
Abstract
The findings of this study suggest that seating and mobility services provided by licensed rehabilitation professionals in El Salvador improve participation in occupations for people with disabilities inside and outside the home.
According to the World Health Organization (WHO; 2020), more than 65 million individuals with disabilities require a wheelchair for mobility worldwide. However, only 10% of those individuals have access to a wheelchair or other seating and mobility services (Nutaitis, 2018; WHO, 2008). Many barriers interfere with access to seating and mobility services, as well as to related education and training. Common barriers include the cost of equipment, environmental barriers, limited availability of services, and health care workers’ lack of skills and knowledge (WHO, 2020).
Wheelchairs as Mobility Devices
Functional mobility is defined as “moving from one position or place to another (during performance of everyday activities), such as in-bed mobility, wheelchair mobility, and transfers (e.g., wheelchair, bed, car, shower, tub, toilet, chair, floor); includes functional ambulation and transportation of objects” (American Occupational Therapy Association [AOTA], 2020b, p. 30). Functional mobility encompasses ambulation without assistance and moving from one place to another with the assistance of a walking aid or wheelchair. Manually powered mobility aids are classified as “walkers, crutches, canes, and braces” (Civil Rights Division, 2014, para. 10), and a wheelchair is defined as “a manually operated or power-driven device designed primarily for use by an individual with a mobility disability for the main purpose of indoor or of both indoor and outdoor locomotion” (Civil Rights Division, 2014, para. 7). For this article, we defined seating and mobility devices as equipment (wheelchairs and manually powered mobility aids) that helps to facilitate a person’s functional mobility.
The use of seating and mobility devices may improve occupational performance beyond functional mobility; prior research has demonstrated an association with improved quality of life, employment, income, function, and health indicators (Shore, 2017). According to Rousseau-Harrison et al. (2009), using a wheelchair may also improve social participation. Although there are clear benefits associated with the use of a wheelchair, few people in low- or middle-income countries have access to seating and mobility devices (WHO, 2008). Production of wheelchairs is insufficient, and related services, such as assessment of the fit of a wheelchair, are often not offered (WHO, 2020).
Short-Term Medical Missions
Short-term medical missions (STMMs) are an established model for health care professionals to serve in low- or middle-income countries where access to mobility services may be limited, combining philanthropy with patient care (Maki et al., 2008). STMMs are becoming more popular because of increased global communication, travel, and awareness of the need for health care services in lower income countries (Hawkins, 2013). Current estimates suggest that U.S.-based organizations have spent $250 million on more than 6,000 STMMs (Maki et al., 2008). However, resource allocation alone does not ensure safety and efficacy or suggest mutual benefit for individuals serving and being served. Current evidence suggests a positive impact on those who serve, especially regarding cultural sensitivity and clinical competence in the clinic (Flinn et al., 2009; Short & St. Peters, 2017; Short et al., 2020). However, a lack of standardized evaluation for those being served calls into question the impact on service recipients (Maki et al., 2008). Yet, the principles of nonmaleficence and beneficence necessitate the provision of occupational therapy services that benefit recipients (AOTA, 2020a). Although good intentions no doubt motivate STMM work, empirical research is needed to ensure that the services provided are not harmful and provide the intended benefit for recipients.
Seating and Mobility Services Provided Through Short-Term Medical Missions
Seating and mobility services provided through STMMs vary in scope and format. Service provision may include proper fitting of the device to the individual along with education or training in the use of the equipment, or it could solely involve an individual receiving a generic wheelchair without any supplemental services. Evaluating the short- and long-term holistic impact of seating and mobility services for the recipients is essential to understand their effectiveness (e.g., benefit, safety).
A study conducted by Mukherjee and Samanta (2005) found that of 162 individuals in India who had received a generic wheelchair without customization, education, or training, more than 80% had rejected the chairs because of pain, fatigue, upper limb involvement, limited adaptability to the environment, or damage. The results suggest that wheelchair distribution may have a harmful effect if wheelchairs are provided without proper assessment, customization, education, and environmental considerations (Mukherjee & Samanta, 2005). Similarly, a mixed-methods study by Visagie et al. (2015) found, on the basis of ratings on the Quebec User Evaluation of Satisfaction with Assistive Technology, that more than 60% of wheelchair recipients (n = 94) in Zimbabwe were dissatisfied with the effectiveness of their chair and felt that supportive services (e.g., education and training) were inadequate. Recipients were not consulted, and each user received limited training and information when they obtained a seating and mobility device. Shore (2017) also noted inconsistent long-term benefit for wheelchair recipients in Peru, Uganda, and Vietnam, with no significant change in individuals’ independence level, health status, or employment status over 30 mo. The findings of these studies support the essential need for proper holistic assessment, education, and training to ensure safety and effectiveness of seating and mobility services.
