
Abstract
Occupational therapy based on joint attention–based intervention can enhance the effectiveness of special education programs attended by children with autism spectrum disorder (ASD) by improving visual perception, social communication, and positive behaviors.
Any sort of nonverbal communication (e.g., glances, facial expressions, gestures, overstated responses, and voices) used to form a mutual interactive experience and draw another person’s attention is considered joint attention (Nyström et al., 2019). Joint attention behavior typically occurs between 5 and 8 mo of development and includes behavior patterns such as looking, point tracking, and pointing between the infant and the person (Mundy, 2018). There are two main categories of joint attention. The first category is the response, which refers to the infants’ ability to follow other people’s looks and gestures and, as a result, share a common social and visual reference point (Mundy, 2018). These joint attention response behaviors are present in the developmental stage (Cilia et al., 2020), before children are able to initiate this kind of interaction on their own. The second category is the spontaneous formation of a shared reference point by observing the infant’s movements, gestures, or gazes between the rest of the people (i.e., starting joint attention). The ability to respond to and initiate joint attention during infancy facilitates basic social cognition skills and language development (Brooks & Meltzoff, 2015; Cochet & Byrne, 2016). Also, a lower tendency to engage in joint attention is considered one of the hallmarks of autism spectrum disorder (ASD) in young children (Nyström et al., 2019). The capacity of children with ASD to respond to joint attention bids is effective in predicting imitation skills and is also associated with receptive and expressive language skills (Bottema-Beutel, 2016; Frost et al., 2022 ; Pickard & Ingersoll, 2015). These joint attentional behaviors emphasize social signals that express interest in objects or events. The first category involves processing other people’s signals and understanding intention, and the second category involves the processes of revealing targeted behaviors and social preference (Mundy, 2018 ; Schietecatte et al., 2012).
ASD is linked with reduced social, affective, cognitive, behavioral, and communication skills that postpone the achievement of developmental milestones and affect social roles and activities (Bhat, 2021). Children with ASD have problems with engaging and initiating joint attention, including behaviors such as establishing relationships and responding to other people, maintaining eye contact, pointing, and gesturing, as well as mutually beneficial social interaction using verbal and nonverbal communication (Clifford & Dissanayake, 2008; Franchini, Glaser, Wood de Wilde, et al., 2017 ; Key et al., 2015; Wong & Kasari, 2012). In literature, a lack of joint attention before ages 2 to 3 yr is expressed as one of the first signs and indicators of autism (Franchini et al., 2019 ; Mundy, 2016). Impairments in joint attention are seen as early indicators of ASD and have an impact on educational practices, and they are also important in developing social interaction skills (Franchini et al., 2019 ; Murza et al., 2016 ; Schietecatte et al., 2012).
In people with ASD, there is a decrease in social stimulation that is due to the lack of social orientation (the ability to independently perceive and notice social stimuli, including characters, faces, eyes, and body postures); as a result, this decrease in social stimulation affects communication skills by causing a decrease in joint attention behaviors. Some studies supporting the notion that children with ASD have less interest in social orientation have advanced the idea that the social world is important for the development of joint attention tendencies (Franchini, Glaser, Wood de Wilde, et al., 2017). In preschoolers with ASD, it has been demonstrated that social orientation and joint attention participation have a favorable association (Adamson et al., 2010). Joint attention in young children is caused by an automatic process of focusing on significant stimuli, such as eye and head motions, which are the basis of joint attention (Mundy & Newell, 2007). Studies examining the effectiveness of eye tracking in assessing social orientation in children with ASD have reported that the orientation toward dynamic social stimuli decreases and that the time spent on dynamic geometric stimuli increases (Pierce et al., 2011, 2016). These studies demonstrate the significance of emotional facial expressions in joint attention gaze shifts. Exaggerated facial expressions and gestures are different early intervention strategies that may be used to clarify the behavioral meaning of a glance or gesture, assisting