
Abstract
This article highlights occupational therapy practitioners’ need to support electrical stimulation (ES) to address functional deficits for those with spinal cord injury. The authors identify the utility of existing clinical practice guidelines, challenges and opportunities to translate research findings into clinical practice, and desirable characteristics for an occupational therapy–specific ES clinical guide.
Electrical stimulation (ES) is used widely by occupational therapy practitioners to supplement parallel therapeutic interventions designed to improve function for clients who have experienced a spinal cord injury (SCI; Dionne et al., 2020). ES is typically deployed to improve upper extremity strength and the subsequent functional performance of activities of daily living via external stimulation to affected muscles. Few studies have investigated the effects of ES on arm and hand functional recovery in people with cervical SCI (Lu et al., 2015) and with more advanced functional ES systems (Patil et al., 2014). Owing to this fact, occupational therapy practitioners tend to rely heavily on information from interdisciplinary colleagues, manufacturer manuals, and ambiguous guidance from rehabilitation literature (Dionne et al., 2020) for the application of this modality. Despite its wide use, no unifying protocol or clinical guideline exists to support consistent ES treatments across practitioners.
Similarly, clinical research studies on ES have not used readily comparable intervention protocols, limiting our ability to synthesize findings across research studies. In addition, much of the extant research involves study designs (e.g., single-case and case series studies) yielding low levels of evidence that offer little concrete practice guidance (Dionne et al., 2020 ; Lu et al., 2015; Patil et al., 2014). Thus, the absence of a cohesive evidence-based protocol to guide consistent deployment of ES in practice and research threatens consistency of outcomes for clients and hampers researchers seeking to align their studies with common clinical practices.
The aforementioned challenges strongly suggest the need for an evidence-based, occupational therapy–specific clinical guide that would support systematic intervention practices and provide a basis for clinical research protocols on ES effectiveness. Freely accessible, appropriate, and concisely summarized evidence must be available to clinicians to appropriately use therapeutic approaches (Lin et al., 2010). To create change, innovations need to be accessible, clear, and concrete regarding expectations; they also need to achieve active engagement with the target audience (Grol et al., 2013; Lin et al., 2010; Marr, 2017). Toward that end, in this study we convened an expert panel to identify the needs of expert clinicians who actively engage in use of ES as a modality for clients with SCI.
Given the lack of a cohesive “roadmap” for practitioners and researchers to unify their approach to ES deployment, in this study we sought to identify (1) the underlying needs for clinical guidance supporting occupational therapy practitioners who use ES with the SCI population, (2) the utility of existing clinical practice guidelines (CPGs) for occupational therapy practitioners, (3) the challenges and opportunities for occupational therapy practitioners when attempting to apply findings from research studies to everyday clinical practice, and (4) key characteristics that would be desirable for a clinician-friendly guide supporting use of ES by occupational therapy practitioners working with the SCI population.
Method
Design
This study occurred in two stages. During Stage 1, a panel of geographically dispersed occupational therapy practitioners (all experts using ES with SCI populations) was convened into two discussion groups. The results from these groups were compiled and used as the basis for the draft outline of an occupational therapy–specific clinical ES manual. During Stage 2, members of the expert panel completed (1) a member-check survey in response to the qualitative summary of the Stage 1 discussions and (2) a survey in which they assigned a priority rating to each section of the proposed outline for an occupational therapy–specific clinical ES manual.
Participants
A panel of 7 experts in SCI rehabilitation was selected from a pool of ES users who had previously expressed interest in participating in future studies. All panelists were clinical leaders in their respective setting and reported frequent ES application; they also provided guidance of ES modalities to colleagues. Additionally, all panelists, at the time of the study, worked at SCI model systems centers or Commission on Accreditation of Rehabilitation Facilities (CARF)–accredited facilitates across the four regions of the United States. All panelists met the following inclusion criteria: current occupational therapy–occupational therapy assistant licensure, experience in the previous 12 mo using ES with patients having SCI in a formal treatment context, current eligibility to administer ES on the basis of their state-practice act, and current employment at a CARF-accredited or SCI model system center.