However, evidence also suggests that receiving mobility devices, education, and training may provide beneficial outcomes for recipients. Bazant et al. (2017) noted increased performance of activities of daily living (ADLs) and wheelchair use among wheelchair recipients (n = 852) in Kenya and the Philippines who received education and training versus those who did not. An association between increased mobility and falls was also noted, further emphasizing the need for mobility education and training (e.g., transfers, device use) for recipients, family members, and caregivers. Short (2022) also noted positive outcomes for recipients of seating and mobility devices (N = 133) in Peru who received education and training, with more than 85% agreeing or strongly agreeing that receiving the services and equipment had a positive impact on their life, functional abilities, social interaction, and sense of well-being. Prior research has suggested that seating and mobility services provided through a STMM model should be carefully planned and evaluated with an emphasis on customization of services to meet the needs of the individual and their specific environmental context. This conclusion aligns with global initiatives to standardize education and service provision for seating and mobility services (Ardianuari et al., 2022; Gartz et al., 2017 ; Kamalakannan, 2023).
Joni and Friends
Joni and Friends International Disability Center, a faith-based nonprofit with a mission to serve individuals with disabilities, collaborates with in-country partners—typically disability organizations—and supports STMMs that provide seating and mobility services in low- or middle-income countries (Joni & Friends, 2021). Although the in-country partners nurture long-standing relationships with service recipients and guide service provision, including follow-up after the STMM teams depart, licensed occupational therapists and physical therapists and support personnel or students serve alongside in-country partners to provide seating and mobility services. These services include a professional evaluation, customized mobility devices and aids, and education on and training in the proper use and care of the equipment, which is donated and refurbished in the United States. Individuals receive a holistic assessment of their physical abilities and environmental and social factors that influence their mobility needs. Mobility equipment is customized to facilitate their specific occupational priorities. For example, a tray table may be added to a wheelchair for a student to facilitate writing, or a walker may be provided for in-home functional mobility. Additionally, recipients and their families receive education on and training in the use of the equipment (e.g., transfers, navigating stairs), maintenance, and safety (e.g., pressure relief). The previous study by Short (2022) in Peru found generally positive perceptions among recipients but did not use a standardized functional outcome assessment.
By adding a standardized functional outcomes assessment, the current study aimed to address the gap in the literature by evaluating the benefits for individuals with disabilities of customized seating and mobility services that include education and training on in-home and out-of-home occupational participation. We incorporated the original survey completed by Short (2022), modified for Spanish speakers in El Salvador, and Part 1 Wheelchair Outcome Measure (Miller, 2004), professionally translated to Spanish, for standardized functional outcome data. Thus, we examined perceptions of receiving seating and mobility services of individuals with disabilities in El Salvador and analyzed the impact on preferred occupations using the standardized WhOM.
Hypotheses
The following hypotheses were tested by using inferential statistics to analyze pretest and posttest scores on the WhOM: H1: Receiving seating and mobility equipment, education, and training will demonstrate a statistically significant increase in satisfaction ratings for in-home occupations. H0: Receiving seating and mobility equipment, education, and training will not demonstrate a statistically significant increase in satisfaction ratings for in-home occupations. H2: Receiving seating and mobility equipment, education, and training will demonstrate a statistically significant increase in satisfaction ratings for out-of-home occupations. H0: Receiving seating and mobility equipment, education, and training will not demonstrate a statistically significant increase in satisfaction ratings for out-of-home occupations.