joint attention (Mead & Mataric, 2010; Rogers & Dawson, 2020). Moreover, studies of ASD-related therapies indicate that expressing surprise in actual settings can encourage joint attention behaviors (Franchini, Glaser, Gentaz, et al., 2017 ; Mastrangelo, 2009). In light of this literature, using dynamic social expressions and exaggerated mimicry and coordinating pointing were seen as critical to the occupational therapy practice planned for our research. Studies have revealed the efficacy of joint attention interventions, including creating and sharing attention through eye contact in children with ASD (Freeman et al., 2015; Isaksen & Holth, 2009; Jones et al., 2006; Kaale et al., 2012; Kasari et al., 2010; Shih et al., 2021 ; Weisberg & Jones, 2018). When practicing joint attention with children with ASD, practicing synchronized staring and pointing may help them to become better at responding to joint attention bids (Von Hofsten et al., 2005). For example, Weisberg and Jones (2018) stated that intervention procedures consisting of direction and reinforcement are effective in teaching demanding and joint attention skills to children with ASD; however, individualized procedures are needed for children to acquire the skills. Kasari et al. (2010) showed significant improvements in joint attention responses and diversity of functional play actions with moderate to large effect sizes after the interventions and 1 yr after the intervention in young children with ASD. Considering the significance of joint attention in the development of communication skills in children with ASD, early intervention programs created for children with ASD are expected to promote joint attention skills (Franchini, Glaser, Gentaz, et al., 2017 ; Rogers et al., 2012).
Consciously controlled visual attention is an important factor affecting visual perception (Rensink, 2003). Attention is known to alter the quality of visual perception and behavioral response to visual stimuli (Boynton, 2005). The strategies for teaching joint attention can be used to advance cognitive performance skills such as social interaction and visual perception in children with ASD (Franchini et al., 2019). Various and coordinated activities involving joint attention are very important to children’s social and language development (Racine & Carpendale, 2007).
In the occupational therapy literature, the success that emerges as a result of the interaction of occupations with the person and the context reflects occupational performance. Occupational performance is a multidimensional construct that encompasses process skills, motor skills, and social interaction skills (American Occupational Therapy Association [AOTA], 2020). As indicated in the literature, joint attention is a comprehensive and important skill for a child with ASD to acquire to socially stimulate and initiate a qualified response to the social world. For this reason, among children with ASD, the promotion of joint attention skills that are accepted as a co-occupation and facilitation of children’s occupational performance are explicitly related (Eschenfelder & Gavalas, 2017). Joint attention training strategies are in line with occupational therapy methods and boost the effectiveness of occupational therapy interventions (Eschenfelder & Gavalas, 2017).
It is important to have a holistic and client-centered perspective in occupational therapy practice (AOTA, 2020). Tanner et al. (2015) stated that to improve social communication and interaction skills among children with ASD, occupational therapy interventions should adopt joint attention strategies, and more research should be planned in this area. In addition, Frolek Clark and Schlabach (2013) advised that joint attention interventions increase play, language, and social interactions among preschool children with autism, and they generalize to new situations. Moreover, further research conducted by occupational therapy practitioners is needed to identify intervention strategies that involve joint attention. Occupational therapy practitioners should consider using joint attention strategies that also address functional cognitive skills to strengthen play and leisure activities, improve social participation, and address social skills limitations in children with ASD (Tanner et al., 2015). To our knowledge, no study has investigated the effect of joint attention–based holistic occupational therapy intervention on visual perception. Therefore, this study aimed to offer a joint attention–based holistic occupational therapy intervention to attract the attention of another person, create an interactive experience and communication style, and improve visual perception in children with ASD and to examine the effects of this training on children’s social communication, ASD-related behaviors, and visual perception skills.
