
Abstract
This systematic review demonstrates that constraint-induced movement therapy (CIMT) is an effective intervention when compared with other therapeutic approaches and can be used by occupational therapy practitioners who work alongside children diagnosed with hemiparesis associated with cerebral palsy (CP).
Cerebral palsy (CP) is a neurodevelopmental motor impairment caused by nonprogressive lesions in the developing brain (Taub et al., 2004). Clinically, disorders of movement seen in children with CP are distinguished and defined by the location of the lesion, extremity affected (i.e., hemiplegia, diplegia, quadriplegia), clinical judgments of muscle tone, and presence of involuntary movement (i.e., spasticity, ataxia, athetosis; Nahar et al., 2015). The amount and degree of muscle tone, abnormal movement, and body part affected vary widely based on the location of the lesion. Depending upon the severity of the diagnosis, the limbs affected, and the degree of muscle tone, children who have CP may use different strategies and techniques to perform daily tasks (Nahar et al., 2015). A common type of CP involves spasticity in the affected extremities. The spasticity may be mild, allowing some movement, or severe such that no or limited movement is possible. Upper extremity function may be reduced as a result of sensory abnormalities, weak grip, loss of fine motor skills, impaired speed of movement, and the degree of spasticity (Nahar et al., 2015). This can potentially limit a child’s ability to participate in occupations.
Increasing functional use of the affected upper extremity in children with CP has been the focus of intervention. Constraint-induced movement therapy (CIMT), also known as constraint-induced therapy (CIT), is an intervention that was created by combining ideas from behavioral psychology, learning, and neuroplasticity. It was derived from fundamental experimental psychology research with nonhuman primates conducted by Taub and colleagues (Rostami & Malamiri, 2012; Taub et al., 1994). There are three components of CIMT: (1) constraining the nonaffected arm, (2) performing repetitive and intensive motor activities with the more affected arm, and (3) shaping functional movements of that affected arm (Rostami & Malamiri, 2012). Taub et al. (1994) successfully increased function of the affected upper extremity using CIMT with adults poststroke. On the basis of these results, they hypothesized that children with hemiplegic CP could also benefit from this approach to improve the use of the impaired upper extremity (Taub et al., 2004).
The aim of this review is to determine whether CIMT is more effective than other approaches in improving upper extremity function of children diagnosed with hemiparesis-associated CP. In addition, this systematic review aims to advance the knowledge of the effectiveness of CIMT for occupational therapy practitioners and students by accumulating research performed over the past 20 yr.
Method
This review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and followed the Cochrane Collaboration methodology (Higgins et al., 2019; Moher et al., 2009).
Literature searches were conducted independently by the authors to gain a comprehensive overview of the studies published related to using forms of CIMT for children with hemiparesis associated with CP. Inclusion criteria for the review were (1) a primary diagnosis of hemiparesis associated with CP; (2) participants younger than 21 yr of age; (3) CIT, CIMT, or other modified forms of CIMT offered as an intervention; and (4) containing at least one group in the study. Exclusion criteria were articles not in English, case reports or single-subject research designs, or other diagnoses as the primary focus of the intervention (Figure 1). Literature search results were collected, duplicates were removed, and the results were exported. The authors independently screened titles and abstracts resulting from the search. The authors then compared their decisions to include or exclude. When differences appeared, they were resolved by discussion until a consensus was reached.