Method
Research Design
A one-group retrospective pretest–posttest (RPP) design was implemented using a survey that aligned with the Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; AOTA, 2020b) categories of occupational performance for individuals who had received seating and mobility services between January 2017 and March 2022. In addition, the WhOM was administered to wheelchair recipients who had received a wheelchair in the past 5 yr. The RPP design has been advocated as a viable alternative to a traditional pretest–posttest (TPP) design, specifically when measuring perceptual constructs when time has elapsed from the initial intervention and a TPP design may not be feasible. Reflecting on current and prior perceptions at the same point in time may limit response shift bias, a change in the internal frame of reference about the construct being measured between the pretest and posttest. Additionally, RPP study designs demonstrate sensitivity to change and have been used for numerous federally funded research studies (Little et al., 2020).
Participants
Individuals with disabilities from El Salvador who had received seating and mobility services through an STMM model within the past 5 yr through a collaborative effort between Fundacion Venciendo Barreras and Joni and Friends International Disability Center were recruited by phone and email for participation in the study. All age demographics were included, and for those younger than age 18 yr, a parent or caregiver completed the survey and WhOM. Individuals who had not received seating and mobility services or who had received services >5 yr before study implementation were excluded from the study.
Instrumentation
The survey implemented by Short (2022), based on the occupations outlined and defined in the OTPF–4 with peer review to enhance face validity, was implemented in this current study to examine the perceived impact of receiving seating and mobility services on various areas of occupational performance. The survey was constructed in SurveyMonkey and translated into Spanish before dissemination. It included open-ended questions related to the participant’s individual experience and feedback to improve service provision. In addition, the survey elicited demographic information and Likert-scale ratings of the impact of seating and mobility services on a variety of occupations. The survey was peer reviewed and revised on the basis of feedback from occupational therapy faculty with expertise in the field to ensure clarity and comprehensible delivery.
The WhOM is a two-part semistructured interview that analyzes the importance of and satisfaction with self-reported activities in and out of the home, comfort, body position, skin breakdown, and skin integrity to identify desired outcomes (Alimohammad et al., 2016 ; Miller, 2004). Only Part 1 of the WhOM, in which participants rate the importance of and satisfaction with various reported activities on a 10-point Likert scale, was used for participants who received a wheelchair. Psychometric data reveal high test–retest reliability (WhOM Satisfaction intraclass correlation coefficient [ICC] = .90; WhOM Satisfaction × Importance = .93; WhOM Body Function ICC = .83), interrater reliability (ICC = .99), and agreement between raters for identified participation outcomes (κ > .71; Alimohammad et al., 2016; Garden, 2009).
Procedures
With university institutional review board approval, the survey was peer reviewed and revised before translation to Spanish. The survey and WhOM were translated from English to Spanish using forward–backward translation (Degroot et al., 1994), following a protocol similar to that for other non-English translations of the WhOM. A professional translator in El Salvador translated them from English to Spanish, and a second professional translator in El Salvador translated them back to English. The two translators then discussed and revised any discrepancies for clarity. In-country El Salvadoran Spanish speakers were hired as research assistants and trained to administer the survey and WhOM.
All those who had received a seating and mobility device in the past 5 yr received an invitation to participate and a link to the survey through email, telephone, text message, and social media. Those who did not have an internet connection or telephone service were administered the survey in person.
The end of the survey requested that individuals who had received a wheelchair participate in the WhOM by providing their consent and a telephone number. Participants who had received a wheelchair but did not complete the survey were also contacted by personnel from Fundacion Venciendo Barreras to participate in the WhOM assessment. The research assistants then administered Part 1 of the WhOM by phone or in person to those who volunteered to participate. Participants were asked to identify their preferred functional activities inside and outside the home, and they rated their satisfaction with completing these activities before and after receiving a wheelchair. Research assistants read both the survey and the WhOM to participants who were unable to read.
WhOM data were recorded in hard copy, translated to English, scanned, and emailed securely to the primary investigator (Nathan Short), and the original hard copies were shredded upon completion of the study. Survey and WhOM data were kept in password-protected files, and no identifying information was collected or stored. The pretest and posttest reports were analyzed to understand the impact on the participants of receiving a wheelchair with education and training.
