in a primary care setting.
Improved control of hypertension (HTN) and Type 2 diabetes mellitus (T2DM) has been recognized as a priority by the World Health Organization (WHO) because of the associated concomitant mortality and morbidity and subsequent rising health care costs (WHO, 2013, 2018a, 2018b). Taking medications as prescribed is key to successful health management for both conditions, but half of the people with these conditions do not take their medications as prescribed (Bailey & Kodack, 2011; Stewart et al., 2014; Will et al., 2016). Poor medication adherence results in uncontrolled disease progression and subsequent poor health outcomes and hospitalizations (Jiang et al., 2016; Stewart et al., 2014; Will et al., 2016). This results in further physical, financial, and social costs (Schroeder et al., 2004; WHO, 2013, 2018a).
Although the factors that influence adherence are well documented, no clear means for improving adherence has been identified (Geboers et al., 2015; Nieuwlaat et al., 2014). Research has shown that client-centered interventions that allow for individualized problem solving have the potential to affect adherence positively (Nieuwlaat et al., 2014; Schroeder et al., 2004). The Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020) and emerging research suggest that occupational therapists can play a role in addressing medication management and adherence (Schwartz & Smith, 2016). According to the OTPF–4, health management is “occupation focused on developing, managing, and maintaining routines for health and wellness by engaging in self-care with the goal of improving or maintaining health” (AOTA, 2020, p. 77). The Integrative Medication Self-Management Intervention (IMedS) is an occupational therapy intervention designed to improve client adherence to medications with a focus on the effective use of therapeutic communication (e.g., motivational interviewing and therapeutic use of self) and health literacy. In a randomized Phase 1 feasibility study completed in a lab environment, the IMedS was shown to influence medication adherence (Schwartz & Smith, 2016), and a qualitative analysis showed that the IMedS facilitated new medication habits and routines (Schwartz et al., 2017). The objective of this study was to evaluate the effectiveness of the IMedS in a primary clinic on adults with HTN, T2DM, or both.
Method
Study Design
This randomized controlled trial using a pretest–posttest control group design took place at a large federally qualified health center (FQHC) in Missouri. The University of Indianapolis institutional review board approved all study procedures.
Participant Selection
An a priori sample size estimation indicated the need for 32 participants to detect a moderate effect size of .30. To be included in the study, participants were required to be adults with uncontrolled HTN, T2DM, or both seeking treatment from the clinical pharmacist at an FQHC. Clients were excluded if they had a medical power of attorney or were unable to provide their own informed consent.
Instruments
Medication adherence was the primary outcome for this study. The seven-item version of the Adherence to Refills and Medication Scale (ARMS–7) is a reliable and valid self-report questionnaire of medication adherence with a 4-point response scale (Kripalani et al., 2015). The scale ranges from 1 to 4 per item, but 6/7 items are scored as 1 = all of the time, and on the last question 1 = none of the time, to help correct for agreement bias. Scores on the ARMS–7 range from 7 to 28. The instrument was designed to be flexible and, in this study, higher values indicated better adherence (Kripalani et al., 2009). Pill count identifies how many pills remain in a person’s bottle as compared with refill timing and the number that should remain (Hawkshead & Krousel-Wood, 2007).
We also investigated the control of the chronic conditions via blood pressure and hemoglobin A1c (HbA1c) values. We measured blood pressure using the manual auscultatory method. Readings were converted into mean arterial pressure (MAP). For people with hypertension, lower MAP scores are better. For diabetes, HbA1c values were retrieved from participants’ medical charts.
Participants’ demographics were also collected (Table 1). Comorbidities were weighted by means of the validated Charlson Age–Comorbidity Index (CACI). The CACI score was used to weigh the impact of participants’ comorbidities on their performance (Charlson et al., 1994).
Demographic Characteristics of Study Participants at Baseline (N = 29)
Note. There were no significant differences between groups at the p < .05 level. IMedS = Integrative Medication Self-Management Intervention; TAU = treatment as usual.