Method
Participants
Twenty children (10 each in the study and control groups) participated in this study. The study inclusion criteria were ages 4 to 6 yr and a diagnosis of ASD. The participants included in our research were children who were diagnosed with ASD according to the report of the health board of hospitals affiliated with the Ministry of Health. Children with a comorbid condition in addition to ASD were not included in the study to eliminated confounding factors. In addition, children who had previously attended a training course were excluded to obtain a better understanding of the effectiveness of the occupational therapy intervention. Between April 2020 and February 2021, a total of 28 children were interviewed for this study. Three children were excluded because they did not meet the inclusion criteria (they had previously participated in training and had received a diagnosis of a comorbid condition). Thirteen children were randomly assigned to the study group, and 12 children were randomly assigned to the control group. Three children from the study group dropped out because of time, transportation, or other reasons, and 2 children from the control group were dropped because they did not complete the second evaluation. As a result, a total of 20 children with ASD (10 study participants and 10 control participants) formed the sample (Figure 1).
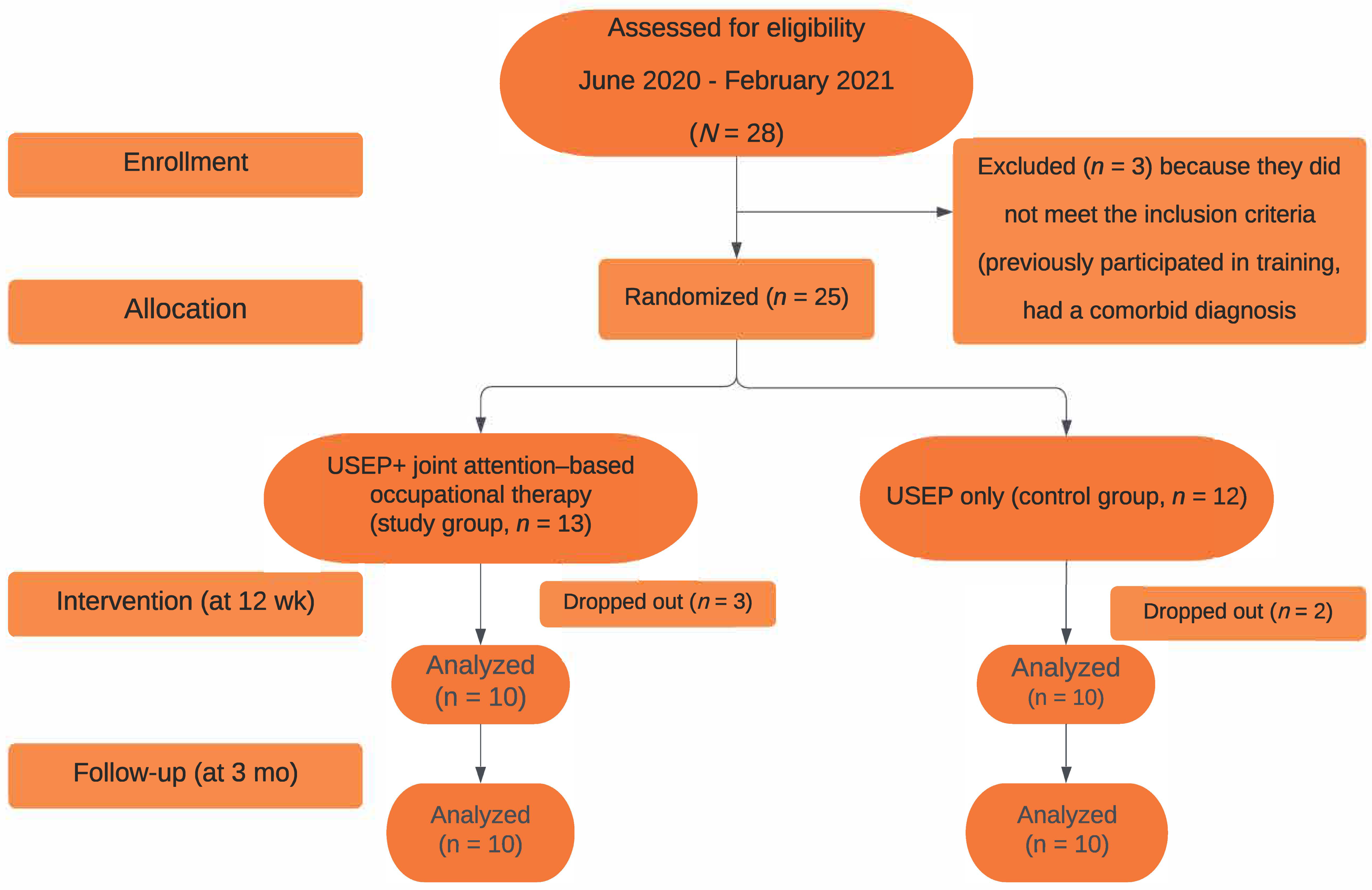
Flow of participants through the study.
