
Abstract
This study found that sensory interests, repetitions, and seeking behavior predicted occupational therapy service utilization by children with autism, whereas other sensory response patterns did not, suggesting a possible referral bias for certain sensory response patterns and the opportunity for occupational therapy practitioners to educate parents and teachers about the scope of practice.
Autism is a neurodevelopmental disability affecting 1 of every 44 U.S. children (Maenner et al., 2021). Sensory features and restricted and repetitive behaviors are symptoms of autism (American Psychiatric Association, 2013) that impair adaptive skills and daily participation to varying degrees (Little et al., 2015). Occupational therapy, which is among the services most commonly accessed by children with autism (McIntyre & Zemantic, 2017), addresses daily occupational performance challenges (American Occupational Therapy Association [AOTA], 2020). Understanding predictors of occupational therapy service utilization is important as a first step toward identifying the amount of services that children with autism may need to address their clinical presentations.
Overall Service Utilization by Children With Autism
Several studies have examined predictors of overall service utilization (i.e., total hours of services across disciplines). Children of minority backgrounds in rural areas with lower household incomes received fewer hours of intervention across therapies than children of majority backgrounds in urban areas with higher household incomes (Bilaver & Havlicek, 2019). An inverse relationship has been found between children’s age and IQ and overall service utilization (Mire et al., 2015).
Findings in the service utilization literature are inconsistent regarding the extent to which autism symptom severity, adaptive behavior, and sensory features predict occupational therapy–specific service utilization. These clinical factors may affect overall service utilization; however, findings vary, potentially because of differences in measurement of these factors (Bilaver et al., 2016; Bilaver & Havlicek, 2019; McIntyre & Zemantic, 2017; Patten et al., 2013).
One study measured autism symptom severity using an instrument that primarily assessed severity of disability not specific to autism (Bilaver et al., 2016), and another measured need for services, rather than the effect of symptom severity, on service utilization (Bilaver & Havlicek, 2019). These differences in measurement of autism symptom severity may contribute to unclear associations with overall service utilization.
Adaptive behavior includes the abilities and skills needed to function in daily life (e.g., eating, dressing, hygiene, social participation; Sparrow et al., 2005). Individuals with autism vary in their functional abilities but tend to display lower adaptive behavior skills than peers (Kanne et al., 2011; Meyer et al., 2018). One study reported that adaptive behavior was not associated with overall service utilization (McIntyre & Zemantic, 2017); however, adaptive behavior is likely to be an important contributor to occupational therapy service utilization because of occupational therapy practitioners’ emphasis on participation in daily life (AOTA, 2020). This study addressed inconsistencies in the service utilization literature by examining the extent to which autism symptom severity, adaptive behavior, and sensory features predict occupational therapy–specific service utilization.
Sensory features in children with autism are evident across modalities, though prevalence varies depending on measures and ages (Ben-Sasson et al., 2019). Sensory features in autism have been classified using various taxonomies, including those related to sensory subtypes (Ausderau et al., 2014; Lane et al., 2014) and to sensory registration and sensitivity (Dunn, 2014). We adopted a four-pattern taxonomy of sensory responsiveness across modalities for this study: (1) hyporesponsiveness or hyporeactivity; (2) hyperresponsiveness or hyperreactivity; (3) sensory interests, repetitions, and seeking (SIRS) or seeking/restricted and repetitive behaviors; and (4) enhanced perception (EP; Ausderau et al., 2014; Baranek et al., 2006). Sensory hyporesponsiveness is a slow, dampened, or absent response to stimuli; sensory hyperresponsiveness is an aversive, defensive, or avoidant response to stimuli; SIRS involves intense desire for specific stimuli; and EP is a superior ability to perceive stimuli (Ausderau et al., 2014). We selected this taxonomy because of its relevance and specificity to autism and the availability of a free and well-validated tool for measuring sensory features in children with autism within the age group of our sample (Baranek, 2009).
Findings in the literature indicate that hyporesponsiveness is related to decreased social communication skills (Baranek et al., 2013), hyperresponsiveness is associated with community participation limitations (Little et al., 2015), sensory seeking is related to hyperactivity in the classroom (Nesayan et al., 2018), and EP is sometimes considered a relative strength (Mottron, 2019). Further, sensory features have been associated with earlier age at start of services but have not been examined as a predictor of amount of occupational therapy service utilization (Patten et al., 2013).