Procedures
Recruitment and Consent
Participants were recruited from the clinical pharmacy caseload at an FQHC. Participants were then invited to review and sign the informed consent form. Then, the clinical pharmacist requested an occupational therapy order from the participant’s referring provider.
Randomization
Participants were consecutively and randomly assigned to either the group receiving treatment as usual (TAU) or the group receiving TAU plus occupational therapy and the IMedS intervention—hereinafter referred to as the IMedS group. Group assignment was performed using sequentially numbered, identical, opaque, sealed white envelopes.
Data Collection and Intervention
First, the interventionist collected baseline measures (ARMS–7, pill count, and blood pressure) of all outcomes; then the clinical pharmacist, pharmacist intern, or occupational therapy researcher (Helen Bourke-Taylor) administered the interventions. The occupational therapy researcher completed competency training with the IMedS author (Jaclyn K. Schwartz) before initiating the study. Occupational therapy services were free to participants, and no compensation was provided to encourage participation.
Treatment-as-Usual Intervention
Participants met individually in person with the clinical pharmacist to learn about the diagnosis, diet, exercise, lifestyle factors, and medication adherence. Participants were also asked to set a health management goal, and the pharmacist adjusted medications as needed. The number of visits varied and was based on participant need and participation (Table 1). At each visit, the pharmacist delivered the intervention and administered the outcome assessments of pill count, ARMS–7, and blood pressure reading.
IMedS Intervention
Participants met individually in person with the occupational therapist to discuss their medications as well as their habits, roles, and routines. To help guide the intervention, the medication management subtask of the Performance Assessment of Self-Care Skills was performed (Rogers & Holm, 1989). To enhance medication adherence, the therapist delivered information in a manner consistent with the participant’s health literacy and used a motivational interviewing–based guided approach. Motivational interviewing, compared with traditional advice giving, has been found to be associated with better outcomes (Miller & Rollnick, 2012). Participants were then asked to develop new strategies around their personal routine while considering environmental supports and constraints. The full IMedS manual is available for review at Schwartz (n.d.). The number of visits was determined by the occupational therapist’s plan of care and a person’s level of participation (Table 1). At each visit, the occupational therapist delivered the intervention and administered the outcome assessments.
Data Screening and Analysis
Data were analyzed using IBM SPSS Statistics (Version 24). Because participants had different numbers of visits, outcomes were assessed from the data collected at the initial visit and the final visit. At the group level, change scores were evaluated for outcome measures using Fisher’s exact test for nominal data and either an independent t test or a nonparametric Mann–Whitney U test, depending on whether the normality assumption was met. Change scores were calculated for both groups by subtracting the initial result from the final result. A 2 × 3 mixed analysis of variance (ANOVA) was used to test whether there was a difference in ARMS–7 scores between and within the two groups. Effect sizes for the ARMS–7 results were reported using Dunlap’s correction for intercorrelation of the measurements (Dunlap et al., 1996) instead of Cohen’s d (Cohen, 1988), which may overreport the true effect.
Results
Originally, 32 participants enrolled in the study. Three participants did not return after the initial visit, leaving a total sample size of 29, with 12 participants assigned to TAU and 17 assigned to IMedS (Figure 1). Sample and baseline characteristics of the IMedS and TAU groups are found in Table 1. The IMedS and TAU groups were found to be similar across all demographic characteristics.