Informed consent was obtained after the scope and purpose of the study were explained in detail to the participants and primary family caregivers. The research was conducted in accordance with the Helsinki Declaration. The Clinical Research Ethics Committee of the Ondokuz Mayis University provided approval for the study (Decision No. 2020/126).
Assessments and Trial Design
Joint attention is an important multidimensional (sensory, motor, process, social) skill, in terms of both social communication and the development of play behaviors. Therefore, the Turkish versions of the Social Communication Questionnaire (SCQ; Avcil et al., 2015), Autism Behavior Checklist (ABC; Yilmaz- Irmak et al., 2007), and Motor-Free Visual Perception Test–4 (MVPT–4; Köse et al., 2021) were administered to the children before and after the intervention, and the results were compared.
The validity and reliability of the SCQ were originally reported by Berument et al. (1999). The SCQ items correspond to the diagnostic criteria for autism outlined in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994). The questions cover social interaction; communication; and repetitive, stereotypical patterns of behavior (Eaves et al., 2006). The SCQ is a 40-item scale that is completed by the primary caregiver. Each item is answered yes or no, with 1 or 0 points, respectively, indicating whether developmentally inappropriate behaviors are present. The scoring is completed by a clinician. The total score can be between 0 and 39 for children who can speak. A high score indicates low social communication skills. The Turkish version of the SCQ—which consists of three subscales: Reciprocal Social Interaction, Language and Communication, and Repetitive and Stereotyped Patterns—has validity and reliability (Avcil et al., 2015).
The ABC, developed by Krug et al. (1980), is among the scales used for screening and evaluating education in autism in many countries. It is completed by the caregiver and consists of five subscales: Sensory, Relating, Body–Object Use, Language, and Social and Self-Help. The total score can range from 0 to 159; a high score indicates the presence of typical ASD- related behaviors (Yilmaz-Irmak et al., 2007).
The MVPT–4 is an instrument that presents a fast, reliable, and valid evaluation of children’s and adults’ general and visual perceptual abilities. It consists of 45 items that are organized and grouped to provide a smooth implementation process. The items consist of black-and-white drawings and patterns developed to present answer options. Motor skills are not necessary to provide a response, which makes this test useful, especially for people with motor disabilities. A high score reflects good visual perception (Köse et al., 2021).
All children included in the study attended the usual special education program (USEP) for two sessions per week in a rehabilitation center. The USEP intervention included gross motor skills (e.g., walking within a defined area), communication skills (e.g., performing simple one-step verbal instructions), preschool preparation skills (e.g., relationship building, matching), and self-care skills (e.g., hand washing, brushing teeth). The control group consisted of children attending the USEP. Children in the study group received an occupational therapy intervention that was based on joint attention in addition to the USEP. The intervention sessions were conducted 3 days/wk for a total of 12 wk. The initial assessments were administered to children in both groups. At the end of the 12 wk, the evaluations were repeated in both groups. Follow-up evaluation was performed in both groups 3 mo after the second evaluation.