The criteria were chosen to ensure that data would reflect perspectives of clinicians regularly using ES in advanced clinical environments with access to best practices and prevailing technologies. The virtual context for the group discussions in Stage 1 necessitated that all participants have access to an internet-connected device with microphone and video capabilities. Participants received a $150 honorarium for completing the Stage 1 and Stage 2 activities.
Instruments
During the Stage 1 panel, the research team posed four questions: (1) What CPGs have you used, and what features either support or undermine clinical implementation? (2) What characteristics of research information make its clinical implementation harder or easier? (3) What key characteristics and parameters should be included in a CPG for using ES with functional activities? (4) How prescriptive and flexible would a clinical guide on ES with functional activities need to be for successful clinical implementation?
For Stage 2, two brief surveys were created. The first was a member-check survey designed to assess the degree of participant agreement with the themes and conclusions that the research team derived from the discussion transcripts (Creswell & Clark, 2017). The second survey was created to elicit priority inclusion ratings from the experts for each ES topic area that was identified in the Stage 1 group discussions.
Procedure
For Stage 1, the 7 expert panelists were scheduled into one of two 1-hr discussion groups divided into Group 1 (n = 4) and Group 2 (n = 3). In advance of the panel, participants received a consent form and discussion questions. During the groups, discussion was initiated and facilitated by the second author, whereas the first author served the roles of note taker and observer. For each question, participants were queried and given the opportunity to reflect on other participants’ responses. The sessions were audio recorded and subsequently transcribed to ensure data set accuracy. On the basis of the transcripts, themes from the discussions and priorities for CPGs for ES with the SCI population were identified. In response, the research team drafted an occupational therapy–specific clinical ES manual outline (Figure 1).
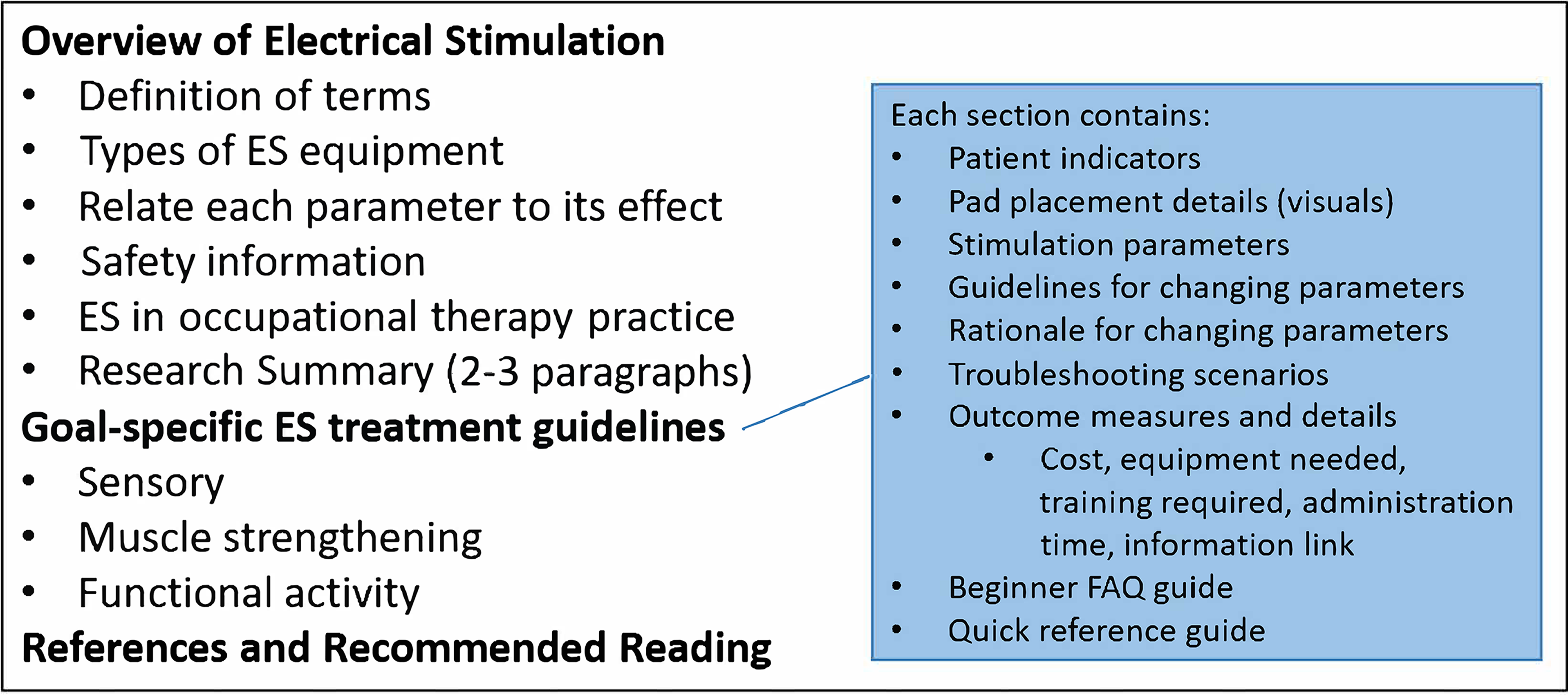
The proposed table of contents for an occupational therapy–specific clinical ES guide, on the basis of expert-panel discussions.