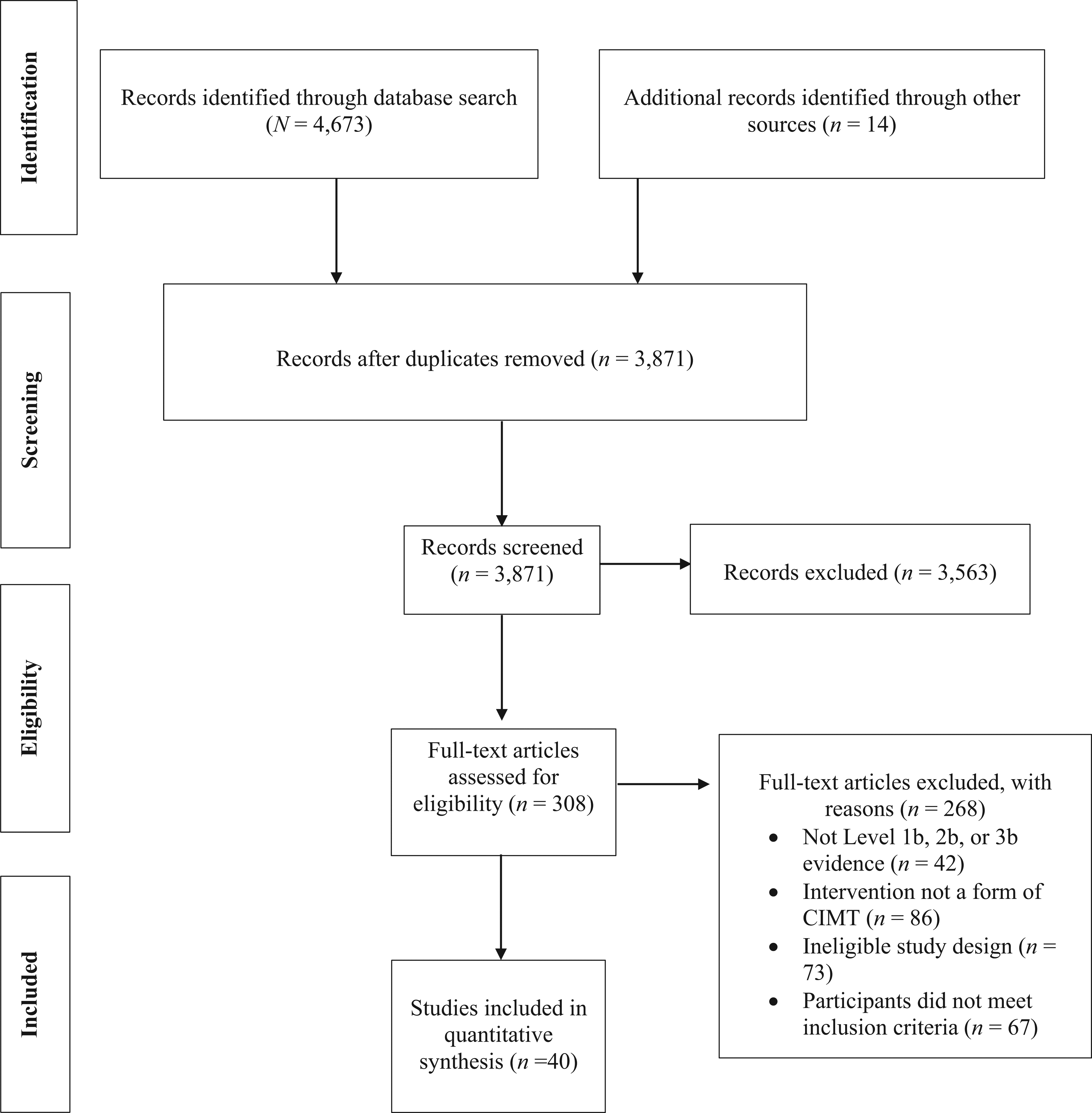
Flow diagram for inclusion and exclusion of studies in the systematic review.
Databases used in the search were the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Health Source: Nursing/Academic Edition, PsycINFO, PubMed, Research Gate, and Google Scholar. Keywords included occupational therapy, CIMT, CIT, constraint induced movement therapy, cerebral palsy, pediatrics, and children. There were 4,687 articles initially identified. Articles from more than 10 yr ago were included to show the progression of research on the implementation of CIMT. Articles’ publication dates ranged from 2001 to 2018, with a majority of the research conducted from 2011 to 2018.