Occupational Therapy–Specific Service Utilization by Children With Autism
Few studies have explored occupational therapy service utilization separately from the utilization of other services, even when the researchers considered sensory features, adaptive behavior (McIntyre & Zemantic, 2017), and other person factors. Most studies examined demographic factors associated with overall service utilization and did not adequately examine clinical characteristics.
Analysis of occupational therapy service utilization can lend preliminary information to use in developing clinical practices and health equity policies. Occupational therapy practitioners must understand the characteristics of children with autism commonly seen in practice to inform decisions regarding evaluation, intervention, and continuing education. Developing a better understanding of the characteristics of children who do or do not receive services may help identify profiles of children who could benefit from but are not receiving occupational therapy. Furthermore, evidence regarding the amount of occupational therapy services provided to children with specific clinical presentations could offer foundational knowledge with implications for policy, access to services, and health equity. That is, an understanding of the manner in which clinical presentation (e.g., sensory features, adaptive behavior) influences service utilization can enable the profession to recognize gaps in service coverage for children with autism.
Method
Purpose and Hypotheses
We analyzed extant data to examine the extent to which sensory features, adaptive behavior, and autism severity were related to occupational therapy service utilization by children with autism, before and after adjusting for demographic variables. We hypothesized that elevated sensory hyperresponsiveness and SIRS would be particularly associated with increased occupational therapy service utilization because of the known functional impacts of these clinical factors on childhood occupations (Kanne et al., 2011; Nesayan et al., 2018). We did not develop a directional hypothesis for EP because of the limited literature and because EP may function as a strength rather than a limitation in this population (Mottron, 2019). We hypothesized that findings for hyporesponsiveness would not be significant because of its co-occurrence with SIRS (DeBoth & Reynolds, 2017) and because of its strong association with social communication deficits that are often the focus of other behavioral or speech-language therapies (Baranek et al., 2013). We included all four sensory responsiveness patterns in the analyses because they are interrelated and central to the conceptual model of the measure we used (see the Measures section).
Participants