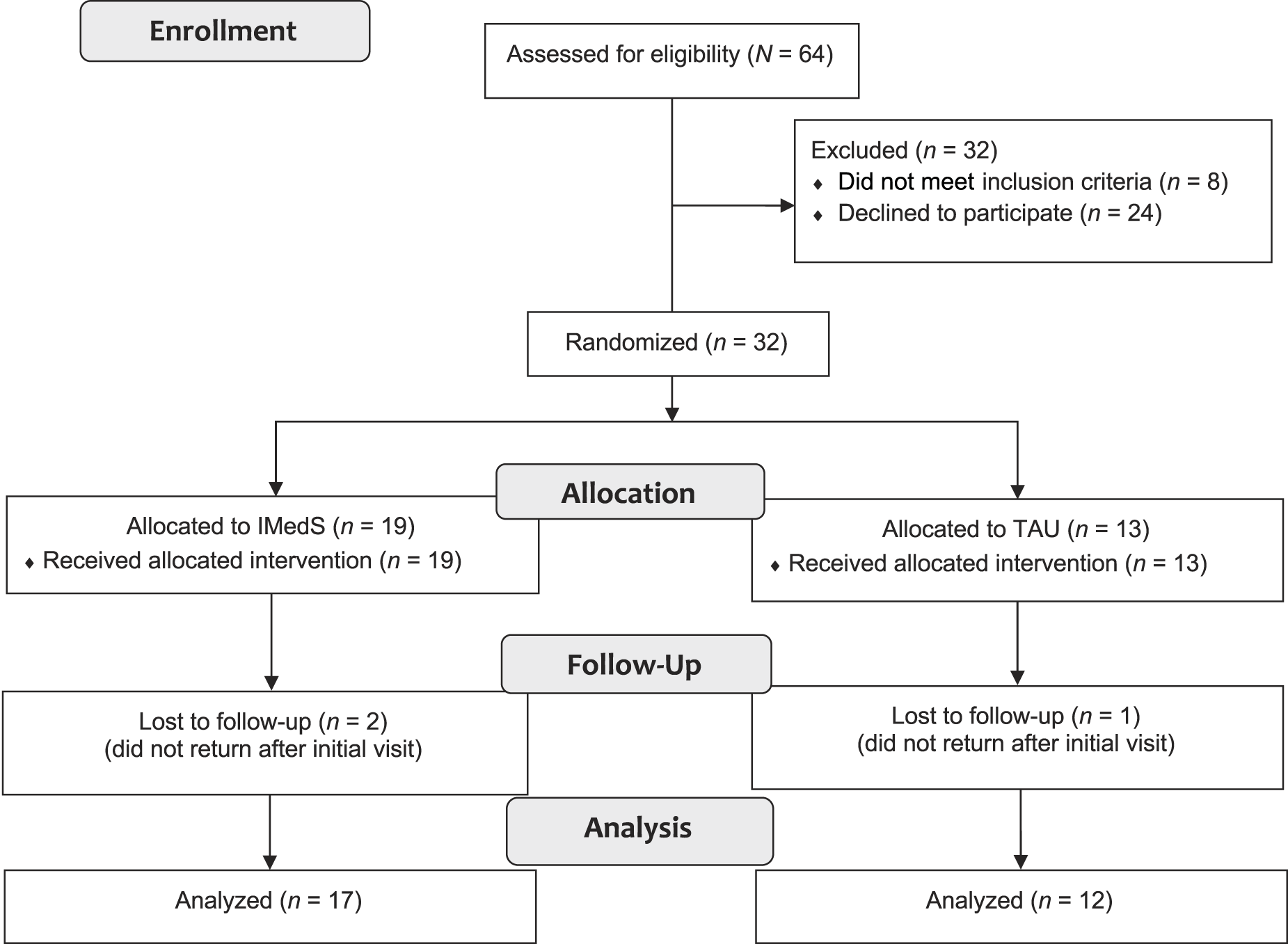
Consolidated Standards of Reporting Trials flow diagram of participants.
Comparisons Between and Within Groups
ARMS–7
The results of the mixed ANOVA indicated that there was not a significant interaction and that there was a weak effect size, F(2, 23) = 2.24, p = .129, η = .16. There was no main effect between groups; however, there was a significant main effect within the three time periods, F(2, 23) = 6.11, p = .007, η = .35, indicating that both groups had significant improvement over time.