Risk of bias was evaluated using the Cochrane tool depending on the study design (Higgins et al., 2016). Studies that were included in this review provided Level 1b, 2b, and 3b evidence. This information is included in Table A.1 of the Supplemental Appendix (available online with this article at https://research.aota.org/ajot). Classification for level of evidence was determined by using the Oxford Centre for Evidence-Based Medicine (2009): Level 1b: well-designed individual randomized controlled trial (RCT) Level 2b: prospective cohort studies; ecological studies; and two-group, low-quality RCT and nonrandomized studies Level 3b: individual retrospective case–control studies, one-group, nonrandomized pretest–posttest studies, and cohort studies.
The U.S. Preventive Services Task Force (2018) recommendations were used in addition to the risk-of-bias results, number of studies, and level of evidence to describe the strength of evidence for our findings:
Strong: Two or more Level 1a or 1b studies. The available evidence usually includes consistent results from well-designed and well-conducted studies. The findings are unlikely to be called into question by the results of future studies.
Moderate: At least one Level 1a or 1b high-quality study or multiple moderate-quality studies such as Level 2a/2b or Level 3a/3b. The available evidence is sufficient to determine the effects on health outcomes, but confidence in the estimate is affected by the number, size, quality, or inconsistency across individual studies. The findings may be questioned in the future.
Low: Small number of low-level studies, flaws in the studies, or both. The available evidence is insufficient to assess effects on health outcomes. Evidence is insufficient because of the limited number or size of studies, inconsistency of findings across individual studies, or lack of information on health outcomes.
Results
Forty studies that met the inclusion criteria were identified for this systematic review. The results describe the ages of children who were included in the studies and provide a comparison of the outcomes of the types of CIMT versus the comparison group when appropriate. Table A.1 of the Supplemental Appendix summarizes the research design, characteristics of the participants, the outcome measures, the intervention methods, and the results of the included studies.
Ages of Children in the Studies
In this review, 15 studies had participants with a mean age of 0 to 5 yr (Al-Oraibi & Eliasson, 2011; Case-Smith et al., 2012; Chamudot et al., 2018; DeLuca et al., 2006, 2012, 2017; Eliasson et al., 2005, 2011, 2018; Gelkop et al., 2015; Naylor & Bower, 2005; Smania et al., 2009; Sung et al., 2005; Taub et al., 2004; Wallen et al., 2011); 14 studies had participants with a mean age of 5 to 10 yr (Charles et al., 2006; Chen et al., 2013; de Brito Brandão et al., 2010, 2012; Friel et al., 2021; Gordon et al., 2011; Hung et al., 2020; Klingels et al., 2013; Nahar et al., 2015; Reidy et al., 2012; Rostami & Malamiri, 2012; Sakzewski et al., 2015; Simon-Martinez et al., 2020; Stearns et al., 2009); and 11 studies had participants with a mean age of more than 10 yr (Bonnier et al., 2006; Charles et al., 2001; Dong et al., 2017; Eliasson et al., 2009; Gillick et al., 2018; Gordon et al., 2007; Sakzewski et al., 2012; Sakzewski, Ziviani, Abbott, et al., 2011a, 2011b, 2011c; Sakzewski, Zivinia, & Boyd, 2011).
Intensity of Constraint-Induced Movement Therapy
CIMT was most commonly implemented for 6 hr per day for anywhere from 10 to 21 consecutive days in 18 of the studies (Case-Smith et al., 2012; Charles et al., 2001, 2006; de Brito Brandão et al., 2012; DeLuca et al., 2006, 2012, 2017; Friel et al., 2021; Gordon et al., 2011; Hung et al., 2020; Reidy et al., 2012; Sakzewski et al., 2012, 2015 ; Sakzewski, Ziviani, Abbott, et al., 2011a, 2011b, 2011c; Sakzewski, Ziviani, & Boyd, 2011; Taub et al., 2004). The studies that used CIMT most intensely used the therapy for 7-hr sessions (Bonnier et al., 2006; Eliasson et al., 2009). The studies that used CIMT or forced-use therapy the least intensely used the therapy for only 30-min sessions (Eliasson et al., 2018; Sung et al., 2005). However, all 4 of these studies demonstrated that CIMT was an effective intervention in improving use of the affected hand.
