
Abstract
The Family Assessment of Quality in Self-Care Engagement (FAQ–Self-Care) is a promising tool that highlights the influential life factors that intersect with the self-care participation of families raising neurodiverse children on the autism spectrum.
Throughout every walk of life, families become a strong foundation for their child’s neurophysical, cognitive, and psychosocial development (DeGrace et al., 2014; Hillman et al., 2017). The intrinsic meaning that families create, find, or are met with on their journeys with their child has been found to be the driving force that enables families to conjure up the daily strength and resilience needed to provide intricate support to their child (Chiaraluce, 2018). Families’ diverse use of cognition almost intuitively gifts them with the ability to understand who their child is and what their child’s needs are. Families continuously create and integrate meaningful strategies to support their adaptation to and fulfillment of their care occupations (Schiavone et al., 2018). For instance, families may create unique occupational lives, from choosing to be a stay-at-home parent to having flexible full-time employment, to balance attending to their child’s immediate needs and routine care schedules (e.g., going to medical or health appointments, coordinating school drop-offs and pick-ups, eating at mealtime; Bagatell, 2016; Ozdemir & Koç, 2022). Families may configure ways to help their child perform their activities of daily living (ADLs), such as getting ready for school in the morning while simultaneously doing their routines or activities of interest (e.g., making coffee, preparing for the workday; Lim et al., 2022). Families may also navigate toward forming strong connections with their child through meaningful child- and family-focused activities (McDougall et al., 2014). Many families tend to greatly adapt their lives and occupational involvement to care for their child, and even multiple children. However, families caring for their exceptional child or children on the autism spectrum have a greater level of caregiver vigilance (Goodwin et al., 2022 ; McAuliffe et al., 2019). With this great devotion to being vigilant caregivers comes a significant influence on families’ holistic health outcomes, including their self-care (McAuliffe et al., 2022).
Self-Care in the Scope of Family Practice
Self-care is a multifaceted and rather ambiguous term that becomes molded by diverse individuals, populations, and societies. Aligned with the scope of family practice, self-care is defined as a wide range of meaningful activities that families desire to, want to, or choose to do within and apart from their roles as care providers as they navigate their occupational lives. Engaging in such activities is powerfully intertwined with families’ perceived quality of life and further shapes families’ relational and physical health in addition to their mental or intrapersonal, socioemotional, cultural, and political wellness (Chafouleas et al., 2020; Hooker et al., 2020).
Current Family-Centered Assessment Practices
In the realm of family-focused care, many self-care assessments used by medical and health professionals address prerequisites of self-care such as individuals’ participation in activities to support daily living (e.g., bathing, dressing) rather than examining families’ holistic self-care. However, the perspectives surrounding self-care have been significantly expanding (Butler et al., 2019; El-Osta, 2019; Laposha & Smallfield, 2020). For instance, the Denyes Self-Care Practice Instrument (DSCPI–90; Denyes, 1990) is derived from Orem’s Self-Care Deficit Nursing Theory (Orem 1980, 1985). Briefly, this theory defines self-care as care for oneself and posits that self-care agency or ability precedes the performance of self-care. Given Orem’s translation of the concept of self-care, the DSCPI–90 evaluates adolescents’ and adults’ ability to care for themselves and to make decisions about, as well as perform, self-care activities that promote their health (Andrews et al., 2009). Although the term self-care is not specifically referred to in the Life Participation for Parents (LPP; Fingerhut, 2005) assessment tool, it contributes to an examination of the fullness of families’ participation and balance achieved in life occupations as families provide specialized care to their child or children. Using the LPP, families can intricately assess their participation in areas that include engaging in social and community activities, receiving emotional support, and performing household management. More recently, the My Family’s Accessibility and Community Engagement (My FACE; Bourke- Taylor et al., 2021, 2022) assessment tool was developed. The My FACE assessment is guided by the Person–Environment–Occupation Model and thereby focuses on children with special abilities, their families, and their adaptation within their communities, particularly their level of engagement and inclusion (Bourke-Taylor et al., 2021, 2022). Other tools, including the Health Promoting Activities Scale (Bourke-Taylor et al., 2012), collectively assess the frequency of participation and the health-defined aspects that promote lifelong participation.
