
Abstract
This study identified occupations that enhance an inherent sense of responsibility among people with Parkinson’s disease (PD). Subjective knowledge of one’s actions and their consequences lie behind people’s daily occupations and their outcomes. Taking this knowledge into consideration when administering occupation-focused interventions can be beneficial for individuals with PD.
Parkinson’s disease (PD) is a neurodegenerative condition characterized by difficulties with voluntary movements. Reduced output from the basal ganglia to the presupplementary motor area leads to decreased initiation of actions (Haggard, 2008). The ability to perform voluntary actions is crucially important to humans, yet it can be disrupted by neurological disorders such as PD (Rowe & Wolpe, 2014). Voluntary activities play a critical role in generating a sense of agency (SoA; Moore et al., 2010). The SoA as a subjective experience (i.e., the experience of controlling one’s actions and their consequences) underpins the concept of responsibility for one’s daily occupations and their outcomes (El Zein et al., 2019; Yano et al., 2020). To the best of our knowledge, although the concept of responsibility and SoA has been studied in diverse disciplines (Coyle et al., 2012; Maeda et al., 2012; Minohara et al., 2016; Nierula et al., 2021), it has not yet been investigated in rehabilitation practice.
Responsibility depends greatly on the brain circuits underpinning SoA and voluntary actions (Haggard, 2008, 2017). According to the model of human volition, performing actions has both motivational and volitional components (Haggard, 2008). Responsibility has a key association with motivation and volition (Beck et al., 2017; Taylor & Kielhofner, 2017), and higher motivation and volition tend to have a positive relation with participation (Harel-Katz & Carmeli, 2019; Li et al., 2011). Moreover, responsibilities are an inherent part of people’s daily life roles, especially roles such as parent or worker (Taylor & Kielhofner, 2017). In movement disorders such as PD, disruptions in responsibilities and SoA have significant consequences for quality of life (Haggard, 2017). Hence, incorporating the concept of responsibility in rehabilitation programs may promote health, quality of life, and occupational participation among people living with PD.
People with PD experience difficulties with their daily occupations and experience decreased responsibility for participating in them (Benharoch & Wiseman, 2004; Taylor & Kielhofner, 2017). The involvement of multiple professions in PD management has been recognized in the literature (Levy et al., 2020; Sturkenboom et al., 2014; van der Marck et al., 2013), but the concept of responsibility has not yet been considered. The literature has proposed that responsibility is higher in active and free-choice conditions with more alternatives (Caspar et al., 2016, 2018). Client-centered and occupation-focused practice in occupational therapy actively integrates clients into the decision-making process of intervention (Mroz et al., 2015). Using client-centered occupations with an emphasis on the concept of responsibility may be one therapeutic approach to increasing client participation (Taylor, 2017). The dearth of research regarding the concept of responsibility in rehabilitation hampers practitioners in delivering evidence-based care according to this concept.
The Delphi method is a well-known methodology for establishing expert consensus on issues when the existing literature is limited (Hohmann et al., 2018). Expert consensus on the selection of appropriate occupations will help clinicians increase patient compliance with rehabilitation services and improve outcomes. In the current study, we used the Delphi methodology to form consensus and explore an area beyond the existing literature. Our first aim was to generate a list of occupations that enhance the inherent sense of responsibility among people with PD that was based on consensus among experts. We hypothesized that rehabilitation practitioners may use diverse occupations according to the client’s condition and roles. Certain types of responsibilities are suitable for individuals depending on their abilities, interests, characteristics, and socioeconomic positions (Frantik, 2018). Hence, the second aim of our study was to identify the importance of patient-related information when selecting an occupation, with an emphasis on occupations that have the potential to enhance a sense of responsibility.
Method
Study Design
This two-round, anonymous, and iterative Delphi study was conducted according to the Guidance on Conducting and REporting DElphi Studies (CREDES; Jünger et al., 2017). The Ethics Committee of the Iran University of Medical Sciences approved the study protocol (IR.IUMS.REC.1400.753). Participant anonymity was guaranteed by assigning an identification code to each completed questionnaire. Informed consent was obtained from all individual participants in the study.