Stage 2 was initiated 2 wk after the Stage 1 discussion groups. Participants were sent two documents: (1) a summary of the Stage 1 discussions and (2) the outline of an occupational therapy–specific clinical ES manual (see Figure 1). Participants were asked to complete two online surveys in which they rated their level of agreement with thematic summaries of the Stage 1 discussion groups and assigned a prioritization rating for all sections of the proposed outline for the occupational therapy–specific clinical ES manual.
Data Analysis
The expert-panel recordings were transcribed by the first author and then reviewed by the second author to ensure accuracy. The first author subsequently analyzed qualitative data from the transcripts using constant comparison techniques (Creswell & Clark, 2017). During the initial coding, transcripts were examined to identify similarities and differences between data chunks. Like categorical and thematic units were grouped and summarized with the content analysis approach (Stewart & Shamdasani, 2017). All analyses were completed by the first author (Timothy P. Dionne) to maintain analytical integrity. To enhance the trustworthiness and reliability of the qualitative analysis, transcription, and thematic summary, participants completed a member-check survey (Creswell & Clark, 2017). Descriptive summaries were calculated for the member-check survey and ratings of prioritization for each area of the occupational therapy–specific clinical ES manual.
Results
Of the 7 participants, 5 worked within an inpatient SCI unit, 1 worked in an outpatient pediatric specialty clinic, and the final participant maintained a caseload of both adults and pediatric clients in an inpatient rehabilitation hospital. No other demographic information was collected to maintain anonymity, per institutional review board direction.
Stage 1: Expert-Panel Group Discussions
The group discussion covered seven topic areas: (1) usability of CPGs, (2) translation of research to practice, (3) guidance needed for occupational therapy practitioners using ES in clinical practice, (4) prescriptiveness versus flexibility, (5) use of ES to support functional activity, (6) outcome measures for ES, and (7) required characteristics of CPG for ES.
Three themes emerged from the qualitative analysis within these topic areas: (1) Published CPGs are difficult to apply in practice, (2) existing summaries of evidence for clinical deployment of ES do not readily support occupational therapy–specific interventions, and (3) clinicians often resort to ad hoc adaptation of existing intervention guidelines on the basis of personal experience and trial and error.
Theme 1: Difficulty Using Clinical Practice Guidelines for Electrical Stimulation
Participants conveyed skepticism about existing occupational therapy–specific CPGs for ES treatment: “I don’t search out OT [occupational therapy] practice guidelines. . . . I have found some PT [physical therapy] ones.” One participant described the utility of clinical pathways that include guidance on goal setting, identifying treatment steps, and updating goals: “I haven’t used clinical practice guidelines per se, but we have some documents here, more like pathways documents.” “They provide me a jumping off point,” stated the participant, which allows for clinical experience to tailor treatment approaches as necessary or needed on the basis of patient-specific goals and capabilities.