Occupational Therapy Procedure
The acquisition frame of reference, which proposes to shape the behaviors that contribute to skill acquisition, and the developmental frame of reference, which emphasizes the continuous change and emergence of skills with age, guided the occupational therapy intervention (Case-Smith et al., 2001; Royeen & Duncan, 1999). Therefore, all activities were designed according to the chronological and developmental ages of the children. During the joint attention–based intervention sessions, holistic occupational therapy approaches to the child’s sensory, physical, social, language, and communication deficits were prioritized.
Four Approaches Used in Occupational Therapy Practice
In the first approach, each parent was interviewed about the child’s preferences. The types of toys preferred by a child and those toys to which a child might react negatively were identified. The therapist selected 15 toys to conduct paired stimulus preference assessments: Five of these toys were stuffed animals and figures; 5 consisted of multipart activities; and the remaining 5 consisted of toys activated by light, movement, or sound. Each group of toys was used according to the child’s interests and habits in three stages: (1) creating a response to a joint attention offer, (2) initiating joint attention, and (3) reinforcing a joint attention response. One of the authors, therapist Mahmut Yaran, added visually striking and unusually placed items to the environment before each session. When the child entered the room, the therapist waited for the child to initiate the offer of joint attention. Subsequently, when the child initiated the offer, the therapist showed a socially appropriate response.
If the child’s attention was directed toward an object that was not striking and newly placed, the therapist directed the child toward the target object and initiated joint attention by picking up the target toy. When the child became involved in the activity, the therapist associated the toys with expressions such as “Wonderful!” “Ooh!” “Wow!” and “Look!” in an appropriate and enthusiastic manner.
The therapist used the less-to-more orientation to get the child to respond to the offer of joint attention. For example, if the child did not respond to the joint attention offer within 5 to 10 s, the therapist first directed the child, using exaggerated gestures, to move toward the targeted toy. If the child still did not respond, the therapist slowly directed the child’s head physically. In addition, the therapist gave a verbal command (e.g., “Look at how his arms are waving [pointing to the toy]; now, look at me”). When the child looked at the toy and reacted, the therapist again gave enthusiastic and activity-appropriate feedback (e.g., he tickled the child, saying, “Isn’t it weird, is there ever such a long arm?”). The therapist followed the child’s interest and leadership in the activities, including what the child did and said. Positive feedback was then provided when the therapist offered it, even if the child partially attempted or initiated joint attention.
In the second approach, the Dynamic Model for Play Choice, the formation of play preferences is the outcome of a nonlinear process, and the choice of play activity is dynamic in character. According to this paradigm, the way in which a person views entertainment reflects attraction and the individual play patterns that support a child’s self-organization process in response to this attraction. When a child repeats play activities they find enjoyable, they feel good, and this causes them to repeat choices or patterns of choices that may also manifest as a liking for that play activity. Persistence in a play selection indicates a pattern, and the repetition of that pattern might be interpreted as a liking for that selection. Consequently, the choice of this amusingly and repetitive play pattern by the child and the therapist, with the therapist making funny sounds and gestures, helps in the development of emotional meaning (Miller & Kuhaneck, 2008). During the joint attention–based occupational therapy intervention, researchers paid attention to maintaining eye contact: The therapist called out the child’s name to make eye contact. If necessary, the therapist called the child’s name again, and if the child still did not respond, the therapist made a funny sound and a funny facial expression (Nyström et al., 2019), while following the child’s lead. Activities were conducted at the desk and on the floor. A play pattern was created using the selected toys; the pattern was planned and implemented as activities for an average of 20 min.
In the third approach, fine motor activities such as handicrafts and finger games; gross motor activities such as obstacle courses, music, and dance; and visual–motor activities such as drawing, cutting, and assembly were used. The focus of the intervention was initiating and responding to joint attention during these activities. With the training, the aim was to generalize behavioral skills and transfer them to the context of social play. In practice, occupational therapists specifically address the child’s interests and reactions to sensory, tactile, auditory, visual, and vestibular stimuli individually. In joint attention–based occupational therapy, the child’s response to joint attention and the initiation and maintenance of joint attention were the focus.