Participants
To recruit participants, a preliminary email describing the aim of the study, detailed information the study’s purpose, and instructions was sent to renowned experts in the management of PD. Our objective was to recruit a group of international experts with various professional backgrounds, including physical therapists, occupational therapists, speech-language pathologists, general practitioners, neurologists, neuroscientists, psychologists, and psychiatrists. Professionals were invited (1) if they were clinicians or researchers and (2) had the ability to read and write in the English language. Health professionals were identified through their research interests, clinical expertise, and recently published articles and through academic university profiles and occupational therapy and physical therapy association lists (Association of Occupational Therapists of Ireland, Canadian Association of Occupational Therapists, WA Occupational Therapy Association, Australian Physiotherapy Association, Occupational Therapy Australia) by means of a Google search.
According to de Villiers et al.’s (2005) recommendations, participants were considered eligible if they were clinicians or researchers with the professional qualifications required for diagnosis or management of people with PD. Participants were allowed to contact us if they had questions while completing the questionnaires. Approximately 669 potential participants were invited through the invitations disseminated by email. According to the Consensus-based Standards for the Selection of Health Measurement Instruments recommendations, we planned to enroll at least 100 experts in the first round (Terwee et al., 2018), and 116 experts agreed to participate in the first round of the study (Figure 1).
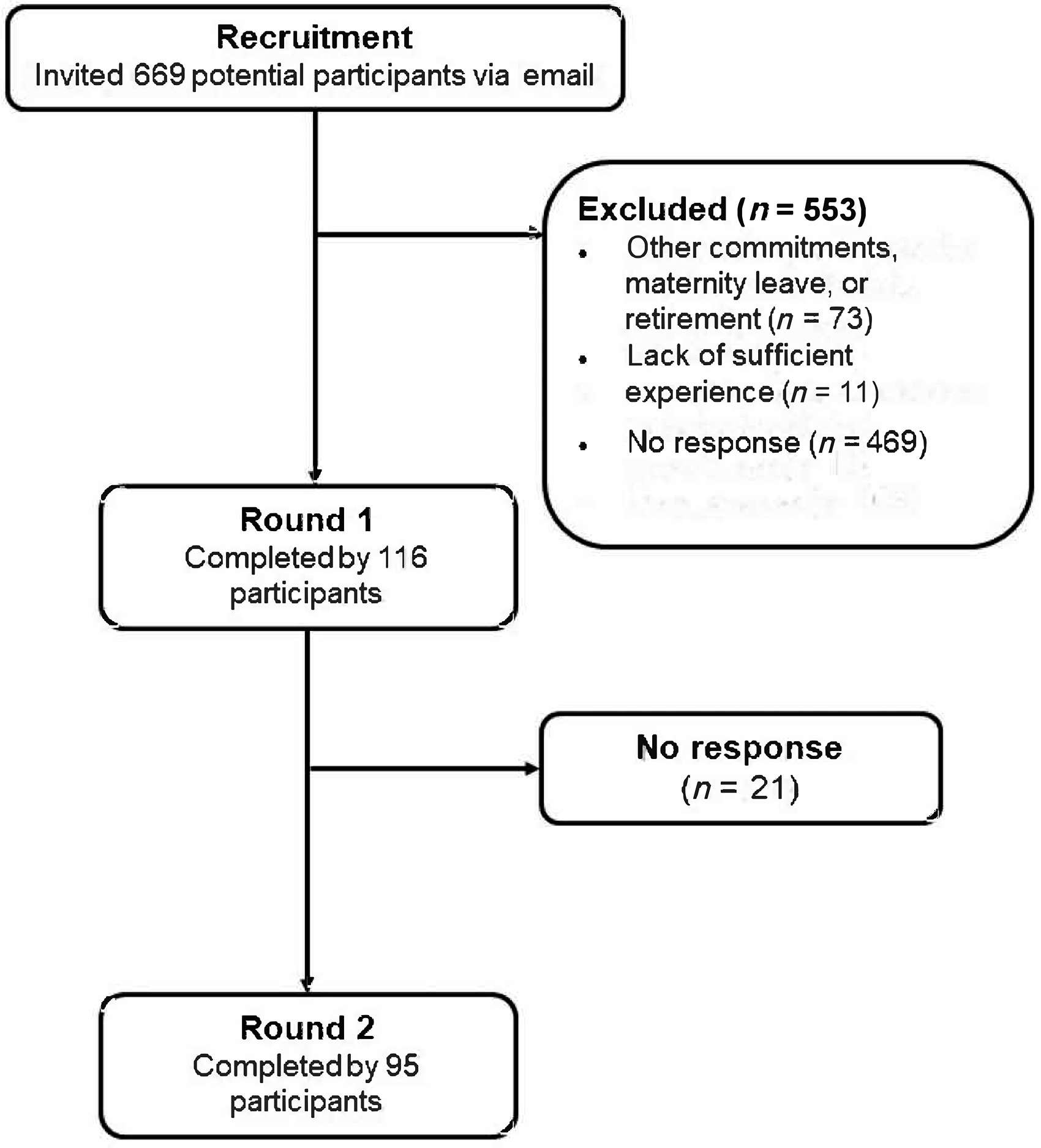
Flow diagram of the stages of the Delphi process.
Developing the List of Occupations With Diverse Inherent Responsibilities and Patient-Related Information
We defined responsibility as accountability for one’s actions and their consequences (Bednar et al., 1974). The cognitive basis for feeling responsibility is the intentional binding mechanism that connects intentions to outcomes (Frith, 2014). The process of attributing their own actions to themselves provides people with a sense of control and makes them accountable for the effects of their actions (Gallagher, 2000; Nierula et al., 2021). An SoA creates the basis for a feeling of responsibility for one’s activities (Haggard & Tsakiris, 2009). This sense of responsibility