Data Analysis
Descriptive statistics for demographics and responses to questions about the impact of receiving seating and mobility services were analyzed and compared on the basis of the participants’ sex, age, and type of mobility equipment and devices received (e.g., walker, crutches, wheelchair). Quantitative analysis involved descriptive and inferential statistics to analyze data from the survey and WhOM. The average change in mean was calculated for the total in-home and out-of-home responses, and individual occupations were grouped. Applying a concept-driven approach based on language in the OTPF–4, we met as a team to analyze each activity the participants reported on the WhOM and categorized the activities into areas of occupation. The team deliberated until 100% consensus was reached. A paired two-sample t test (one-tailed p < .05) was used to analyze statistical significance, and Cohen’s d (<0.01 = very small; 0.01–0.2 = small; 0.2–0.5 = medium, 0.5–0.8 = large, 0.8–1.2 = very large; >2.0 = huge) was used to analyze effect size for pretest and posttest satisfaction scores on the WhOM (Sawilowsky, 2009).
Results
The survey sample (n = 49) included 25 women and 23 men with a median age of 28 yr (range = 3–103 yr). The survey had fewer respondents than the WhOM (n = 86); the survey was administered via email, with a 57% response rate, and the WhOM was administered in person or by phone to 100% of the participants contacted.
Survey
Of the survey recipients (n = 49), 44% responded directly, and parents (38%), caregivers (17%), or siblings (2%) responded on behalf of the other recipients. All participants had received a wheelchair, and 2 also received a cane. More than 86% of respondents answered agree or strongly agree to the questions assessing the perceived impact of receiving mobility equipment on performance of ADLs, social interaction, community mobility, and sense of well-being. Figure 1 displays the responses to the question of whether receiving services had a positive impact on the recipient’s life and is representative of the generally positive trend for responses to other questions related to areas of occupational performance. Survey questions regarding the perceived impact on work and attending school did not follow the same trend; more than 45% of respondents indicated that the question did not apply to them.
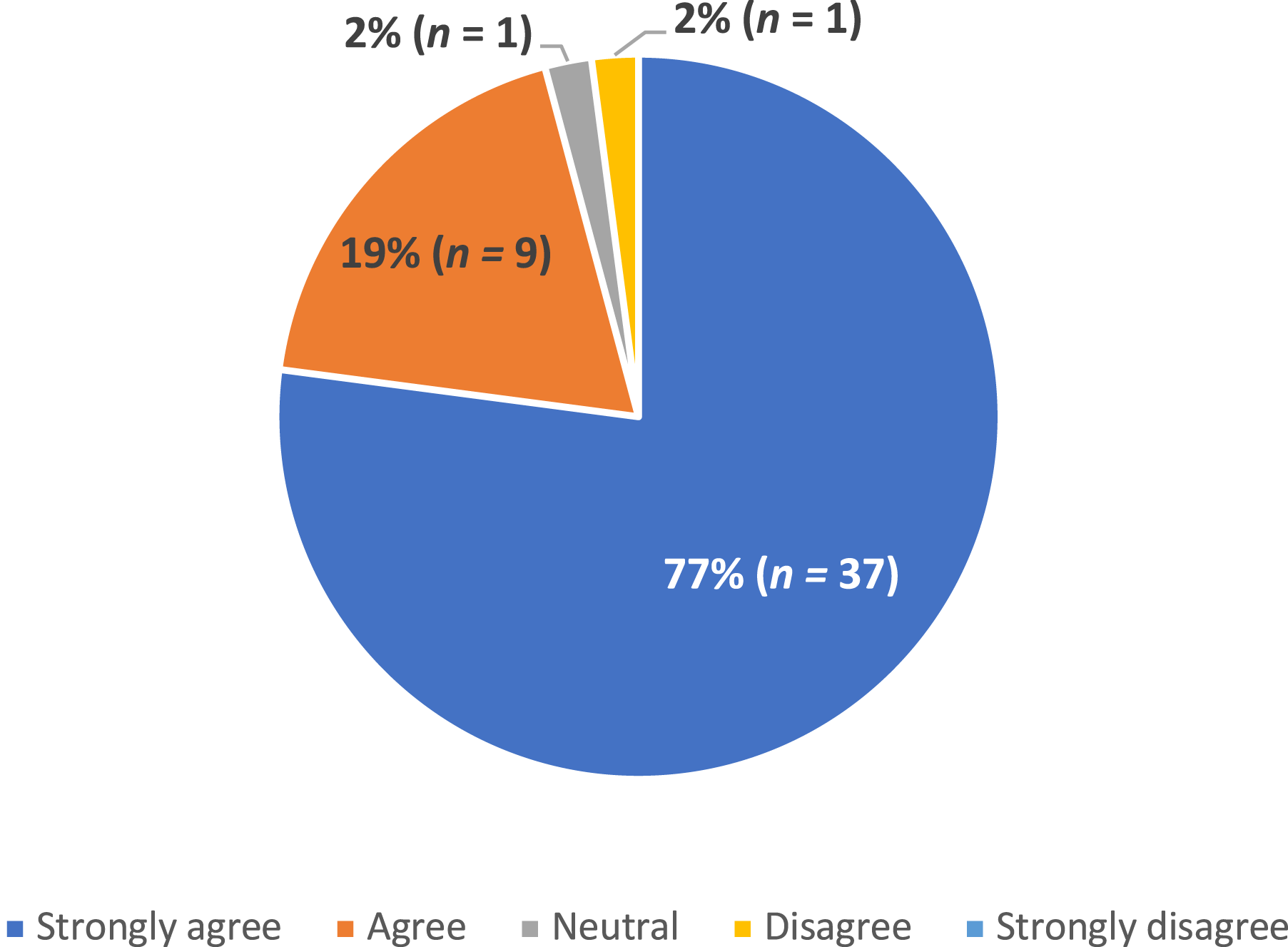
Responses to the questions of whether receiving mobility equipment, education, or training had a positive impact on the participants’ life (N = 49).
Wheelchair Outcome Measure