The means plot revealed a V shape for the IMedS group that bore further analysis (Figure 2) because of its dissimilarity to the pattern of change in the TAU group. Given the statistically significant main effect for time, post hoc paired t tests using the Bonferroni correction were completed. The only post hoc pairwise test that was significantly different was the comparison between the midpoint and final results for the ARMS–7 measurement, t(14) = 3.41, p = .004, dc = 0.65. The limited power of the test, owing to the relatively small sample size, however, was not sufficient to find this in a comparison of the initial to midpoint results or of the initial to final results. Although both groups were assessed at relatively high adherence by means of the ARMS–7, ultimately, participants in the IMedS group arrived at a self-assessed adherence rate slightly greater than that of the TAU group (Figure 2).
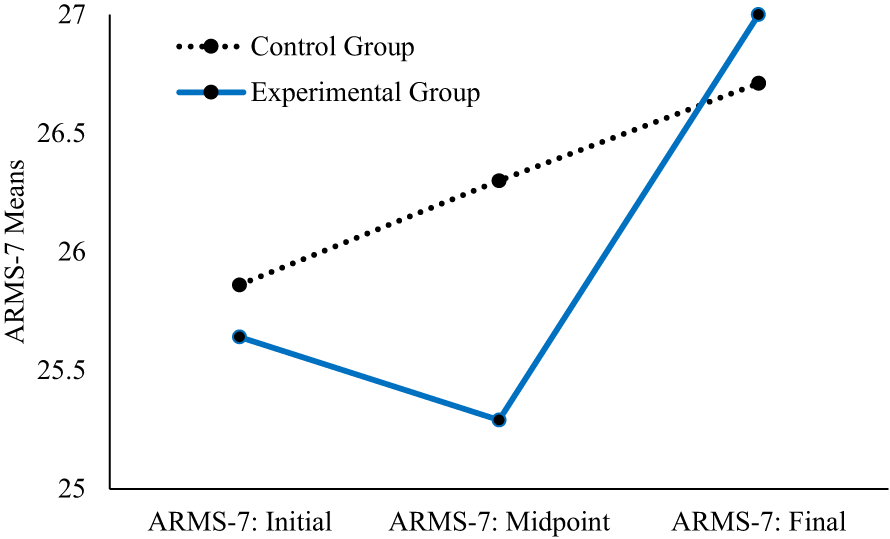
Scores on the ARMS-7 by group over time (N = 29).
Pill Count
The change score between the first and final pill count was calculated and compared between groups. Because of the violation of the normality assumption, we used a Mann–Whitney U test. The change score was not significantly different between the IMedS and TAU groups for pill count, U = 46.00, z = −1.28, p = .215. The median pill count percentages for the change score were noted to demonstrate a sizable difference, with the IMedS group having a median of 20.80 and the TAU group having a median of 1.70. We used an effect size calculator, Measure of the Effect (Version 0.0.0.9100), to examine mean differences on a standardized scale (Buchanan et al., 2017). Our calculation revealed an effect size of .55, indicating a medium effect size for the IMedS intervention on pill count (Cohen, 1988).
Control Chronic Conditions
The impact of the intervention on the control of chronic conditions was also used to measure adherence. To assess the impact on blood pressure, we compared the MAP change scores—calculated using the initial and final results—of the IMedS and TAU groups (IMedS group, Mdn = −4.00; TAU group, Mdn = −8.33). The assumption of normality was violated. Mann–Whitney U test results indicated that there was not a significant difference (U = 60.00, z = −1.17, p = .259). In line with previous analyses, the effect size was small (.31). Through the randomization process, 10 of the 11 participants with a recorded HbA1c were assigned to the IMedS group. Therefore, change was evaluated on the basis of an established clinical threshold of a change of at least 0.5% (5.5 mmol/mol; Lenters-Westra et al., 2014). The majority of participants with T2DM (n = 8; 89%) in the IMedS group demonstrated a clinical improvement in their HbA1c; however, the 1 participant in the TAU group with T2DM did not meet this standard of change.