Participants were 892 parents of children with autism ages 3 to 13 yr from 50 U.S. states (Table 1). Inclusion criteria for autism followed categories in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision), including autism, pervasive developmental disorder–not otherwise specified, and Asperger’s disorder (American Psychiatric Association, 2000). Children with genetic disorders, severe physical disabilities, sensory loss, traumatic brain injury or neurological malformations, severe mental illness, and recent seizures were excluded (Figure 1).
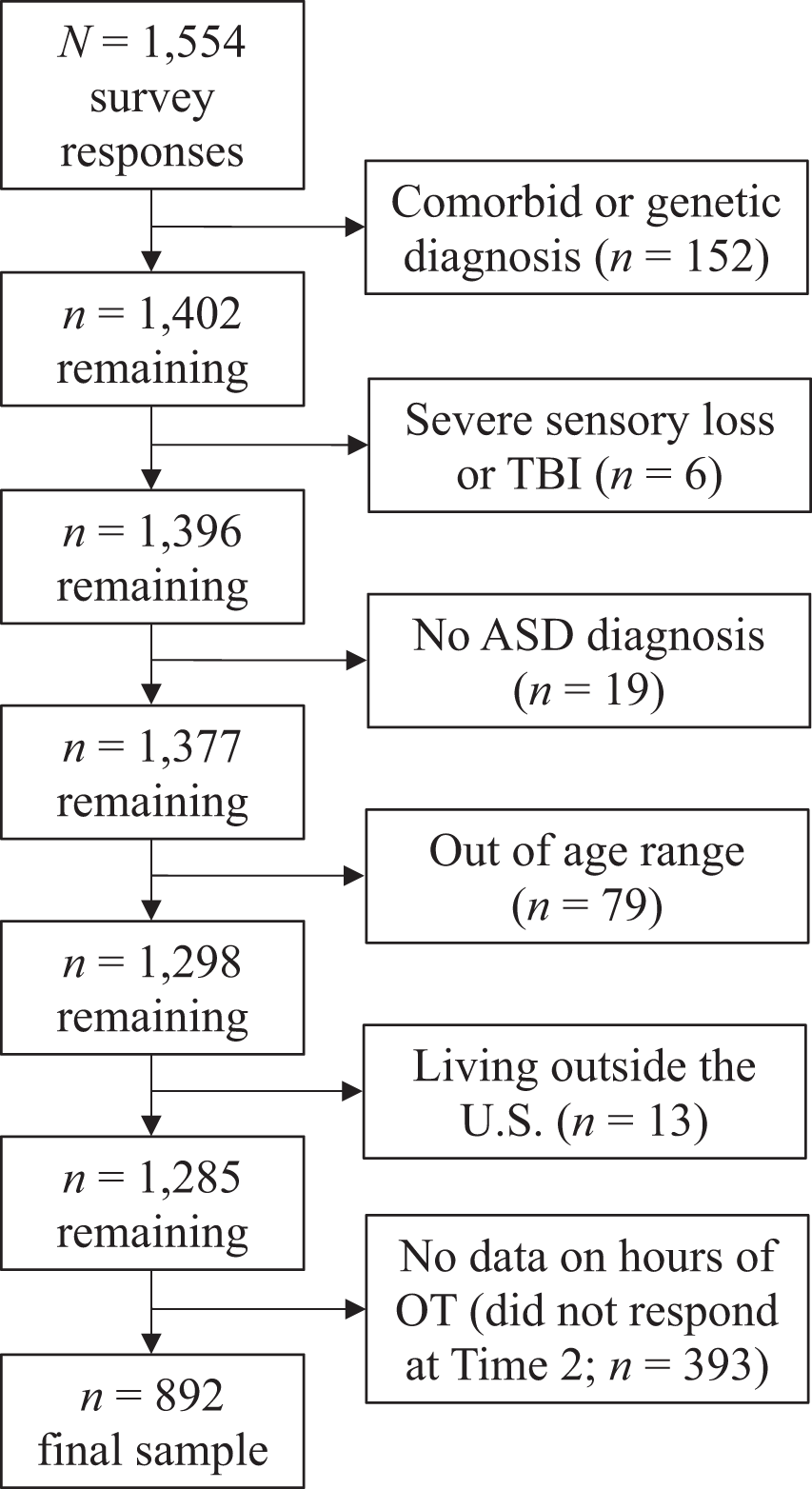
CONSORT diagram showing the flow of participants through each stage of the study.
Participant Characteristics (N = 892)
Highest education completed, transformed into years of school.
Annual income in thousands of dollars per year.
Procedures
The larger parent study that provided the data was a grant-funded national survey of families of children with autism that examined sensory subtypes and changes longitudinally (Ausderau et al., 2014). The University of North Carolina at Chapel Hill’s institutional review board approved all procedures at the time of data collection.
In the parent study, measures of demographic variables, cognitive level, and autism symptom severity were collected at Time 1. Measures of adaptive behavior and estimated weekly occupational therapy service utilization in the past year were collected 1 yr later, at Time 2. A measure of sensory features was collected at both time points; we used Time 2 sensory data because of their concurrent collection with adaptive behavior and service utilization data. Most measures were collected at only one of the two time points; our analyses are limited to the available data. Data were extracted primarily by the lead author (Emily Campi) under close supervision of the team’s data manager and its statistician (John Sideris), who was also involved in the original data processing for the parent study. Campi first created a data set of merged raw data files from the parent study; the data manager replicated the merging process to confirm accuracy. Campi then filtered out cases on the basis of the exclusion criteria and the completeness of occupational therapy service utilization data.
Measures
Autism symptom severity was measured using the Social Responsiveness Scale (SRS; Constantino & Gruber, 2005), a 65-item parent-report questionnaire that measures severity of autism traits; time to administer is 15 to 20 min. The total score was used in this analysis. This measure demonstrates concurrent validity with other measures of autism symptoms, including the Autism Quotient (r = .64, p < .001; Armstrong & Iarocci, 2013) and the Autism Diagnostic Interview–Revised (rs = .65–.74; Constantino et al., 2000).