Additionally, participants worried that some CPGs for ES did not provide current information, creating concerns for safety: “I feel like what there is out there, is outdated and it’s not really staying up to date with the research, and I think that in some ways some of the guidelines could be dangerous.” Another participant responded, I would second that. I think the clinical practice guidelines, you know the PVA [Paralyzed Veterans of America], has a clinical practice guideline [Preservation of Upper Limb Function Following Spinal Cord Injury: A Clinical Practice Guideline for Health-Care Professionals; PVA, 2005] that I find totally useless [to guide occupational therapy–specific ES interventions]. They . . . come from a very traditional perspective. And while there is some good evidence-based references there . . . it becomes outdated pretty quickly.
Another participant provided a more positive perspective on the PVA guidelines, mentioning that they often use the PVA guidelines as a starting place for new graduates and as a refresher for those with more experience, adding that it provided “good baseline information.”
Specific to ES, one participant stated that they use guidelines for physical therapy intervention “specifically related to stim in stroke and stim in spinal cord or just clinical practice guidelines to treat spinal cord injury or treat stroke with upper extremity . . . but I don’t know of anything specific to OT.” Additionally, panelists reported that current guidelines can limit client progress. One participant reported frustration that novice clinicians sometimes follow ES clinical recommendations blindly without fully considering the needs and functional level for individual patients, providing an example: “[a] patient is splint[ed] for a tenodesis grasp, when they can completely recover both flexion and extension.”
Theme 2: Lack of Clinical Summaries to Guide Occupational Therapy–Specific Electrical Stimulation Treatment Activities
Participants identified several general obstacles when translating research findings into everyday clinical practice, including (1) difficulty comprehending dense procedural descriptions in journal articles, (2) clinical impracticality of idealized treatment protocols found in research studies, (3) heterogeneity of the SCI population that limits cleanly delineated sample groups, and (4) poor summaries of clinically relevant findings.
Another participant stated how difficult it was to comprehend the useful information from a research article: “[It is] hard to implement things in studies mostly because of how it’s described. I’m more of a visual learner.” One participant described that research protocols often do not readily generalize to their day-to-day practice setting: In research protocols they focus on things that clinicians may not really functionally do . . . by doing this large volume of treatment but then also getting that increase in muscle strength isn’t functional . . . what does that mean, to me, as a clinician. It’s hard to really take away a message from that.
Specific to SCI rehabilitation, one participant suggested that the heterogeneity of the SCI population in clinical practice adds an additional challenge to interpretation of research studies, which often feature narrow injury ranges: I think in spinal cord it’s also difficult because . . . they might have a mixed bag of complete versus incomplete versus how incomplete, and that can make it difficult to generalize. . . . You may not have that large of an N for your complete cases.
In regard to population-specific approaches, such as pediatric practices with day-to-day use of evidence in clinical practice, participants reported limited evidence in specific areas of practice: “So I think that’s one of the main frustrations where I’m at in pediatrics, having actual real evidence to support the statements that therapists and people are using. . . . There’s not a lot of research in pediatrics.” Expert panelists provided several suggestions to improve approachability and comprehension of research summaries, specifically visual modalities, including (1) charts (“concise summarization or charts at the end”), (2) videos (“a video . . . of a protocol [that] would help me learn and be able to implement it more than reading . . . a bunch of paragraphs in an article”), and (3) smartphone technology (“you can have the app . . . [on] phones and . . . measure range of motion through the camera” with “a picture of the upper extremity . . . and it will show somebody doing the intervention to that particular body part”).
Participants reported that determination of stimulation parameters was a major challenge for clinicians; they also suggested that an occupational therapy–specific guidance for ES should include basic ES stimulation parameters and a comprehensive explanation of the effects of each. Additionally, respondents regarded clinical decision making while using ES intervention: “People aren’t really comfortable programming . . . stim parameters and tend to overly rely on . . . pre-set programs.” The respondents continued to describe that ES parameter settings are often conveyed in a confusing manner and suggested that parameter settings be summarized according to the muscle group and expected functional response. The respondents also noted that novice clinicians are not always aware how to adjust ES parameters to ease discomfort: “They don’t know that you can actually make a change to get a better outcome . . . or based off the patient’s feedback of either it hurts, or it feels like they’re being stung by bees.”