Discussion
Poor medication adherence is an important health management issue that affects more than half of people with HTN and T2DM. Despite this importance, no clear means to improve adherence in community settings has been identified (Geboers et al., 2015; Nieuwlaat et al., 2014). The purpose of this study was to evaluate the efficacy of the IMedS on community-dwelling adults with HTN, T2DM, or both.
The findings of this study suggest that the proportion of adherent participants increased in both groups but was not significantly different between groups when measured by either self-report or pill count. This finding supports the work of Schwartz and Smith (2016) and indicates that medication adherence can be responsive to occupational therapy intervention. This finding also corroborates previous work by Doggrell (2010) that suggests that there is no clear preference for an intervention from a specific profession.
Although both groups improved, an analysis of individual outcome measures suggests an interesting phenomenon. As demonstrated in Figure 2, medication adherence sharply decreased and then sharply increased for the IMeDS group, whereas the TAU group experienced a gradual increase. We attribute this difference to the fact that the occupational therapy intervention often improved participants’ ability to identify nonadherence, resulting in a drop in self-reported adherence on the ARMS–7. In these cases, participants were also noted to verbalize a heightened understanding and commitment to making changes in their daily habits related to medication adherence. Once the participants identified the need to improve their adherence and implemented self-selected strategies, their adherence rose to just above that of the TAU group.
Standardized mean difference effect sizes, although limited by sample size, provide information for clinical application and may be useful in future research to strengthen power analyses. The pill count outcomes were further evaluated for differences across time and group because of the differences identified in the mean percentage change between the IMedS group and the TAU group. The comparison of the two interventions yielded a medium difference between the two, suggesting that the occupational therapy intervention positively affected adherence as measured by pill count. This difference supports previous IMedS research findings that medication adherence is responsive to occupational therapy (Schwartz & Smith, 2016). These findings also expand on previous research demonstrating that the intervention can be effective in a lab setting by showing that the IMedS approach can be useful in a primary care clinic.
Effect size analysis of the MAP change score indicated that the TAU group saw a larger change for blood pressure than the IMedS group. Because both groups received an intervention by the clinical pharmacist for the adjustment of medications and counseling, the difference may be due to small variations between groups or individual factors that influence blood pressure but were not tracked in the study (e.g., caffeine intake, stress level). Although the differences were not statistically significant, the IMedS group demonstrated an older mean age, was managing more medications, had less assistance at home, and had a higher number of comorbidities. The TAU group also started with a higher mean MAP, which may have made it easier to detect change. We remained cautious because of the number of missing data points for MAP; however, we saw an overall decrease in MAP for both groups, indicating that the interventions had the desired effect in this population.
Although HbA1c could not be compared between groups because of the inequality in the number of participants with T2DM, it is notable that nearly 90% of participants in the IMedS group demonstrated a clinically relevant decrease in their HbA1c. These participants received both the pharmacy and the occupational therapy interventions. Future research should focus on whether the occupational therapy intervention was necessary to produce this change.
The literature supports the IMedS approach as administered by an occupational therapist. In a systematic review of medication adherence interventions, Conn et al. (2015) reported that the interventions showing the most promise were those addressing the link between habits and adherence behaviors, providing adherence feedback, self-monitoring of blood pressure, the use of pill boxes, and motivational interviewing. In the clinical process, the occupational therapist inherently views clients through their individualized daily occupations, habits, and routines, which have also been identified as key components of effective adherence interventions (Längst et al., 2015). The occupational therapist also used the pill count information as objective feedback to increase self-awareness about adherence behaviors. Participants also used combinations of individualized environmental supports such as taking their blood pressure at home; using pill boxes; and establishing environmental cues such as checklists, alarms, and smartphone applications. The occupational therapist’s approach also included assessing and treating cognitive and coordination limitations that affect medication management. Motivational interviewing throughout the intervention appeared to be key for the prolonged use of new strategies, as the individual was coached to identify and personalize areas for improvement and strategies that best fit their unique contexts.