is crucial for maintaining social cohesion (Frith, 2014). Therefore, we considered three distinct forms of responsibility—being responsible to oneself, being responsible to family members, and being responsible to other people in society—in generating a long list of occupations, with potential overlaps among them (Eliasa, 2014). The applicability and convenience of occupations in clients were emphasized.
We initially developed a list of 77 occupations in which people with PD have an inherent responsibility that were based on data gathered from semistructured interviews with rehabilitation experts, related literature, and our clinical experience (American Occupational Therapy Association [AOTA], 2020). Occupations included in the list were elements of good clinical practice and were known to enhance participation (AOTA, 2020). In addition, we prepared a list of 38 types of patient information that are important when patients and therapists are choosing an occupation, with an emphasis on occupations that have the potential to enhance a sense of responsibility. This patient-related information was also explored on the basis of our clinical experience and on semistructured interviews with experts in PD management.
Procedure
Following a pilot study and minor grammatical changes by three professionals, the questionnaires were sent to all participants using Google Forms. Participants were asked to provide their age, gender, profession, highest level of education, region of practice, years of experience in the management of PD, and Hoehn and Yahr Scale stage of the people with PD (Goetz et al., 2004) with whom they most frequently worked. To maximize the response rate, two reminder emails were sent for each round.
In the first survey round, the list of occupations and types of information were presented to the experts. The survey included an open-ended question to which experts could respond with additional occupation categories or types of patient-related information. Experts were asked to rate the level of inherent responsibility in each occupation and the importance of each type of patient-related information on a 5-point Likert scale (1 = very low responsibility/not at all important, 2 = low responsibility/unimportant, 3 = moderate responsibility/uncertain, 4 = high responsibility/important, 5 = very high responsibility/very important). This round lasted 9 wk. Items on which the participants reached consensus were eliminated from the next round, in compliance with the Delphi methodology (Jünger et al., 2012).