Family functioning is also important to the discussion of families’ self-care. Widely used assessments that provide a vital view of families’ perceived burden and stress in caring for children with multiple conditions or severe illnesses include the Parental Stress Index (Abidin, 1983, 1986) and the Caregiver Burden Inventory (Novak & Guest, 1989), respectively. The Beach Center Family Quality of Life Scale (Beach Center on Disability, 2006) analyzes key life dimensions such as family interaction and intrapersonal well-being with regard to the satisfaction of families and family members with disabilities as they navigate life together. Furthermore, other scales, such as the Impact on Family Scale (Stein & Riessman, 1980), in addition to the combined use of semistructured interviews and self-designed surveys, assess internal and external demands, including sociodemographic factors (e.g., financial and culture-driven stressors) that affect families.
The current climate has been geared toward supporting individuals’ health across meaningful self-care practices, so this “push” and same vigor must be exemplified throughout practice. By creating meaningful assessments that use integral pieces from theoretical models (e.g., stress, family functioning), and unifying current assessment practices, families can deeply address their unmet needs and desires for self-care (Honaker, n.d.; Zaidman-Zait et al., 2018). Thus, assessments that focus on the quality of families’ self-care may be just what is needed to bridge this current gap in practice.
The Family Assessment of Quality in Self-Care Engagement Assessment Tool
The Family Assessment of Quality in Self-Care Engagement (FAQ–Self-Care) assessment tool was inspired by the inherent need to focus on families’ self-care. The FAQ–Self-Care is derived from premises of the Family Adjustment and Adaptation Response Model (McCubbin & Patterson, 1983), which describes the interrelationships between biophysiological and psychosocial factors that are part of micro and macro family systems and their influence on families’ life process of adaptation (Patterson, 1988). The FAQ– Self-Care analyzes the demands posed by three tiers (the individual, family, and community), in addition to the supports and resources that can be accessed across these tiers, and the impact that such demands have on families’ capability to participate in or actually perform self-care. The overall purpose of the FAQ–Self-Care is to enable families who are raising a child or children on the autism spectrum to self-assess the factors that influence their participation in meaningful self-care activities. The nonstandardized nature of this tool ensures that families’ first-hand perceptions and experiences are subjectively captured.
An extensive literature review of family life and the care of children on the autism spectrum supported test item construction. Recurrent themes, such as informal and formal support systems, balancing care occupations, and the frequency of routines, were organized into three subdomains (Figure 1). A total of 22 test items were created across the subdomains of Life Performance Patterns, or family care routines (5 items); Perceptions of Occupational Involvement, or families’ experiences and beliefs about their self-care (12 items); and Contexts and Environments, or the internal and external supports as well as resources that families have to participate in self-care (5 items). With careful test-item selection, the FAQ–Self-Care is intentionally framed through a strength-based lens to help families assess the variables that influence their liberty to choose when, where, and how they will engage in meaningful self-care activities, using a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). In addition, families can choose to complete this assessment on their own or with professional support.