Participant (n = 86) demographics were similar to those of survey participants, and they reported participation in 29 distinct functional activities representing all occupation categories noted in the OTPF–4 (i.e., ADLs, instrumental activities of daily living [IADLs], health management, rest and sleep, education, work, leisure, play, social participation). Participants reported 18 distinct in-home occupations, such as watching television (n = 59), functional mobility (n = 47), home management (n = 42), meal preparation (n = 39), and eating (n = 38), and they reported 11 distinct out-of-home occupations, such as visiting family (n = 67), going to doctor or therapy appointments (n = 65), attending church (n = 50), shopping (n = 40), and going to the park (n = 22). Several participants reported improvement in occupations related to their role performance as a student (n = 20), worker (n = 12), or parent (n = 3). Of note, participants scored 82 occupations, nearly 10% of all functional activities rated, as 0 on the pretest, suggesting a complete inability to participate in the desired occupation before receiving services.
Mean satisfaction scores for performance of in-home occupations after receiving seating and mobility services increased by 5.42 points (n = 86; p < .05), and mean satisfaction scores for performance of out-of-home occupations increased by 7.17 points (n = 76; p < .05; Table 1). Psychometric testing of WhOM results suggested a clinically meaningful change with a minimum of a 2-point difference between pretest and posttest satisfaction scores (Miller, 2004). We found a huge effect size for ratings regarding performance of both in-home (d = 5.67) and out-of-home (d = 6.46) occupations.
Pretest and Posttest Wheelchair Outcome Measure Satisfaction Ratings for In-Home and Out-of-Home Occupations
Statistically significant mean differences appeared for all subcategories of occupational performance. The change in mean between pretest and posttest scores for out-of-home occupations trended higher than that for in-home occupations, with leisure and work demonstrating the most significant increase in mean ratings (Table 2).
Difference in Mean Scores for Subcategories of Occupational Performance
Note. ADLs = activities of daily living; IADLs = instrumental activities of daily living; N/A = not applicable.
Discussion
The purpose of this study was to analyze the perceived impact of seating and mobility services, education, and training for individuals with disabilities in El Salvador by means of a survey and standardized WhOM assessment. Recipients reported largely positive perceptions of the impact on occupational performance on the survey. This finding was confirmed by statistically significant improvement in the pre- and posttest satisfaction ratings on the WhOM for both in-home (p < .05; d = 5.67) and out-of-home (p < .05; d = 6.46) occupations, leading us to reject the null hypotheses. The findings provide robust support for seating and mobility services, delivered by licensed rehabilitation professionals through an STMM model that included education and training and in partnership with local organizations, as beneficial for individuals with disabilities in El Salvador with respect to satisfaction in the performance of both in-home and out-of-home occupations.