Effectiveness of Constraint-Induced Movement Therapy in Single-Group Research Designs
Seven studies did not have control groups. These were primarily older studies with publication dates ranging from 2001 to 2017. Six studies were single-group pretest–posttest designs (Bonnier et al., 2006; Charles et al., 2001; DeLuca et al., 2017; Gordon et al., 2007; Reidy et al., 2012; Stearns et al., 2009). One was a pilot study (Naylor & Bower, 2005).
Significant improvements in hand and upper extremity function, two-point discrimination, upper limb coordination, dexterity, strength, dissociated movements, and muscle activation were found when using CIMT or modified CIMT (mCIMT) as an intervention method (Bonnier et al., 2006; Charles et al., 2001; DeLuca et al., 2017; Naylor & Bower, 2005; Reidy et al., 2012; Stearns et al., 2009). One study found no significant improvements with mCIMT from pretest to posttest in hand or upper extremity function or quality of movement (Gordon et al., 2007).
In summary, low strength of evidence was found to support forms of CIMT as an intervention to improve hand and upper extremity function for children diagnosed with hemiparesis associated with CP in studies without a comparison group. All 6 of the single-group pretest–posttest designs were Level 3b studies, and the pilot study was a Level 2b study.
Constraint-Induced Movement Therapy Compared With No Treatment
Charles et al. (2006) did not include treatment for the control group when comparing it with the CIMT intervention group. Improved hand function and movement efficiency were present in the CIMT group compared with the control group. In addition, children were able to maintain these improvements at a 6-mo follow-up (Charles et al., 2006). In summary, moderate strength of evidence (Level 1b) was found to support CIMT as an intervention compared with no treatment to improve hand function for children diagnosed with hemiparesis associated with CP.
Variation in Constraint-Induced Movement Therapy Compared With General Rehabilitation
General rehabilitation was compared with CIMT in 12 studies (Chen et al., 2013; de Brito Brandão et al., 2010; DeLuca et al., 2006; Dong et al., 2017; Eliasson et al., 2005, 2011, 2018; Nahar et al., 2015; Sakzewski et al., 2015; Smania et al., 2009; Sung et al., 2005; Taub et al., 2004). Children receiving CIMT demonstrated significantly more gains in regard to upper extremity function. Taub et al. (2004) reported that children using CIMT acquired more motor skills (9.3 vs. 2.2) than those using conventional therapy. CIMT improved hand function and allowed children to use the hemiplegic hand more than did a general rehabilitation program (Chen et al., 2013; DeLuca et al., 2006; Dong et al., 2017; Eliasson et al., 2005; Nahar et al., 2015; Sung et al., 2005). Smania et al. (2009) reported that mCIMT improved the use and function of the affected arm with improvements being maintained at a 4-wk follow-up. The general–conventional group with which the mCIMT group was compared with did not show any improvements across any outcome measure. De Brito Brandão et al. (2010) reported that the CIMT group demonstrated higher gains than the general rehabilitation group for functional skills and independence with a large effect size of 1.37.
Eco-CIMT is CIMT with an ecological approach and follows a 10-step agenda (Eliasson et al., 2011). When Eco-CIMT was compared with general rehabilitation, it was reported that the use of the affected hand improved with Eco-CIMT, with a large effect size (1.26) observed. Sakzewski et al. (2015) compared hybrid CIMT, which combines mCIMT and bimanual training (BIM) with standard care. Both groups had significant improvements in dexterity and bimanual performance of the affected upper extremity. Baby CIMT, which is CIMT that is adapted for children younger than age 12 mo, was compared with a massage group (Eliasson et al., 2018). This study demonstrated that baby CIMT was more effective than the massage group in improving function of the affected hand.
In summary, strong evidence (7 Level 1b and 5 Level 2b studies) was found to support forms of CIMT as an intervention to improve upper extremity function for children diagnosed with hemiparesis associated with CP over general rehabilitation.