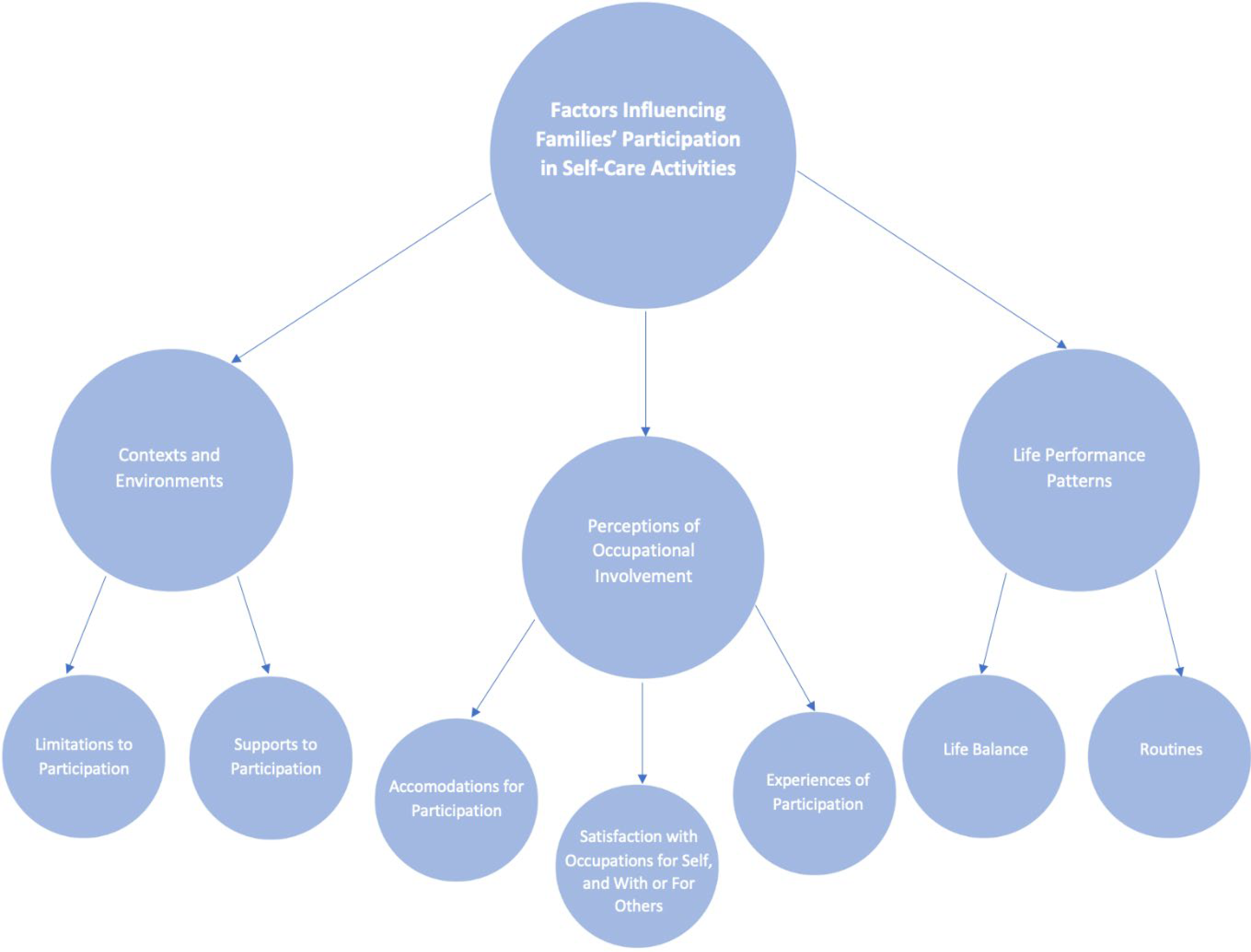
Latent, sublatent, and observable variables.
Method
Research Design
A mixed-methods study design was used to assess qualitative data regarding item relevancy and expert responses on the FAQ–Self-Care, in addition to statistical correlates through quantitative analysis. Content validity concerns the degree to which a scale has an appropriate sample of items to represent the construct of interest—that is, whether the domain of content for the construct is adequately represented by the items (Polit et al., 2007). In the health care professions, the most widely used method of quantifying content validity for multi-item scales is the content validity index (CVI), which is based on expert ratings of relevance (Polit & Beck, 2006).
Participants
Ten occupational therapists were invited as expert reviewers to assess the FAQ–Self-Care. They were chosen on the basis of the following qualities: current specialty area or areas aligned with pediatrics and family-centered practice, at least 10 yr of practice experience in working with families of children on the autism spectrum, and any presentations or publications related to the topic. Experts were recruited through a review of presentations or publications related to the topic using a library database search. Once contact information was gathered, experts were invited to participate in the study via email and signed a formal consent. The review process occurred through Qualtrics, an online survey platform. A total of 6 experts opted to complete the review of the FAQ– Self-Care. This study was approved by the Columbia University Institutional Review Board.
Data Collection
Although formal training was not included in this course of study, content experts were provided with an explanatory cover letter detailing an operational definition of the term self-care; the purpose of this study; and a description of the FAQ–Self-Care, including scoring, before proceeding with the review on the Qualtrics survey platform. Experts were given 6 wk to review the FAQ–Self-Care. Experts ranked the relevance of the 22 items on the FAQ–Self-Care using a 4-point ordinal scale on which 4 = highly relevant, 3 = moderately relevant, 2 = minimally relevant, and 1 = not essential (Davis, 1992), according to the factors that strongly influence the self-care of families with children on the autism spectrum. Experts were also given a space to provide qualitative feedback for each test item to support further refinement of this assessment tool.
Data Analysis
We analyzed the quantitative data in Microsoft Excel, calculating the item-level CVI (I-CVI), scale-level CVI (S-CVI), probability of chance, and the modified κ (K*). However, only the I-CVI and S-CVI are reported in Table 1. In addition, frequency ratings and mean percentages were generated through an automatized system on Qualtrics.