In the second round, 15 additional occupations and 16 patient-related types of information were added to the lists on the basis of the experts’ suggestions, and the questionnaires were sent to the experts who completed the previous round. In addition, the response statistics for each occupation category and type of information from the previous round were sent. Experts were asked to reconsider their previous ratings by reviewing the response statistics for the previous round to establish consensus with other experts. The duration of this round was 5 wk.
Data Analysis and Definition of Consensus
Quantitative statistical analyses were performed with Microsoft Excel 2016 and IBM SPSS Statistics (Version 16.0). For each occupation and type of patient-related information, we calculated the median (Mdn) and interquartile range (IQR) for the Likert-scale ratings. Consensus was defined as an IQR of ≤1 for each occupation (Jünger et al., 2012). The predetermined consensus criterion for each type of patient-related information was set as an IQR ≤1 and a Mdn of ≥4 (Ab Latif et al., 2017 ; Hasson et al., 2000). Subgroup analyses were performed for occupations and type of patient-related information according to gender, years of experience, and Hoehn and Yahr Scale stage of PD of patients with whom the experts most frequently worked. The Kruskal–Wallis test was used to investigate differences among experts in median ratings of occupations in regard to region of practice. A p < .05 was considered significant.
Results
In the first round, responses were obtained from 116 international experts from 16 countries with a variety of geographical locations. Ninety-five (81.89%) participated in the second round. The experts’ mean age and years of experience were 36.93 (SD = 12.19) and 8.39 (SD = 7.60), respectively. The majority of respondents were occupational therapists (n = 76; 65.51%). Experts were clinicians, researchers, or both. The demographic characteristics of the Delphi panel are summarized in Table 1.
Demographic Characteristics of the Delphi Expert Panel (N = 116)
Note. Percentages may not total 100 because of rounding.
Percentages are calculated as the number of patients at each stage divided by the number of experts.
In the first round, consensus was reached on 19 of 77 occupations. Also, consensus was achieved regarding all 38 types of patient-related information. Five types of patient-related information—“living alone or with others,” “severity of activity limitations,” “balance disorders,” “cognitive function,” and “psychological disorders”—were considered very important when choosing an occupation with an emphasis on the concept of responsibility for intervention (Table 2 and Appendix Table A.1).
Importance of Each Type of Patient-Related Information When Selecting Occupation-Focused Interventions
Note. Types of patient-related information are arranged in descending order. Types of information were rated on a 5-point Likert scale ranging from 1 (not at all important) to 5 (very important). IQR = interquartile range; NA = not available; PD = Parkinson’s disease.
New patient-related information added in Round 1.
In the second round, consensus was reached for all the presented occupations and types of patient-related information. Moreover, consensus was reached on additional occupations and types of patient-related information proposed by respondents. Of the 16 additional types of patient-related information, “on and off medication phases,” “motivation,” and “reliance on rehabilitation” were deemed very important. “Social interactions with other people with PD” and “leisure and recreational interests” were also considered to be important. However, “having children,” “family problems, such as financial issues,” “living in urban or rural areas,” “awareness of the disease,” “self-confidence,” “awareness of the concept of responsibility,” “culture,” “pragmatism in managing symptoms,” “availability of support based on location,” “ecological status in place of residence, such as pollution,” and “presence of domestic animals” were regarded as uncertain.
In subgroup analyses, the ratings of the level of inherent responsibility for each occupation were similar regardless of profession, panelists’ gender, years of experience, and Hoehn and Yahr Scale stage of PD of patients with whom they most frequently worked. We found no significant difference among experts in regard to region of practice in all occupations, except “going to clinical appointments and maintaining contact with health care practitioners” (p = .001), “feeding pets at home” (p = .011), “planning a routine for meaningful activities” (p = .002), “engaging in leisure activities” (p = .044), “gathering information about their disease” (p = .004), “doing physical activities or walking” (p = .0001), “making sure about safety” (p = .022), “present[ing] a book, film, etc. [to] family members/friends” (p = .002), “disseminating useful and practical contents” (p = .024), and “remembering to drink 8 glasses of water daily” (p = .003).