Constraint-Induced Movement Therapy Compared With Intensive Therapy
One study in this review compared mCIMT with intensive rehabilitation therapy. Wallen et al. (2011) found that neither group produced superior results. This study found no clinically significant or statistically significant differences between groups for all outcome measures when comparing mCIMT with intensive occupational therapy (Wallen et al., 2011). In summary, moderate strength of evidence (Level 1b) was found to support mCIMT and intensive therapy as interventions to improve upper extremity function for children diagnosed with hemiparesis associated with CP. However, CIMT was not more effective in improving upper extremity function than intensive therapy in this study.
Modified Constraint-Induced Movement Therapy Compared With Modified Constraint-Induced Movement Therapy With Intensive Therapy
One study compared mCIMT with the combination of mCIMT and intensive therapy (Klingels et al., 2013). The results from this study demonstrated that mCIMT with intensive therapy favors bimanual performance. However, both groups demonstrated improvements in strength, muscle tone, grip strength, and unimanual capacity (Klingels et al., 2013). In summary, moderate strength of evidence (Level 1b) was found to support mCIMT and mCIMT with intensive therapy as interventions to improve upper extremity function for children diagnosed with hemiparesis associated with CP.
Constraint-Induced Movement Therapy Compared With Hand–Arm Bimanual Intensive Therapy and Bimanual Training
In this review, 11 RCTs compared CIMT with BIM or hand–arm BIM (HABIT; Chamudot et al., 2018; de Brito Brandão et al., 2012; Friel et al., 2021; Gelkop et al., 2015; Gordon et al., 2011; Hung et al., 2020; Sakzewski et al., 2012 ; Sakzewski, Ziviani, Abbott, et al., 2011a, 2011b, 2011c ; Sakzewski, Ziviani, & Boyd, 2011). The results of these studies demonstrated that CIMT, HABIT, and BIM are all capable of improving hand function in the more-affected upper extremity. Studies have reported that both BIM and forms of CIMT showed significant improvements in personal care skills and hand function (Chamudot et al., 2018; Sakzewski, Ziviani, Abbott, et al., 2011a). In addition, when CIMT was compared with BIM at a 52-wk follow-up, it was found that both groups retained the significant gains made from baseline for unimanual capacity (Sakzewski, Ziviani, Abbott, et al., 2011b).
Both CIMT and HABIT appear to demonstrate statistically similar improvements across bimanual performance, unimanual dexterity, and whole-body movements (Friel et al., 2021; Hung et al., 2020). However, CIMT was found to produce greater continued gains toward therapeutic goals than HABIT at 6 mo (Gordon et al., 2011). In addition, Sakzewski, Ziviani, Abbott, et al. (2011a) reported that CIMT had superior outcomes compared with BIM for unimanual capacity. Bimanual performance and upper extremity functioning were examined by Gelkop et al. (2015), with the CIMT group improving 35% compared with the HABIT group, who improved 24%. Sakzewski, Ziviani, and Boyd (2011) found that the odds of producing a favorable outcome were 21 times greater for the CIMT group than the BIM group. When feelings about functioning and physical and psychosocial well-being were reviewed, it was found that results favored CIMT over BIM. However, these were not maintained at a 3-wk follow-up (Sakzewski et al., 2012). In contrast, de Brito Brandão et al. (2012) reported that HABIT resulted in greater improvements in performance on the Canadian Occupational Performance Measure than CIMT. Bimanual performance may also be improved when using HABIT rather than CIMT. Friel et al. (2021) reported an increase of 2.4 Assisting Hand Assessment (AHA) units for HABIT and 1.8 AHA units for CIMT.
In summary, strong evidence (8 Level 1b and 3 Level 2b studies) was found to support CIMT, BIM, and HABIT as interventions to improve upper extremity function among children diagnosed with hemiparesis associated with CP. However, CIMT was not more effective in improving upper extremity function than BIM or HABIT.
Constraint-Induced Movement Therapy Compared With Neurodevelopmental Treatment
Al-Oraibi and Eliasson (2011) compared CIMT with neurodevelopmental treatment (NDT) and found that CIMT improved bimanual activity and hand function. This study found that participants in the CIMT group improved from 41.6 to 48 points on the AHA, but the NDT group’s scores increased from 56 to only 56.6 (Al-Oraibi & Eliasson, 2011). In summary, low strength of evidence (Level 2b) was found to support CIMT compared with NDT as an intervention to improve hand function for children diagnosed with hemiparesis associated with CP.