The I-CVI is a strong determinant of the proportionality of relevant items that were rated by the panel of experts (Fawcett, 2007). According to Polit and Beck (2006), an I-CVI score can be calculated by providing a sum of ratings that are declared to be highly and moderately relevant and dividing the summated ratings by the number of content experts. A CVI of 0.80 or higher is considered to have good to excellent content validity. However, items with attributed content validity scores falling within the 0.51 to 0.70 range necessitated further revisions (Polit et al., 2007). An S-CVI score was also generated to analyze the appropriateness of using a 4-point Likert rating scale to distinctly evaluate the indicated items on the FAQ–Self-Care. An S-CVI score of 0.80 to 1.00 is acceptable. Obtaining an S-CVI score entailed summating all I-CVI scores and then dividing the total I-CVI score by the total number of test items (Polit et al., 2007).
The CVI analysis captures interrater agreement but not full interrater agreement (Polit et al., 2007). To account for the probability of random agreement between multiple raters, the probability of chance statistic was used to rule out the odds of experts providing the same rating per test item because of confounding biases or test-related variables. Thus, the chance agreement should be closer to a value of 0 than to 1. A modified κ analysis was also conducted to assess the fidelity of the ratings that were provided by all experts in addition to the level of agreement that occurred across expert raters (McHugh, 2012). A modified κ value of 1 or close to 1 was considered to have near-perfect to perfect interrater agreement per item (Sim & Wright, 2005). The modified κ index was recommended by Polit et al. (2007) as an additional supporting value to account for chance agreement between multiple raters after accounting for the probability of random agreement between raters. When the modified κ index score is close or of similar value to the I-CVI, there is stronger confidence in the agreement among raters about how essential each test item is in measuring the theoretical construct.
To obtain the I-CVI, we used the equation I-CVI = (n
3 + n
4)/N, in which n
3 represents the number of experts who provided a score of 3 (moderate relevance), and n
4 represents the number of experts who scored test items as 4 (high relevance). Both n
3 and n
4 are summated, and then the resulting value is divided by N, or the total number of experts. The S-CVI was configured by using the equation S-CVI = SUMI-CVI/n
items. I-CVI indices were summated and then divided by the number of FAQ–Self-Care test items. The probability of chance was calculated using the equation P
c = 0.5
N
, where N represents the total number of experts. Last, the modified κ was determined by applying the probability of chance to the formula
Given qualitative feedback, the content experts provided their comments anonymously. Each comment was thoroughly reviewed on an individual basis per test item by the primary author (Valencia Steele). Common themes that emerged were cross-analyzed and later transcribed into four specific categories: item clarity or word use, test item distinction, the definition as well as the translation of the term self-care, and description of self-care activities. Depending on the complexity of the feedback provided, comments were either split or reduced and organized into the thematic category that was determined to be the best fit.
Results
Demographics
All respondent occupational therapists reported having more than 10 yr of practice experience and attaining at least a master’s degree. Most occupational therapists indicated having at least one publication in addition to providing six or more presentations in a specialty field related to pediatrics, family practice, or both.
Study Outcomes
Table 1 provides a summary of CVIs that is based on 6 experts’ review of the FAQ–Self-Care test items. Frequency ratings and mean percentages were also observed (not shown). The majority of test items (20 of 22) were rated “highly relevant” by experts; thus, mean percentages were 66.6% or greater. Corresponding I-CVI scores also ranged from 0.833 to 1.000. Moderate relevancy was favored for two test items (Items 4 and 9); however, the I-CVI scores fell within an acceptable range. Although mixed ratings were provided for 15 test items, no more than 2 respondents attributed ratings that were less than moderately relevant, which was equivalent to mean percentages of 33.3% or lower. However, only 2 items (Items 3 and 16) that received mixed ratings required significant revisions because of an I-CVI score of 0.667. Given qualitative data, Item 3 was revised because of the lack of a clear distinction between test items. With comments regarding the limited synchrony of Item 16 with other test items (e.g., the frequency of self-care), further revisions were made. Minimal revisions were required for the other 20 items in congruence with experts’ feedback. Most experts suggested that this assessment tool could be strengthened by ensuring that items are actively stated and can be understood by the families for whom this tool is intended, especially the discussion of self-care. Other comments aligned with creating distinctions between or among test items and providing a consistent set of examples of self-care activities that can be relatable to most, if not all, families’ lives. Few comments regarded the sequencing of test items and the inclusion of extended family members.