The survey assessed categories of occupations and asked participants to rate the impact of the services on specific occupations. Overall, we found that seating and mobility services improved recipients’ ability to complete everyday activities, such as traveling around their community, socializing with friends and family, and attending church or other community events. However, responses to questions in the categories of work and education indicated that more than 45% of respondents indicated that these questions did not apply to them. Although limited functional mobility may present a challenge to employment or education, many other factors contribute, and this finding warrants further examination regarding barriers to participation in these occupations for individuals with disabilities in El Salvador.
The pretest and posttest WhOM responses demonstrated a statistically significant (p < .0.5) change with a huge effect size (d ≥ 2), notably with Cohen’s d values above 4.0 for both in-home and out-of-home occupations. Although having an effect size >1 may seem improbable, a huge effect size is possible. Cohen himself encouraged flexibility in interpreting effect size using his eponymous statistical test, and recent research has called for a reexamination and expansion of these suggested values with additional categories added for values >1 (Sawilowsky, 2009). The unusually large effect size is encouraging, but we also recognize this atypical finding as a point of discussion.
The lead author (Nathan Short) trained the data collectors, who were Spanish-speaking El Salvadorans, and observed them as they completed several WhOM assessments and noted minimal deviation from the script outlined in the WhOM assessment. Furthermore, no cues or suggestions were given that might have affected the participants’ responses. However, the participants chose the occupations that were most important to them, both in and out of home, which may have contributed to a tendency to report occupations that were most improved. Additionally, participants rated 82 occupations as a “0” for satisfaction before receiving services, suggesting that they may have been entirely unable to perform these daily activities. Many of these occupations were out-of-home activities and involved community mobility, for example, attending medical appointments (n = 65), visiting family (n = 67), or attending church (n = 50). This may have been a factor in the large effect size because receiving seating and mobility services not only improved but also restored participants’ ability to leave their homes and engage in community activities.
Additionally, some participants may have received a wheelchair and related education and training for the first time, contributing to a positive perception regarding the performance of occupations. Although anecdotal, the lead author has witnessed adolescents in low- or middle-income countries being carried by a caregiver or older adults being pushed in a wheelbarrow for functional mobility. Transitioning from this caregiver-dependent scenario to a customized seating system may well have created the level of perceived satisfaction in occupational performance reflected by participants in this study, although more research is recommended to confirm this finding.
The significance levels and effect size were consistent with pre- and posttest WhOM scores when analyzed by specific areas of occupation. It is notable that ADLs reflected the greatest difference in pre- and posttest mean scores for in-home occupations (M = 5.66), including eating, moving around the home, dressing, and bathing. This higher score may reflect a general lack of in-home mobility before receiving services or the participants’ using the mobility device primarily in the home. Regarding out-of-home occupations, IADLs demonstrated the largest difference in mean between pre- and posttest WhOM scores (M = 6.20). Activities included in this category were going to the doctor, going to church, shopping, and going to therapy. Out-of-home pretest scores trended lower than in-home pretest scores, suggesting that participants were more limited in participation in out-of-home occupations before receiving services. The lack of a customized seating system may have been most limiting for occupations involving community mobility, for example, going to the beach or a park, forms of leisure that demonstrated the most significant change in mean for out-of-home occupations.
Prior research has effectively outlined the need for wheelchairs worldwide because of the millions of individuals with disabilities without access to mobility devices (Nutaitis, 2018; WHO, 2008). Although access to in-country services varies, STMMs provide one avenue for the provision of seating and mobility services in low- and middle-income countries. However, researchers have questioned the benefit of these STMMs because of the lack of standardized outcome measures to evaluate the impact of receiving seating and mobility services (Maki et al., 2008). The current study incorporated a standardized assessment, addressing the limitation emphasized by Maki et al. (2008) and filling a gap in the literature. A previous study by Visagie et al. (2015) analyzed wheelchair users’ (N = 94) satisfaction with seating and mobility services provided in a clinic in Zimbabwe. These recipients received a basic folding or nonfolding wheelchair supplied by rehabilitation technicians, wheelchair technicians, and therapists (Visagie et al., 2015). More than 60% of the participants expressed dissatisfaction with the wheelchair’s durability, weight, ease of adjustment, effectiveness, safety, reliability, and whether it met users’ needs (Visagie et al., 2015). The recipients in the current study received not only effective mobility equipment provided by licensed rehabilitation professionals but also proper fitting and education. It is encouraging that the sample included individuals who had received services from 1 to 5 yr before the implementation of the study, suggesting short- and long-term improvement in occupational performance.