Constraint-Induced Movement Therapy Compared With Constraint-Induced Movement Therapy With Botulinum Toxin Type A Injections
One study compared CIMT with CIMT after intramuscular botulinum toxin Type A (BoNT–A) injections (Eliasson et al., 2009). The BoNT–A injections improved the quality of movement when paired with CIMT. However, these improvements were not maintained at the 6-mo follow-up. CIMT significantly improved speed and dexterity, as indicated by scores on the Jebsen–Taylor Test of Hand Function (Eliasson et al., 2009). In summary, low strength of evidence (Level 2b) was found to support CIMT and CIMT after BoNT–A injections as interventions to improve upper extremity function for children diagnosed with hemiparesis associated with CP.
Constraint-Induced Movement Therapy With Transcranial Direct Current Stimulation Compared With Constraint-Induced Movement Therapy Alone
One study compared CIMT plus transcranial direct current stimulation with CIMT alone (Gillick et al., 2018). Transcranial direct current stimulation delivers low-level stimulation to adjust brain excitability (Gillick et al., 2018). The results demonstrated that there was no significant difference between intervention groups, and all participants improved hand function regardless of the group they were in (Gillick et al., 2018). In summary, low strength of evidence (Level 2b) was found to support CIMT as an intervention to improve hand function for children diagnosed with hemiparesis associated with CP. Both groups demonstrated improvements using CIMT with or without stimulation; however, because there was only 1 study in this category, a low strength of evidence supports the intervention.
Constraint-Induced Movement Therapy With Action–Observation Training Compared With Constraint-Induced Movement Therapy With Placebo
One study compared CIMT with action–observation training with CIMT with a placebo. Action–observation training aims to activate the mirror neuron system by observing others execute actions (Simon-Martinez et al., 2020). This study found that action–observation training provided limited benefits and, with or without action–observation training, proximal movement patterns improved (Simon-Martinez et al., 2020). In summary, moderate strength of evidence (Level 1b) was found to support CIMT with action–observation training and CIMT alone as interventions to improve upper extremity function for children diagnosed with hemiparesis associated with CP.
Treatment Time
Three studies compared groups receiving 3 to 6 continuous hours of CIMT treatment (Case-Smith et al., 2012; DeLuca et al., 2012; Reidy et al., 2012). All 3 of these studies found improvements in upper extremity function regardless of the treatment time. In summary, moderate strength of evidence (1 Level 1b, 1 Level 2b, and 1 Level 3b study) was found to support CIMT regardless of treatment time to improve upper extremity function for children diagnosed with hemiparesis associated with CP.
Setting
Rostami and Malamiri (2012) compared the environment in which CIMT took place. The majority of participants in this study demonstrated a significant improvement on posttest measures, including the Pediatric Motor Activity Log and Bruininks–Oseretsky Test of Motor Proficiency, regardless of the setting (Rostami & Malamiri, 2012). This study demonstrates that CIMT can be effective in either home or clinic settings. In summary, low strength of evidence (Level 2b) was found to support CIMT as an intervention regardless of setting to improve hand function for children diagnosed with hemiparesis associated with CP.
Discussion
The results of this review demonstrate that varying forms of CIMT are an effective intervention to improve upper extremity function in children diagnosed with hemiparesis associated with CP. Furthermore, the results demonstrate that CIMT, BIM, and HABIT are all effective interventions to improve function of the affected upper extremity among this population. Bimanual performance, unimanual capacity, and hand function were all aspects that improved when using these therapeutic approaches. When CIMT was compared with general rehabilitation, superior results were demonstrated among participants receiving CIMT. Improvements observed in the CIMT group included hand function, amount of use, and quality of use of the upper extremity.