In addition, panelists reached consensus on all types of patient-related information regardless of whether they were occupational therapists or male. However, we found a difference in the number of types of patient-related information on which consensus was reached for physical therapists and female experts. Physical therapists reached consensus on all of the patient-related information except for “presence of domestic animals” (IQR = 1.5), “having children” (IQR = 2.0), and “gender” (IQR = 3.0). Furthermore, female panelists reached consensus on all types of patient-related information except for “personality type,” “PD onset,” and “having children” (IQRs = 2.0). Panelists with 2 to 4 yr of experience in PD management reached consensus on all patient-related information except for “personality type” (IQR = 1.5). Panelists who work most frequently with people living with Hoehn and Yahr Scale Stages 2 and 3 of PD reached consensus on all patient-related information except for “personality type” and “marital status.”
Discussion
Through a two-round Delphi procedure involving heterogeneous health specialists in PD management, occupations were rated on their inherent sense of responsibility. Sixty-one occupations were deemed as having a moderate to very high inherent sense of responsibility. In addition, our results showed that experts consider a wide range of patient-related information as very important or important when selecting an occupation that has the potential to enhance a sense of responsibility.
In the second round of the study, we found changes in the median scores of several occupations, which were influenced by the input from the first round’s response data. “Responsibility for remembering his/her own medication hours” was considered an occupation with very high inherent responsibility. This finding is in line with the results of Grosset and Grosset’s (2007) study, which indicated that the timing of medication usage is potentially important in PD management. Furthermore, medication management interventions have been recognized in occupational therapy practice as ameliorating occupational participation (AOTA, 2017 ; Foster et al., 2021). Thirteen occupations, such as “maintaining personal hygiene,” “dressing and undressing his/her own [self],” and “personal device care” were deemed to have high inherent responsibility. Also, 47 occupations, such as “home maintenance,” “taking out garbage from home,” and “washing his/her own clothes,” were considered to have moderate inherent responsibility. In a Delphi survey of best occupational therapy practice for people with PD, Deane et al. (2003) reported that more than 95% of occupational therapists would focus their intervention on improving or maintaining domestic skills, washing, and dressing, which is in line with the results of the current study. Wannheden and Revenäs (2020) reported that health professionals expect people living with PD to take responsibility for activities that are important for their health and to be more independent in self-care activities. Rehabilitation is an ongoing process, and clients should feel a sense of responsibility in the intervention process (Baskett et al., 1999). Moreover, increased patient involvement creates greater responsibility, which leads to increased motivation and participation (Grosset et al., 2005; Li et al., 2011).
Significant differences in ratings of some occupations between experts in different regions of practice may be explained by each country’s different cultures and social contexts. Patients residing in distinct contexts may have a different inherent sense of responsibility in these occupations as a result of diverse circumstances.
Dosing in rehabilitation is a critical element with different parameters, such as frequency, intensity, and duration (Jette, 2017). Evidence does not support low-dose occupational therapy (i.e., using occupations that have a low or very low inherent sense of responsibility) for people with PD (Clarke et al., 2016). Occupational therapy dose is dependent on the client’s goals and progress through the intervention process (Sackley et al., 2009). Occupations can be graded and modified to fit the client’s abilities, capacities, and interests as well as to provide the potential for promotion of occupational performance (Che Daud et al., 2015). Occupational therapy services should be organized with respect to clients’ changing needs and abilities as a result of the progressive nature of the disease (Deane et al., 2003).
Patient-related information is associated with occupational therapy service delivery (Sackley et al., 2009). Our results regarding patient-related factors associated with rehabilitation are supported by previous findings (Lam Wai Shun et al., 2017; Malcolm et al., 2021; Oyake et al., 2020). Further research is needed to explore the occupation-focused interventions that occupational therapists deliver on the basis of client factors.