Wheelchair and mobility devices allow an individual to participate in meaningful activities. The improved satisfaction levels indicated by the WhOM results and overall positive trends in the survey data demonstrate that an effective mobility device improves participation in occupations and general well-being and quality of life. Multiple studies have supported the positive perceived impact of STMMs on service providers and students (Flinn et al., 2009; Short & St. Peters, 2017; Short et al., 2020), and the current study supports their positive perceived impact on recipients. In comparison with prior related literature, the high-quality provision of services, education, and training should be emphasized to optimize outcomes, and efforts should be made to standardize service provision to align with global health care trends. Similar endeavors should consider knowledge and skills testing for providers and standardized education and training to ensure safe and effective service provision (Ardianuari et al., 2022; Gartz et al., 2017 ; Kamalakannan, 2023).
When working cross-culturally, cultural humility, with an emphasis on self-awareness and addressing power imbalances, is paramount to contribute to positive, collaborative outcomes (Foronda et al., 2016). To that end, we intentionally recruited professionals from El Salvador who were familiar with the target population to review and revise the survey, translate the WhOM, and lead the interaction with and data collection from participants. After reviewing many standardized measures related to seating and mobility, we chose the WhOM as the most occupation-based and potentially culturally relevant because participants select the occupations that are most meaningful to them, as opposed to rating predetermined occupations that may reflect a cultural bias. Furthermore, the survey and WhOM intentionally focused on satisfaction with performance of selected occupations versus independence, often an underlying emphasis on assessments developed in more individualistic Western cultures. Although these practical steps may have limited inherent cultural bias and paternalism, we recognize that the development of cultural humility is an ongoing process and encourage further reflection and feedback from in-country partners for future work.
Limitations
The study was conducted during the COVID-19 pandemic with ongoing mask and social distancing requirements and prior lockdowns that likely affected participants’ performance patterns and perceptions regarding use of their mobility equipment during their daily life. Additionally, the data were translated from Spanish to English, potentially affecting the interpretation of the participants’ responses. While completing the WhOM, participants were asked to recall their satisfaction before receiving seating and mobility services, and their perceptions may not reflect how they actually felt at that time. Approximately half of respondents participated in the survey portion of the study, so a response bias may be present in the survey data. Last, some survey and WhOM responses were provided by caregivers, whose representations of the participants’ perceptions were subjective.
Directions for Future Research
Future studies should continue to integrate well-researched, standardized assessments for improved validity and reliability. Additional work should also explore the perceived impact of seating and mobility services in other countries and regions of the world to assess similarities and differences in responses among recipients. It is recommended that future research further investigate the impact of seating and mobility services on education and work participation. It is also important to note that each STMM is unique, and researchers should independently analyze each endeavor.
Implications for Occupational Therapy Practice
The use of STMMs to provide seating and mobility services in low- or middle-income countries may be an effective service delivery model to improve occupational performance. Customized seating systems along with supportive education and training should be provided by licensed occupational therapists or other rehabilitation professionals through collaboration with in-country partners. These findings are specific to seating and mobility and should not be generalized to other areas of practice.
Conclusion
The results suggest that seating and mobility services guided by an in-country partner and provided by licensed rehabilitation professionals through an STMM model can have a positive impact on individuals’ participation in in-home and out-of-home occupations.
Footnotes
Acknowledgments
First, we acknowledge our study participants—thank you for advocating for people with disabilities worldwide by sharing your lived experience with us. Sincere appreciation to our partners at Joni and Friends for their support and warm hospitality: Kimi Archer, MSPT, Director of Internships; Claudia Aguirre, International Regional Manager for Central America; and Monica Aguirre, Director of Joni’s House (El Salvador). We also acknowledge our research assistants— Sergio Valle, Arlyn Urbina-Pino, and Jennifer Flores of Fundacion Venciendo Barreras—who were essential to data collection and translation.