Adaptive behavior was measured using the Vineland Adaptive Behavior Scale–Second Edition (VABS; Sparrow et al., 2005), a parent-response questionnaire that requires 30 to 45 min to complete. The VABS Adaptive Behavior Composite (ABC), used as a primary predictor in this analysis, is a single standardized score that aggregates communication, socialization, and daily living skills. We converted the ABC to standard deviation units for regression analyses by dividing the ABC standard score by 15 to examine more clinically meaningful units of change. The VABS is valid, reliable, and commonly used with children and youth with autism ages 3 to 22 yr (Kanne et al., 2011; Meyer et al., 2018; Sparrow et al., 2005).
Sensory features were measured using the Sensory Experiences Questionnaire (SEQ) Version 3.0 (Baranek, 2009), a 105-item parent-report measure of sensory features in children with autism ages 2 to 13 yr that is completed in 15 to 20 min. Sensory features are characterized in four subscales—hyporesponsiveness, hyperresponsiveness, SIRS, and EP—that have been confirmed with a valid factor structure specific to autism (Ausderau et al., 2014) and predictive utility (Ausderau et al., 2016). Mean subscale scores were used in this analysis. A previous version of the SEQ had internal consistency (α) of .80 and test–retest reliability of .92 in children with autism (Baranek et al., 2006; Little et al., 2011).
Demographic data were collected using the Background Information Questionnaire (BIQ; Time 1) and Background Information Questionnaire Updated (BIQU; Time 2), which were developed for the parent study to examine household income, race, education, sex, age, overall occupational therapy service utilization, and cognitive level (parent report from a clinician-administered test of cognitive function). The BIQU included two questions about occupational therapy service utilization: (1) “Indicate the therapies from the list that your child has received in the PAST YEAR” (list included occupational therapy) and (2) “How much time per week, on average, over the past year was spent on OCCUPATIONAL THERAPY?” Parents who did not check occupational therapy in Question 1 did not complete Question 2, and we assumed that these children received 0 hr of occupational therapy.
Data Analyses
We used IBM SPSS Statistics Version 26 to analyze the extant data set. Race was collapsed into non-White and White because only 14.6% of participants were members of minority groups. Weekly hours of occupational therapy (i.e., occupational therapy service utilization) were categorized as 0 (0.00), 1 (0.01–1.49), 2 (1.5–2.99), and 3 or more (≥3.00). We reviewed data for missingness; 9.8% of all data points on the predictor variables were missing. Percentages of missing data by key variable were as follows: 14.3% for the SRS, 9.1% for the ABC, and <5% per sensory response pattern on the SEQ. We used multiple imputation via the EM algorithm (Schafer & Graham, 2002) to create 20 data sets with imputed data for these variables. We analyzed each data set and compiled results using the SPSS missing values procedure. Patterns of results were similar in the original data set and the pooled analysis resulting from multiple imputations of predictor variables, indicating that the missing data did not meaningfully affect our findings; we report results from the pooled analysis.
A hierarchical ordinal regression model was used to predict weekly hours of occupational therapy in four steps: (1) SEQ subscale mean scores; (2) SRS total raw score and VABS ABC; (3) age, cognitive level, and sex; and (4) mother’s education level, race, and household income. We selected a hierarchical model because it allowed us to examine the most conceptually compelling and occupational therapy–relevant predictors first. We selected an ordinal regression model because weekly hours of occupational therapy were transformed into a categorical variable because of the right-skewed distribution of the original continuous variable. Results are reported using odds ratios (ORs), which indicate a child’s likelihood of a one-category increase in weekly hours of occupational therapy service utilization (e.g., 0 [0.0] hr to 1 [0.01–1.49] hr; 2 [1.5–2.99] hr to 3 [≥3.00 hr]).
Only sensory hyporesponsiveness, sensory hyperresponsiveness, SIRS, and EP subscale scores were included in Step 1 of the model because of the lack of evidence regarding the role of sensory features in service utilization and the specific expertise of occupational therapy practitioners in treating sensory features (AOTA, 2020). The SRS and VABS ABC were added to the model next because of their possible association with overall service utilization (Bilaver et al., 2016; Bilaver & Havlicek, 2019) and relevance to occupational therapy practice (AOTA, 2020), respectively. Steps 3 and 4 included demographic and nonclinical variables that have been shown to affect overall service utilization (Bilaver & Havlicek, 2019; Mire et al., 2015), separated into child characteristics (Step 3) and family characteristics (Step 4), to examine whether these known associations with overall service utilization hold true for occupational therapy service utilization.