A chart published by Martin et al. (2012) was mentioned multiple times in both discussion groups as an effective way to convey how ES parameters can be modified to optimize patient response or to troubleshoot unexpected responses: We started every patient at 20 Hz at 200 μs, and then depending on the patient’s response, were they uncomfortable? Did they demonstrate tetany? Those kinds of things. Then we adjust up or down based on the chart. That seems to be . . . more comfortable for people who don’t have much e-stim experience.
Additionally, participants suggested that visual illustrations for electrode placement would support both novice and expert users. Such visual guidance would offer a helpful starting point for new users and support more experienced users needing to experiment to achieve the desired muscle contraction from ES: “People don’t really know where to place electrodes,” a respondent stated, supporting the idea to add visuals to improve user expertise. Participants also said to include caveats with visual aids: “[Visual aids] are not the Holy Grail, it’s not the Bible of this is where it needs to go, but just a suggestion.”
Several participants discussed how inexperienced clinicians give up on using ES after an initial attempt, particularly when using ES during a functional activity: Clinicians are either going to say, “Okay, I did it wrong and I don’t really want to waste time to try it again.” Or they’re just going to say, “Well, using e-stim in this person isn’t a positive thing or an appropriate intervention.” Where in all honesty they can still use e-stim but not the functional application, putting it on a lower frequency and deeper pulse width. And still actually build the muscle health and the nerve health. So . . . then, get to actually functional electrical stimulation use.
Theme 3: Modifications of Existing Guidelines
Participants discussed the need for novice clinicians to acquire troubleshooting skills for situations in which the anticipated functional response is not achieved: “They need ‘here’s where to start’ and then what do you adjust based on what you see,” stated one respondent.
However, participants indicated that clinical guidelines for ES implementation do not need to be rigid. Rather, they should allow for flexibility by suggesting strategies for changing parameters to achieve desired functional movements: As far as activities, I don’t think it needs to be very prescriptive. I think having the general kinds of activities and how e-stim may be different. How is it different from like a weight bearing or an active reach versus like a sublux protocol?
One participant also suggested that enough information be included in a protocol to maintain safety: “I think flexibility is really important, but again you need have enough specifics to start so that you’re capturing, those who e-stim is new to, and so that they can do it safely.”
Stage 2: Member-Check Summary
After the completion of Stage 1, researchers summarized the discussion and outlined the aforementioned seven topic areas. Figure 2 illustrates panel responses to the member-check survey. In the ratings regarding accuracy of each section summary, four of the seven topic areas (i.e., using CPGs in practice, applying research to practice, prescriptiveness versus flexibility, and using ES with functional activity) received five (N = 7) or more ratings of “no changes,” with the remainder receiving “needs minor revision” or “needs major revision.” Three categories (i.e., outcome measures for ES, guidance needed for ES CPG, and characteristics of CPG for ES) had four or fewer ratings of “no changes,” with the remainder receiving “needs minor revision” or “needs major revision.” No section received a “needs complete revision” rating.