Consensus-based procedures are recognized as providing a lower level of evidence than experimental designs, such as randomized controlled trials (Atkins et al., 2004). Therefore, future research is required to move beyond this Delphi study and augment the implementation of occupation-focused interventions. We recommend that future experimental studies be required to translate this research into clinical practice.
Strengths and Limitations
The findings from this Delphi study represent the multinational consensus of experts from multiple countries with geographical variations in clinical practice. The Delphi process was executed rigorously in terms of using open-ended and closed-ended questions, anonymity, statistical feedback, an a priori criterion of consensus, and adherence to CREDES recommendations (Hohmann et al., 2018; Jünger et al., 2017). The majority of respondents were occupational therapists (65.51%), which is an important strength of the current study because of occupational therapists’ overall clinical role in client-centered and occupation-focused practice.
The results of the current study should be interpreted in light of the limitations of the Delphi methodology. First, the majority of the panelists were recruited from the Middle East (62.0%), which may limit the generalizability of our findings. Second, several professional disciplines had a small number of contributors. Thus, their viewpoints might be understated in the present data. Third, the study data consist of the opinions of experts in this field. In particular, we are unable to specify how experts determined their stated rating for the level of inherent responsibility in each occupation. Fourth, few occupations related to education, work, and leisure were proposed. The level of responsibility inherent in each occupation is idiosyncratic. Therefore, future studies are needed to investigate how people living with PD experience responsibility while participating in occupations. Fifth, communication with experts when questions were raised was conducted by email, which led to limited opportunities for interaction.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: ▪ Occupational therapy practitioners can use the list of occupations in providing occupation- focused care for clients with PD when choosing occupations as a means or an end. ▪ Occupations deemed as having a moderate to a very high inherent sense of responsibility may increase motivation and volition and subsequently promote occupational participation and engagement. ▪ This evidence-based study can inform clinicians and researchers about the dose of inherent responsibility in occupations. A gradual increase in dosing may help in promoting clients’ functional outcomes and better adherence to occupational therapy intervention.
Conclusion
To conclude, 61 occupational categories were deemed as having a moderate to a very high inherent sense of responsibility for people with PD. In addition, a wide range of patient-related information is considered very important or important while delivering these occupation-focused interventions. The outcome of the current study will help occupational therapists strengthen their current practice by considering the concept of responsibility.
Footnotes
Acknowledgments
We acknowledge the contribution of the Delphi panelists for their valuable responses to this Delphi study. This work was supported by Iran University of Medical Sciences, Tehran, Iran.
Appendix
Consensus on Level of Responsibility for Each Occupation in Parkinson’s Disease Management
| Occupations | Mdn (IQR) | |
|---|---|---|
| Round 1 (n = 116) | Round 2 (n = 95) | |
| Responsibility for remembering his/her own medication hours | 4 (2) | 5 (1) |
| Responsibility for maintaining personal hygiene (such as toileting, bathing, washing face, etc.) | 4 (2) | 4 (0) |
| Responsibility for personal device care (such as walking aids, hearing aids, glasses, etc.) | 4 (1) | 4 (1) |
| Responsibility for dressing and undressing [on] his/her own | 4 (2) | 4 (1) |