The limitation to using CIMT as an intervention option is the intensive therapy that must be performed to produce the benefits. This can be challenging for families, caregivers, and children. Among the studies included in this review, CIMT was used from 30 min to 7 hr during therapy sessions. The majority of studies used CIMT for 6-hr-long sessions (Case-Smith et al., 2012; Charles et al., 2001, 2006; de Brito Brandão et al., 2012; DeLuca et al., 2006, 2012, 2017; Friel et al., 2021; Gordon et al., 2011; Hung et al., 2020; Reidy et al., 2012; Sakzewski et al., 2012, 2015; Sakzewski, Ziviani, Abbott, et al., 2011a, 2011b, 2011c; Sakzewski, Ziviani, & Boyd, 2011; Taub et al., 2004). However, regardless of the amount of time spent using CIMT, improvements were demonstrated using CIMT over control groups, if applicable.
The strength of evidence was affected for the comparisons that had only 1 study. For example, there was a low strength of evidence for CIMT’s effectiveness when compared with NDT (Al-Oraibi & Eliasson, 2011). Multiple better-designed studies with improved evidence levels for the different comparison interventions may affect the results. This could potentially be the case when examining the single-group research designs as well.
Limitations
This systematic review examined the effectiveness of forms of CIMT for participants up to age 21 years. Many differences from a motor perspective occur from infancy to early adulthood; this wide age range is a limitation of our review. In addition, there are four types of CP, and this review did not differentiate among or choose a specific type to examine. A general diagnosis of hemiparesis associated with CP was an inclusion criterion for this review. However, depending on the type of CP, the motor outcome may be affected differently. Last, various types of CIMT were included in this review, which may affect the functional or motor outcomes. Although the basis of CIMT was consistent throughout, the various modified types of the therapy could affect the effectiveness of the intervention.
Implications for Occupational Therapy Practice
CIMT should be used in occupational therapy pediatric settings. Although this type of therapy is intensive, research has consistently demonstrated it to be an effective therapy in improving upper extremity function among clients with hemiparesis associated with CP. Continually advocating for extended treatment times with pediatric clients is important to ensure they are receiving the intensive therapy they need. Education and home programs are critical to properly implement CIMT. Caregivers or parents will need to understand the purpose and methods of CIMT to be able to effectively implement the home programs to ensure beneficial motor outcomes. This systematic review has the following implications for occupational therapy practice: The results offer further evidence that CIMT is an effective therapy for improving upper extremity function among children with hemiparesis. Continued advocacy for increased time with pediatric clients is necessary to properly implement CIMT. Using CIMT may allow children to gain motor learning to improve self-care, vocational, and classroom skills. CIMT allows children with hemiparesis to learn effective motor movements that they did not previously have.
Conclusion
The majority of reviewed studies consisted of RCTs, which aided in analyzing the findings and drawing conclusions. The results of the 40 studies reviewed suggest that over the past 20 yr, CIMT has shown to be a beneficial and effective treatment when used with children diagnosed with hemiparesis associated with CP. CIMT was found to improve upper extremity function regardless of age; participants from ages 3 mo to 21 yr showed improvement. In addition, these studies are primarily Level 1b and 2b, demonstrating that the evidence is obtained from well-designed studies. Although there is sufficient evidence on this topic to conclude that CIMT is effective compared with general rehabilitation, more Level 1b RCTs are needed that compare CIMT with bimanual therapy to determine which is most effective and under which conditions.
Supplemental Material
Supplementary material for Effectiveness of Constraint-Induced Movement Therapy for Children With Hemiparesis Associated With Cerebral Palsy: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050152.pdf for Effectiveness of Constraint-Induced Movement Therapy for Children With Hemiparesis Associated With Cerebral Palsy: A Systematic Review by Adam Regalado, Bonnie Decker, Breanna M Flaherty, Lindsee Zimmer and India Brown in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
All of the authors participated in data collection and in the conceptual design of the review. The authors have no conflicts of interest and declare no financial interests in the creation of this review. This research did not receive any grants from any funding agency in the public, commercial, or not-for-profit sectors. The authors acknowledge the members of the occupational therapy faculty who provided guidance as the review was finalized.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.