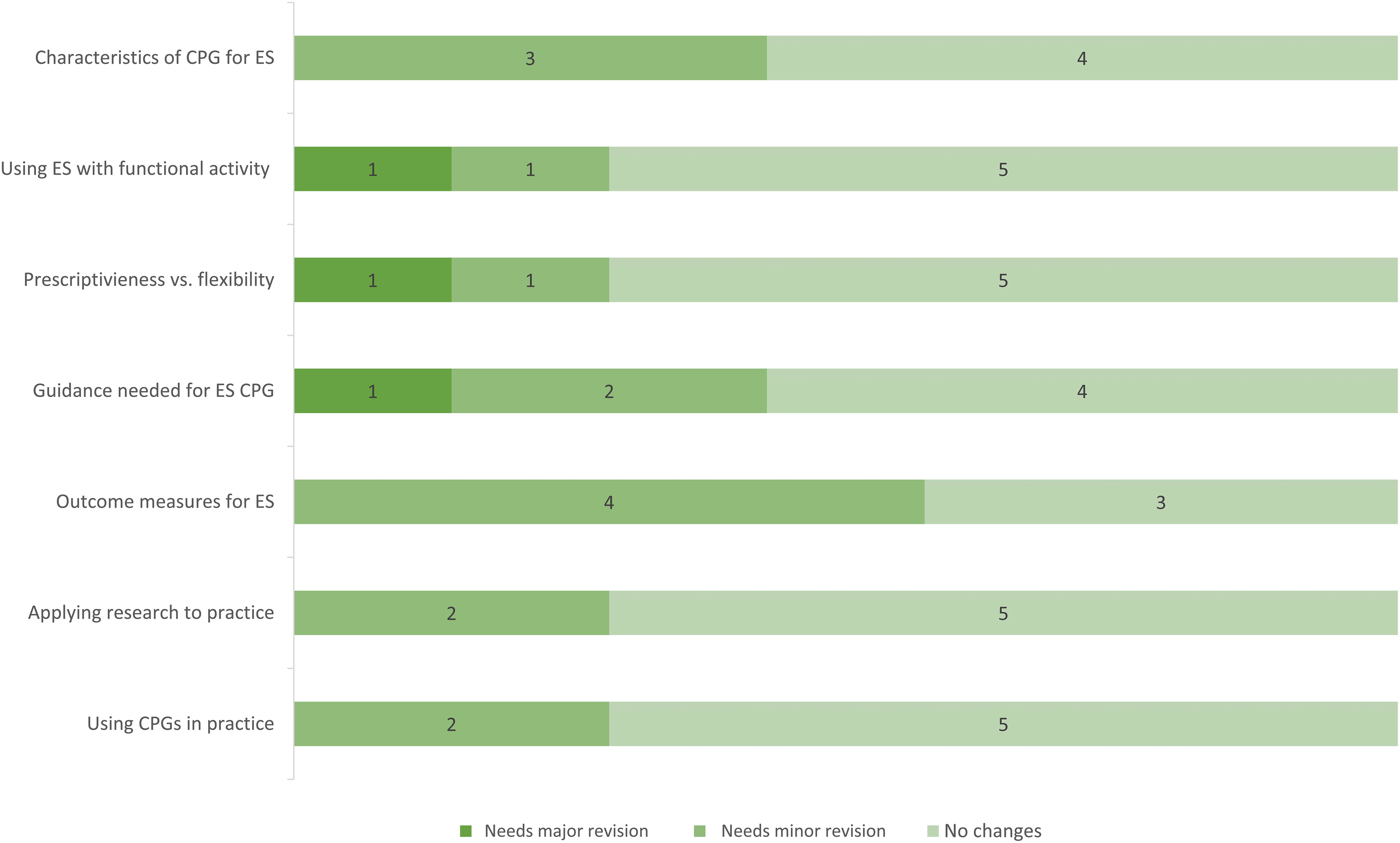
Member check: Does each theme reflect the discussion?
The participants were allowed open-text responses if they indicated revisions were needed. Notably, in reference to the “outcome measures for ES” topic area, the following qualitative responses were made: “I think the use of ES with functional activity may be broad and is a different topic than the use of e-stim so there may be some overlap there,” and “I don’t like to say ‘outcome measures for ES’ because ES is an intervention, not a goal. You would measure the functional skill, not tolerance to or participation in ES. Might consider ‘goals related to application’ or ‘functional outcome measures.’”
Additionally, during Stage 2, participants rated the importance of inclusion for each goal-specific treatment area proposed for the occupational therapy–specific clinical manual and rated the inclusions of nine subsections (Figure 3). All four goal-specific treatment areas were rated as “important” or “essential.” As illustrated in Figure 3, participants rated the importance of the nine proposed subsections to be included. Four of the proposed subsections (i.e., patient indicators, stimulation parameters, guide for changing parameters, and rationale for parameter changes) received five or more “essential” ratings. The lowest rated subsections (electrode placement, outcome measures and details) received three ratings of “somewhat important” and the remainder were rated “very important.” Figure 1 summarizes the panel’s recommendations for a clinical guide that would support deployment of ES by occupational therapy practitioners.