| Responsibility for medication dose management based on daily activity a | NA | 4 (1) |
| Responsibility for financially supporting dependents a | NA | 4 (1) |
| Responsibility for paid or unpaid work within limits of mental and physical energy and abilities a | NA | 4 (1) |
| Responsibility for maintaining self-employment a | NA | 4 (1) |
| Responsibility for going to clinical appointments and maintaining contact with health care practitioners a | NA | 4 (1) |
| Responsibility to keep daily life as autonomous as before PD a | NA | 4 (1) |
| Responsibility for doing therapeutic exercises/activities a | NA | 4 (1) |
| Responsibility for handling his/her own finances (such as paying bills, getting money from the ATM, etc.) | 3 (2) | 4 (1) |
| Responsibility for buying/providing medicine for his/her own [self] | 3 (2) | 4 (1) |
| Responsibility for taking care of children under 2 yr | 3 (4) | 4 (1) |
| Responsibility for washing his/her own small clothes (socks, etc.) | 3 (2) | 3 (0) |
| Responsibility for buying bread for his/her own [self] | 3 (2) | 3 (0) |
| Responsibility for preparing grocery shopping list needed for a day/week/month | 3 (2) | 3 (0) |
| Responsibility for tidying up his/her own room for a day/week/month | 3 (2) | 3 (0) |
| Responsibility for feeding pets at home | 3 (2) | 3 (0) |
| Responsibility for individual or group religious activities (reciting holy books, prayers, etc.) | 3 (2) | 3 (0) |
| Responsibility for serving cold food for family members | 3 (2) | 3 (0) |
| Responsibility for putting garbage in outdoor trash containers | 3 (2) | 3 (0) |
| Responsibility for taking out garbage from home using chute system | 3 (1) | 3 (1) |
| Responsibility for buying bread for family members | 3 (1) | 3 (1) |
| Responsibility for planning time and place of gatherings with family (face-to-face or virtual) | 3 (1) | 3 (1) |
| Responsibility for washing small dishes (glasses, plates, spoons, etc.) for a day/week | 3 (1) | 3 (1) |
| Responsibility for washing large dishes (pots, pans, etc.) for a day | 3 (1) | 3 (1) |
| Responsibility for tidying up the whole house (living room, etc.) for a day/week | 3 (1) | 3 (1) |
| Responsibility for dusting his/her own room | 3 (1) | 3 (1) |
| Responsibility for taking care of plants/cactus for a month | 3 (1) | 3 (1) |
| Responsibility for gardening for a week | 3 (1) | 3 (1) |
| Responsibility for waking family members up | 3 (1) | 3 (1) |
| Responsibility for keeping others employed if they are a business owner a | NA | 3 (1) |
| Responsibility for planning a routine for meaningful activities a | NA | 3 (1) |
| Responsibility for engaging in leisure activities a | NA | 3 (1) |
| Responsibility for gathering information about their disease a | NA | 3 (1) |
| Responsibility for sexual expression and intimacy a | NA | 3 (1) |
| Responsibility for doing physical activities or walking a | NA | 3 (1) |
| Responsibility for making sure about safety (e.g., checking locks, etc.) a | NA | 3 (1) |
| Responsibility for home maintenance (e.g., repairing, etc.) a | NA | 3 (1) |
| Responsibility for taking caring of children over 2 yr | 3 (2) | 3 (1) |
| Responsibility for buying/providing medicine for family members | 3 (2) | 3 (1) |
| Responsibility for dressing and undressing family members like children, etc. | 3 (2) | 3 (1) |
| Responsibility for buying small and large groceries needed for a day/week/month | 3 (2) | 3 (1) |
| Responsibility to notify other people with PD to participate in group discussions related to the disease | 3 (2) | 3 (1) |
| Responsibility to provide solutions to problems raised in group discussion (active participation) | 3 (2) | 3 (1) |
| Responsibility for cooking cold food for family members | 3 (2) | 3 (1) |
| Responsibility for making a cold or hot drink for his/her own [self] | 3 (2) | 3 (1) |
| Responsibility for serving and cooking cold and hot food for his/her own [self] | 3 (2) | 3 (1) |
| Responsibility for gardening for a month | 3 (2) | 3 (1) |
| Responsibility for reminding family members when to take medication | 2 (2) | 3 (1) |