No significant influence of demographics was found once Type 1 error corrections were completed for the demographics of age, gender, ethnicity, assistance at home, number of medications, and number of comorbidities (Table 1). This corroborates a large, randomized controlled trial (Whittle et al., 2016) and a meta-analysis (DiMatteo, 2004), which found that demographic factors had only a small effect on adherence.
Limitations
The randomization of participants created analogous groups for analysis, but potentially confounding factors that influence MAP and HbA1c were not evaluated or controlled. Confounding variables of diet, exercise, health literacy, medication beliefs, and financial constraints may have influenced outcomes in either direction (Náfrádi et al., 2017; Sontakke et al., 2015).
Three outcome measures were used; however, each has its own limitations, and this may have influenced study findings. The findings in this study agree with previous findings that individuals tend to overestimate their level of adherence, with the initial ARMS–7 mean score being 26 out of 28 (Kelly et al., 2016; Nguyen et al., 2014). Pill count data were limited by the participants’ willingness to allow us to count their pills, forgetting to bring their pills, and combining pills from multiple bottles. Although blood pressure provides an objective measurement, it varies throughout the day and can be influenced by extraneous variables such as recent caffeine intake, timing of exercise, stress, a participant’s decision to not take the medicine when in public because of side effects (e.g., increased urination), or the duration of use of antihypertensive medications (Mancia et al., 1983).
Outcomes may also be affected by the amount of time in care. Conn et al. (2015) previously concluded that the most effective adherence measures addressed multiple components and were delivered over several days. Although the IMedS process is intended to address many areas, intervention time was often limited by having to share appointment time between the pharmacist and the occupational therapist, by the participant needing to attend another appointment, or both. Several participants in both groups missed appointments because of a lack of transportation or other individual stressors.
A ceiling effect on the ARMS–7 also affected results: Despite our finding that most participants were not as adherent as they reported, those with truly high adherence had very limited room to improve. These individuals demonstrated little to no change in the outcome variables. Furthermore, it was difficult to determine whether the ARMS–7 was measuring adherence as it was intended or whether it was more accurately measuring the participants’ self-awareness of their adherence. Further studies should be designed to evaluate whether self-report measures are most accurately measuring actual adherence or the level of awareness of adherence.
The total sample size was also a limiting factor that affected generalizability. The recruitment efforts took nearly twice as long as anticipated, and staffing resources prevented an extension of the study. The minimum number of participants were recruited, although with a subsequent attrition of 3 participants.
Implications for Occupational Therapy Practice
These results are consistent with the results from previous research that occupational therapists can offer interventions that can increase medication adherence (Sanders & Van Oss, 2013 ; Schwartz & Smith, 2016). This study also demonstrated that it is feasible for an occupational therapist to provide this intervention in a primary care setting. Behavior change techniques identified by Patton et al. (2018) for improving medication adherence in primary care fit well within the occupational therapist’s scope of practice (e.g., memory, attention, and decision processes; environmental contexts and resources; and social influences). Although there are clear benefits to an occupational therapist addressing this area in an outpatient or home health setting, the primary care setting provides particular benefits for people with limited access to health care, because it reduces demands on the client to make a follow-up appointment and travel for additional services (Gorina et al., 2019). It is also important to consider the research by Khayyat et al. (2019), which identified an association between quality of life and medication adherence specifically in client populations with HTN and T2DM in the primary care setting. The occupational therapist’s role in primary care is in the early stages of its evolution; however, the occupational therapist is well equipped to work with the pharmacy and provider team to improve medication management and adherence.
Conclusions
This study expands the research related to medication management interventions delivered by an occupational therapist—specifically, a manualized approach with the IMedS. It supports the conclusion that an occupational therapist can positively influence adherence, with an emphasis on the use of motivational interviewing to coach a client through the analysis of his or her roles and routines and how medication management strategies can be better integrated into meaningful activities. Future research should include the implementation of the IMedS with a larger sample size and over a longer period to identify possible differences between groups and to further examine the impact of the occupational therapy process on behavioral versus biological factors.