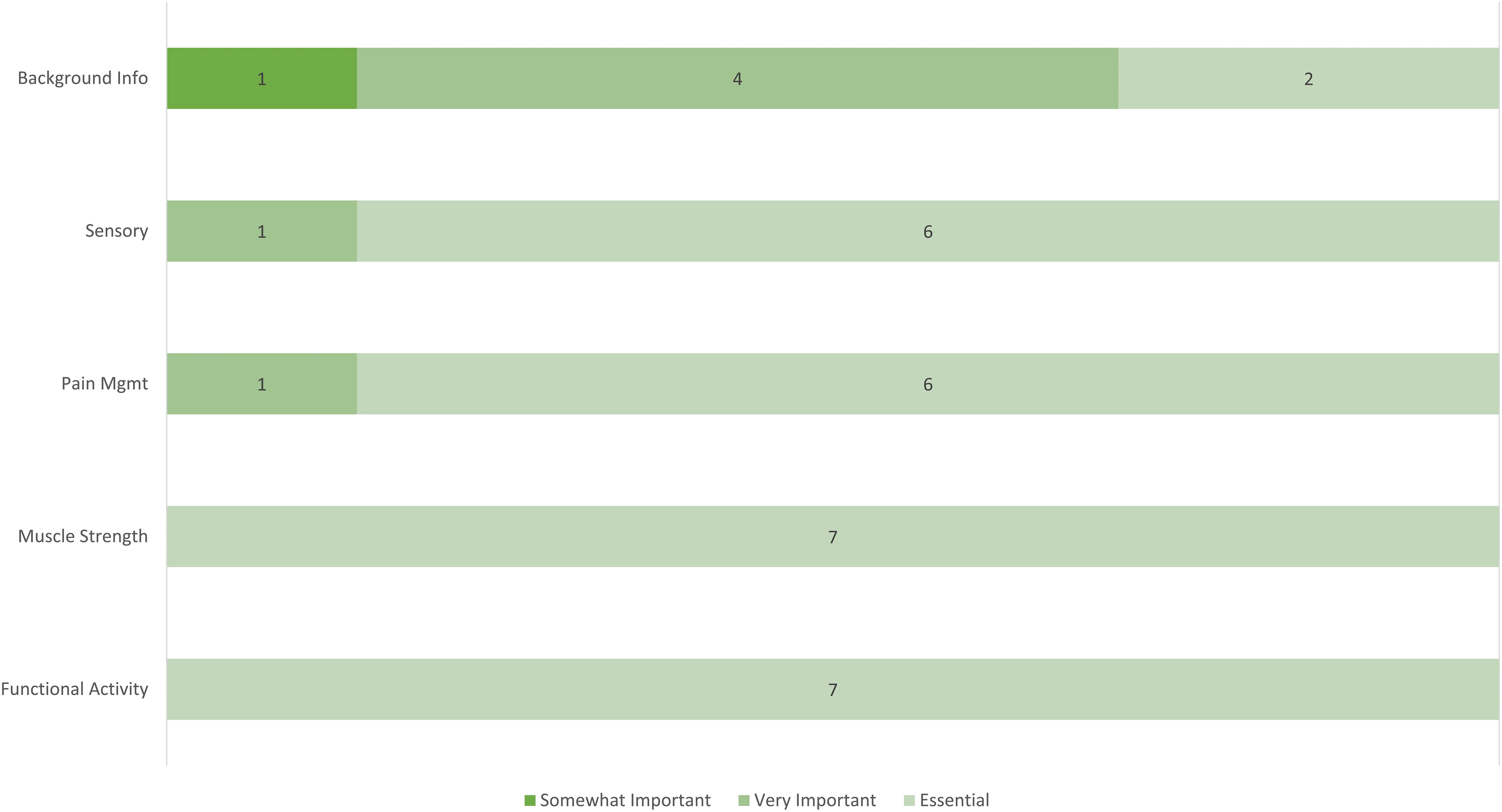
Level of importance of each goal-specific component.