| Responsibility for washing all his/her own laundry | 3 (2) | 3 (1) |
| Responsibility for handling finances (paying bills, getting money from the ATM, etc.) for family members | 3 (3) | 3 (1) |
| Responsibility for serving hot food for family members | 3 (3) | 3 (1) |
| Responsibility for buying bread for friends | 2 (2) | 3 (1) |
| Responsibility for leading group discussions related to the disease (summarizing discussions, etc.) | 2 (2) | 3 (1) |
| Responsibility for washing large dishes (pots, pans, etc.) for a week | 2 (2) | 3 (1) |
| Responsibility for tidying up the whole house (living room, etc.) for a month | 2 (2) | 3 (1) |
| Responsibility for making a hot drink for family members | 2 (2) | 3 (1) |
| Responsibility for dusting the whole house (living room, etc.) | 2 (2) | 3 (1) |
| Responsibility for cooking hot food for family members | 2 (3) | 3 (1) |
| Responsibility for participating in volunteer or charity activities (such as fundraising, etc.) by online advertising, active participation, or going to NGOs or individuals who do charity work | 2 (2) | 2 (0) |
| Responsibility for reminding family members about exercise time | 2 (2) | 2 (0) |
| Responsibility for taking care of plants/cactus for a week | 2 (1) | 2 (1) |
| Responsibility for washing small dishes (glasses, plates, spoons, etc.) for a month | 2 (1) | 2 (1) |
| Responsibility for oral presentation in group discussions to solve problems related to the disease | 2 (1) | 2 (1) |
| Responsibility for making a cold drink for family members | 2 (1) | 2 (1) |
| Responsibility for planning time and place of gatherings with friends (face-to-face or virtual) | 2 (1) | 2 (1) |
| Responsibility for arranging a taxi for family members | 2 (1) | 2 (1) |
| Responsibility for making a cold or hot drink for friends | 2 (2) | 2 (1) |
| Responsibility for cooking and serving cold and hot food for friends | 2 (2) | 2 (1) |
| Responsibility for drying small and large dishes for a day/week/month | 2 (2) | 2 (1) |
| Responsibility for washing large dishes (pots, pans, etc.) for a month | 2 (2) | 2 (1) |
| Responsibility for separating wet and dry waste for a day/week/month | 2 (2) | 2 (1) |
| Responsibility to present a book, film, etc. [to] family members/friends | 2 (2) | 2 (1) |
| Responsibility for disseminating useful and practical contents (typing contents or spreading pretyped contents) | 2 (2) | 2 (1) |
| Responsibility for reminding family members to drink 8 glasses of water daily | 2 (2) | 2 (1) |
| Responsibility for washing small clothes (socks, etc.) for family members | 2 (2) | 2 (1) |
| Responsibility for ironing his/her own clothes | 2 (2) | 2 (1) |
| Responsibility for driving a car to give family members a ride | 2 (2) | 2 (1) |
| Responsibility for remembering to drink 8 glasses of water daily | 3 (2) | 2 (1) |
| Responsibility for ironing friends’ clothes | 1 (1) | 1 (1) |
| Responsibility for reminding friends to drink 8 glasses of water daily | 1 (1) | 1 (1) |
| Responsibility for reminding friends about exercise time | 1 (2) | 1 (1) |
| Responsibility for handling finances (paying bills, getting money from the ATM, etc.) for friends | 1 (2) | 1 (1) |
| Responsibility for reminding friends when to take medication (call or text) | 1 (2) | 1 (1) |
| Responsibility for ironing family members’ clothes | 2 (2) | 1 (1) |
| Responsibility for washing all laundry for family members | 2 (2) | 1 (1) |
| Responsibility for buying/providing medicine for friends | 2 (2) | 1 (1) |
| Responsibility for collecting bottle caps (as a recycling activity) for a month | 2 (2) | 1 (1) |
| Responsibility for feeding animals in the park or on the street | 2 (2) | 1 (1) |
| Responsibility for waking friends up (using telephone, etc.) | 2 (2) | 1 (1) |
Note. Occupations are arranged in descending order. Occupations were rated on a 5-point Likert scale ranging from 1 (very low responsibility) to 5 (very high responsibility). IQR = interquartile range; NA = not available; NGO = nongovernmental organization; PD = Parkinson’s disease.
New occupations added in Round 1.