With regard to the fourth approach, compatible environmental arrangements that provide visual cues are important when structuring environmental activities, because children with ASD respond to the use of visual input (Case-Smith & Arbesman, 2008). Visual environmental supports typically applied by pediatric rehabilitation practitioners include pictorial directions, photographic activity charts, checklists, video-recorded modeling, activity sequences, and color coding, as well as changes to the sensory properties of the environment and materials used in a task (Derakhshanrad & Piven, 2019). For this reason, environmental arrangements were made, using visual stimuli that could attract a child’s attention. Although the same room was used as the session environment for each child, the materials used during the sessions varied, with the games and toys that each child liked taken into account. For example, for one child, materials (e.g., picture prompts, photographic activity schedules, colorful toys) with different visual content were used to provide an enriched environment, such as different: One carton had a picture of different colored fish, another had a fishing rod, and a third had a boy fishing. At the same time, we used miniature toy fishing rods and fish with magnetic hooks and colorful modeling compound. The visually colorful cartons and toys were used in the child’s play pattern (Aronoff et al., 2016; Woo & Leon, 2013).
Randomization and Blinding
One of the authors, Esma Özkan, developed and securely kept a digital randomization list. Children who met the inclusion criteria were randomly assigned to the groups, with equal probability and independent of previous assignment, by means of computer software. At baseline, posttest, and follow-up testing, Sümeyye Belhan Çelik, who made the evaluations, was blinded to the children’s group assignment.
Statistical Analysis
As descriptive statistics, means and standard deviations were used for continuous data, and frequency and percentage were used for categorical data. The conformity of the variables to the normal distribution was checked using the Kolmogorov–Smirnov test, and the homogeneity of the variances was checked using Levene’s test. The distribution of categorical variables in the groups was evaluated using Fisher’s exact test. Group means of normally distributed continuous variables were compared using Student’s t test.
The assumption of sphericity was assessed using Mauchly’s sphericity test statistic. The effectiveness of the intervention was evaluated using a mixed-design (split-plot) analysis of variance (ANOVA) when the sphericity assumption was met. A mixed-design (split-plot) ANOVA with a Greenhouse–Geisser correction to the degrees of freedom was used if the sphericity assumption was not met. When the interaction effect was found to be statistically significant as a result of the analysis, a Bonferroni-corrected simple-effects analysis was used to find the source of the difference. When the effect of interaction was not statistically significant, the sources of significant differences in the main effect of group and time were found with the Bonferroni adjustment post hoc test (Jamieson, 2004; Rutherford, 2011). Clinical significance was determined according to partial eta-squared (η2) and the cutoff values suggested by Cohen (1988) for ANOVA (.0099 for small effects, .0588 for medium effects, and .1379 for large effects). Data were analyzed using IBM SPSS Statistics (Version 21) package program. Statistical significance level was set as .05.
Sample Size
G*Power software (Version 3.1.9.2) was used to assess the study’s power and effect sizes. The sample size was calculated using a power analysis. To achieve an 80% power, 8 participants in each group were required, assuming a two-tailed test for α = .05 with an effect size (Cohen’s d) of 1.6. The statistical significance level was set as .05.
Results
Twenty children with ASD were included. Of the 20 children, 11 (55%) were male and 9 (45%) were female. The participants’ mean age was 4.95 yr (SD = 0.76). Table 1 shows that the gender distribution in both groups was homogeneous (p = 1.000). There was no statistically significant difference between the mean ages of the two groups, t(18) = 0.878, p = .391.
Comparison of Demographic Information and Distributions of the Groups
Fisher’s exact test statistical value.
Student t test statistical value.