Discussion
Responses from the expert panelists reinforced previous findings that clinicians are using ES while referencing a wide variety of both evidence-based and anecdotal sources for parameter selection, activities used, and clinical decision making, which undermines consistent application of ES across practitioners and settings (Dionne et al., 2020). Clinicians are lacking clear, concise, evidence-backed guidance with implementation of ES in the SCI population. Support documents exist, but the successful application of ES is hampered. Participants in this study indicated that clear and explicit clinical guidance is needed to provide confidence and consistency in the intervention’s implementation.
Concerns expressed during the panel touched on challenges of applying and using existing evidence in real-world situations. Panelists expressed difficulty justifying approaches that are used daily by clinicians when evidence appears to be limited. In the case of ES with people with SCI, the panelists recommended several key elements for a clinical guide that would support deployment of ES by occupational therapy practitioners. Specifically, the guide should offer the following features: (1) clear and concise overview of ES, including definitions of ES terms, physiological underpinnings, history of clinical use, description of current equipment and stimulation parameters, safety considerations, and literature review; (2) specific intervention guidelines that are grouped by the desired treatment goal (i.e., sensory, muscle strengthening, and functional activity); and (3) for each desired treatment effect, guidelines for patient indicators, parameter settings, details of electrode placement, conditions and rationale for modifying parameter settings, troubleshooting suggestions, outcome measures, and frequently asked questions (FAQs) for novice clinicians. The panelists also recommended creation of a one-page “quick reference guide” to provide a rapid refresher to support experienced clinicians who use ES less frequently. The resultant themes echo conclusions made by Lin et al. (2010) that translation of clinical research evidence needs to be accessible, clear, and concrete regarding expectations and allow for active engagement by clinicians.
Limitations
Participant recruitment targeted experts in this intervention modality for the SCI population; therefore, the findings reflect the innate professional biases of a highly experienced practitioner group. On the basis of the inclusion criteria, all participants would have knowledge of ES and, it can be assumed, a potential favorable view of ES effectiveness. Additionally, qualitative analysis carries inherent biases reflecting data interpretations made by investigators, which were mitigated by the inclusion of a member check.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ The expert panel reported the need for a clinician-friendly practice guide to support the use of ES as an occupational therapy treatment modality with the SCI population. The current lack of such a guide hampers the consistency with which ES is applied across occupational therapy practitioners and settings. ▪ An easily accessible and useful guide for ES implementation for occupational therapy practitioners would include (1) an overview of ES; (2) specific intervention guidelines grouped by sensory, muscle strengthening, and functional activity applications; and (3) guidelines for patient indicators, parameter settings, electrode placement, conditions and rationale for parameter settings, troubleshooting suggestions, functional outcomes measures, and FAQs for novice clinicians. ▪ Replication of an expert panel as described here could yield insights into knowledge translation needs in other specialty areas of occupational therapy practice.
Conclusion
The expert panelists identified a need for an occupational therapy–specific clinical manual to guide ES interventions by occupational therapy practitioners working with SCI populations. Such a guide would foster interventions that are more consistent across practitioners and settings, support clinical decision making, and lay the groundwork for future scientific evaluation. An example of this in action is the endeavor by the American Occupational Therapy Association (AOTA) to support and provide resources designed to improve practitioners’ access to evidence and provision of clinical guidance. Most notably, AOTA’s Knowledge Translation Toolkit (Juckett, 2022) is the primary source for this information, including a directory of systematic reviews, critically appraised topics, practice guidelines, and other evidence resources.
Support for providing relevant and accessible evidence to occupational therapy practitioners is trending. This study reinforces the need for such support. The study methods presented provide an opportunity to apply its approach in other areas of occupational therapy practice. Other specialty areas that can benefit are those with limited evidence or guidance in their application but yet are widely applied, thus affording consistent application. Ideally, features of such a manual should be readily accessible to occupational therapy practitioners and offer an approachable format that would ultimately serve the everyday practice needs of treating clinicians.
Footnotes
Acknowledgments
Timothy P. Dionne thanks the Rehabilitation Department at the University at Buffalo, School of Public Health and Health Professions, for providing internal funding for this project. We are aware that personal unconscious social, ethnic, and cultural biases might exist; despite this awareness, every attempt was made to acknowledge diverse experiences.