Results
Descriptive data for clinical predictors and hours per week of occupational therapy service utilization are presented in Table 2. Results of the hierarchical ordinal regression analysis are presented in Table 3.
Descriptive Statistics for Primary Outcome Variable and Clinical Predictors
Note. VABS = Vineland Adaptive Behavior Scale–Second Edition.
As shown in Table 3, in Step 1 higher SIRS (OR = 2.20, p < .001) predicted more occupational therapy service utilization and higher EP (OR = 0.74, p < .01) predicted less occupational therapy service utilization. Sensory hyporesponsiveness and hyperresponsiveness were not significant predictors. In Step 2, SIRS (OR = 2.05, p < .001) remained significant, EP was no longer significant, and lower ABC scores (OR = 0.83, p < .01) predicted more occupational therapy service utilization.
Hierarchical Ordinal Regression Analysis
Note. VABS = Vineland Adaptive Behavior Scale–Second Edition.
Pseudo R 2 is not available for the pooled model, so we report the range of pseudo R 2s across imputations.
p < .05.
p < .01.
p < .001.
In Step 3, younger age (OR = 0.79, p < .001) and lower ABC scores (OR = 0.66, p < .001) predicted more occupational therapy service utilization, and elevated SIRS (OR = 1.35, p < .05) still predicted more occupational therapy service utilization. In Step 4, higher household income predicted more occupational therapy service utilization (OR = 1.01, p < .05); associations with SIRS (OR = 1.36, p < .05), ABC scores (OR = 0.66, p < .001), and age (OR = 0.79, p < .001) remained in the same direction as in previous steps.
Discussion
The purpose of this study was to examine clinical and demographic factors associated with occupational therapy service utilization in children with autism ages 3 to 13 yr. Children with the clinical factors of elevated sensory interests, repetitions, and seeking behaviors; lower enhanced perception; and lower adaptive behavior received more weekly hours of occupational therapy, though there was no significant effect of hyperresponsiveness, thus partially supporting our hypotheses. Consistent with previous findings on demographic factors, younger children received more weekly hours of occupational therapy (Mire et al., 2015), and higher household income predicted a slightly increased likelihood of receiving more weekly hours of occupational therapy (Bilaver et al., 2016).
Of the four sensory response patterns, SIRS was the most robust predictor of occupational therapy service utilization, even after adjusting for other clinical and demographic factors. SIRS-related behaviors have been associated with reduced community activity participation, motor skills, and academic performance in children with autism (Ashburner et al., 2008; Kirby et al., 2019; Tomchek et al., 2015), areas that are related to participation in daily occupations and within the scope of occupational therapy practice (AOTA, 2020). These functional implications may explain why our results show that higher SIRS predicts more occupational therapy–specific service utilization and thereby support increased occupational therapy service utilization by children with elevated SIRS.
The significant negative association between EP and occupational therapy service utilization (i.e., children with more enhanced perception received fewer occupational therapy services) was a new finding not previously discussed in the literature. Given evidence that higher EP is associated with increased occupational participation, better adaptive functioning, and lower symptom severity (Little et al., 2015), the result of our analysis is congruent with the idea that EP offers a protective function for this population. This explanation is supported by the lack of association between EP and occupational therapy service utilization after the addition of SRS and ABC scores, indicating that shared variance among EP, SRS, and ABC was associated with occupational therapy service utilization. Children with elevated EP may be less likely to receive occupational therapy, which is important to explore in future research. Finally, the association between adaptive behavior and occupational therapy–specific service utilization was as we expected because of the functional limitations inherent in lower levels of adaptive behavior (Kanne et al., 2011; Meyer et al., 2018).