Statistical Analysis of Test Items on the FAQ–Self-Care
Note. Item 3 (Family Routines and Daily Activities) and Item 16 (Prioritizing Self-Care) were revised as a result of an I-CVI score of 0.667. FAQ–Self-Care = Family Assessment of Quality in Self-Care Engagement; I-CVI = item-level content validity index; S-CVI = scale-level content validity index.
Overall, modified κ values were consistent with the I-CVI values in Table 1, which indicates that the ratings provided by experts across test items were relatively consistent. According to qualitative data analysis, a recurrent area of commentary surrounded the term self-care because the experts were introduced to a novel definition of self-care. For example, one expert stated, “[There is an] issue of defining self-care as pertaining to self and others.” Other responses included that self-care will be interpreted differently and viewed or shaped by different individuals, even though “a broader definition is offered than most [occupational therapists] are used to.” Although a definition of self-care was proposed, 1 respondent highlighted that, without a strong mapping of self-care from the Occupational Therapy Practice Framework (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020), there is still great difficulty in its translation across practice. Thus, there is still a need to form a comprehensive view of self-care that is applicable to all individuals and goes beyond participation in ADLs.
Discussion
The vigilance of care that families specially provide for their child or children on the autism spectrum, in addition to facing myriad life challenges, leads to significant health outcomes, including caregiver burnout (Patty et al., 2021 ; Zaidman-Zait et al., 2017). The quality and strength of support systems, along with the ability to engage in self-care, further contribute to the impact on families’ health across areas concerning their mental, emotional, physical, and sociocultural wellness (Kuhlthau et al., 2014). Given the ongoing need to improve the focus on the holism of families’ health, particularly through their participation in self-care activities, a family-focused assessment tool, the FAQ–Self-Care, was developed. The overall intent of this study was to provide preliminary content validation of this assessment tool.
Although initial content validation occurred in correspondence with 6 expert reviewers, the FAQ–Self-Care has yet to be validated with the intended population of families with children on the autism spectrum. To strengthen its content validity, continued studies on the FAQ–Self-Care should involve families’ input and gauge the level of agreement between raters per test item. The focus will then be to establish construct validity through methodical testing of hypothesized relationships between the potential performance of individual test items and the variations found in families’ responses. In addition, thorough evaluation of the test items and corresponding subscales is necessary to determine whether the FAQ–Self-Care represents the primary construct of the factors influencing families’ self-care.
Within the scope of this study, a novel perspective of self-care was also introduced. In comparison, the OTPF–4 centers on the therapeutic nature of meaningful activities as a means by which individuals are motivated to participate and an outcome in which holistic health is achieved (AOTA, 2020). However, the OTPF–4 falls short of depicting the concept of self-care in addition to creating strong connections that link self-care and its related attributes—such as having “me time,” spending quality time with family and friends, and engaging in activities that are infrequently done—with the foundation of occupational participation. With the current translation in practice, self-care has become synonymous with ADLs such as bathing and dressing (AOTA, 2020). Given the breadth and depth of self-care, a clear definition that bridges participatory and health outcomes is necessary.
In addition, the findings from this study on the FAQ–Self-Care should be carefully interpreted until further rigorous studies are conducted. The first-time use of the term self-care in the context of families’ participation may have led to differences in expert agreement on what constitutes self-care and, hence, related scoring. As the meaning of self-care is diverse, a unified view of self-care that embraces its dynamic nature and the unique characteristics that are shaped by individuals and the sociocultural spheres of which they are a part is necessary.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: There is a need to develop and validate tools that thoroughly depict the unmet needs of families of children with special abilities in addition to families caring for loved ones. Such tools can provide focused support in addressing the needs that are central to families’ lives. Further research is needed to undertake the process of construct validating the FAQ–Self-Care in addition to using other psychometric tests such as goodness of fit and properties such as clinical utility to ensure the precision of and level of confidence in using this assessment tool.
Conclusion
Overall, this study contributes to the body of knowledge in creating a family-focused assessment tool that centers on the self-care of families raising children on the autism spectrum. Furthermore, professionals are geared to focus on families’ holistic health given the outlook on self-care that is provided.
Footnotes
Acknowledgments
The authors thank the wonderful content experts who took their time out to review and contribute to the fine-tuning of this assessment tool. The authors declare no conflict of interest.