The occupational therapy literature suggests that sensory hyporesponsiveness and hyperresponsiveness influence daily participation in children with autism (Little et al., 2015), and occupational therapy practitioners are trained in the treatment of these sensory features. However, our results show that hyporesponsiveness and hyperresponsiveness were not significantly associated with occupational therapy service utilization. Perhaps hyperresponsiveness is more easily accommodated by environmental modifications, such as availability of quiet spaces in the home or classroom, that parents and teachers can implement after informal observation and suggestions by an occupational therapy practitioner (Pfeiffer et al., 2017); more research is needed to explore this interpretation. The lack of a significant relationship between hyporesponsiveness and occupational therapy service utilization may be attributable to the lower likelihood of this sensory pattern causing disruptions during activities of daily living (Kirby et al., 2017). For example, a child who has a lack of awareness of specific sensory experiences, such as a messy face or hands (Tomchek et al., 2014), may be less likely to be referred for occupational therapy (or an increase in weekly hours) than a child who engages in disruptive behaviors in the classroom, perhaps associated with other co-occurring sensory patterns, especially SIRS.
Our findings indicate several possible issues that warrant future research. It is possible that SIRS behaviors, compared with hyporesponsiveness and hyperresponsiveness, are more apparent to teachers and parents, who also may feel less equipped to manage those behaviors without the direct support of an occupational therapy practitioner. Further, parents whose children may benefit from occupational therapy services may have limited knowledge about available services to treat autism-related sensory features (Hodgetts et al., 2015). Exploration of means of providing information to parents about available services may be needed.
The negative association between age and occupational therapy service utilization is consistent with an educational support services policy that results in decreases in overall service utilization with increasing age within the school system (Mire et al., 2015). School-based occupational therapy and speech-language services are common for the age group examined in this study, but the amount of school-based services received tends to decrease after elementary school (Mire et al., 2015). This decrease in services suggests either that older children, in general, have developed the skills they need to meet the demands of their daily lives or that there are older children who are not receiving needed occupational therapy services to manage increasing demands. Further research is needed to explore reasons for decreased services as children with autism age.
Given the existing literature on demographic factors and overall service utilization in children with autism (Bilaver & Havlicek, 2019), we anticipated that race and mother’s education level would be predictive of occupational therapy service utilization. Our finding of a lack of association, however, may be attributable to the restricted racial diversity and somewhat high average mother’s education level in the sample. More important, the significant association between lower household income and lower occupational therapy service utilization may suggest that these families experience financial barriers to accessing occupational therapy services for their children (Bilaver et al., 2016).
Limitations and Future Directions
Data for this large survey study were limited to parent reports; future studies would benefit from the additional perspectives of other informants (e.g., teachers, therapists) and observational measures of child behavior and clinical features. In addition, the study sample included parents of primarily school-age children, with underrepresentation of minority groups, so results cannot be generalized to families of other ages, races, or populations.
Future research should include more diverse participants and additional variables related to the child (e.g., interests, maladaptive behavior, motor performance), parent (e.g., stress, social supports), and payer (e.g., private pay vs. insurance). Such studies can lead to a better understanding of potential limitations of the current referral systems and policies affecting occupational therapy service utilization by children with autism. Future analyses should also include setting-specific examination of service utilization and replication in different study populations, including children with other types of intellectual and developmental disabilities, sensory processing and sensory integration difficulties, and other neurodevelopmental conditions commonly treated by occupational therapy practitioners.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice with children with autism: Occupational therapy practitioners need a strong working knowledge of SIRS and adaptive behavior concerns to evaluate their likely impact on daily participation and develop effective interventions. Practitioners need to be cognizant of the association between household income and occupational therapy service utilization and to advocate for equitable access for families with lower incomes. Practitioners should educate teachers, parents, and providers about the impacts of sensory features on behavior and participation across settings and should advocate for the role of occupational therapy in addressing these challenges.
Conclusion
This study indicates that in children with autism, higher SIRS, lower adaptive behavior, and higher household income are predictive of greater occupational therapy service utilization, even after adjusting for other demographic data, age, cognitive level, and autism symptom severity. Because of the impact of elevated SIRS and low levels of adaptive behavior on these children’s occupational performance and participation across contexts, occupational therapy practitioners are likely to be called on to intervene. Education and advocacy efforts are needed to support equitable access to occupational therapy services for families of lower socioeconomic status and children whose more subtle sensory challenges may be affecting their participation in occupations.
Footnotes
Acknowledgments
We acknowledge all faculty, staff, students, and research assistants who contributed to the collection of the extant data set used in this study and discussion of methods and findings. This study was partially supported by grant funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01HD042168).