The results of Mauchly’s sphericity test showed that the sphericity assumption was met for the SCQ Reciprocal Social Interaction, Repetitive and Stereotyped Patterns, and Total subscale variables and for the ABC Sensory, Body–Object Use, Language, Social and Self-Help, Relating, and Total subscale variables. Therefore, we used a mixed-design (split-plot) ANOVA for statistical analysis of these variables (Table 2), with a Greenhouse–Geisser correction made to the degrees of freedom for the SCQ Language and Communication and MVPT–4 variables (Table 3). The interaction effect was statistically significant for SCQ Reciprocal Social Interaction, Repetitive and Stereotyped Patterns, and Total; ABC Sensory, Body–Object Use, Language, Social and Self-Help, Relating, and Total; and the MVPT–4 variables (p < .05). For children in the study and control groups, mean scores on the SCQ Reciprocal Social Interaction, Repetitive and Stereotyped Patterns, Language and Communication, and Total; ABC Sensory, Body–Object Use, Language, Social and Self-Help, Relating, and Total; and MVPT–4 differed significantly over time (p < .05). For the within-group analyses, averages for the SCQ Reciprocal Social Interaction, Repetitive and Stereotyped Patterns, and Total; ABC Sensory, Body–Object Use, Language, Social and Self-Help, Relating, and Total; and MVPT–4 variables measured at three different times in the study group were evaluated, and the averages measured after training and at follow-up were significantly different from those measured before training (p < .001; see Tables 2 and 3).
Mixed-Design (Split-Plot) ANOVA Results
Note. N = 20; study group, n = 10; control group, n = 10. A = study group; B = control group; 1 = before training; 2 = after training; 3 = follow-up. ABC = Autism Behavior Checklist; ANOVA = analysis of variance; SCQ = Social Communication Questionnaire.
Simple effects analysis with Bonferroni correction was used.
F test value.
Statistical significance was found (p < .05).
Mixed-Design (Split-Plot) ANOVA Results with Greenhouse–Geisser Correction
Note. N = 20; study group, n = 10; control group, n = 10. A = study group; B = control group; 1 = before training; 2 = after training; 3 = follow-up. ANOVA = analysis of variance; MVPT–4 = Motor-Free Visual Perception Test–4; SCQ = Social Communication Questionnaire.
F test value (with Greenhouse–Geisser adjustment to the degrees of freedom).
The mean difference is significant at p < .05.
Simple effect analyses with Bonferroni adjustment were used.
Partial eta-squared (η2) value.
According to the mixed-pattern ANOVA results for the SCQ Communication variable, the interaction effect was not found to be statistically significant, F(1.345, 24.376) = 1.775, p = .196, η2 = 0.090. Therefore, the main effects were evaluated. In a between-groups comparison of the averages of the study and control groups, the mean of the study group (3.733) was found to be statistically significantly lower than the mean of the control group (7.700; p < .001; see Table 3). In a between-times comparison of the marginal averages of the first, second, and third times, the mean for Time 1 (6.250) was found to be statistically significantly higher than the average for both Time 2 (5.350) and Time 3 (5.550; both ps = .001; see Table 3).
With the partial η2 effect size index, the effectiveness of the intervention was evaluated according to the cutoff values suggested by Cohen (1988; .0099 for small effects, .0588 for medium effects, and .1379 for large effects). Joint attention–based occupational therapy had a large effect level for the SCQ Reciprocal Social Interaction, Repetitive and Stereotyped Patterns, Language Communication, and Total; ABC Sensory, Body–Object Use, Language, Social and Self-Help, Relating, and Total; and MVPT–4 variables, according to the partial η2 effect size index (see Table 2).
Mean scores on the SCQ Total, ABC Total, and MVPT–4 variables for the study group measured at follow-up were significantly different from those measured before and after training (p < .05; see Tables 2 and 3). The follow-up findings show that the training maintains its effectiveness compared with the pretraining period but that the effectiveness of the therapy decreases by the third month compared with the posttraining measurement.
Discussion
The primary objective of this study was to examine the effects of the joint attention–based approach on communication, ASD-related behaviors, and visual perception in children with ASD as an early occupational therapy intervention. We have four main findings. First, the study suggests that occupational therapy intervention that is based on joint attention in the preschool period may be effective in changing some aspects of basic social communication among children with ASD. Deficits in joint attention are a problem for children with ASD because they affect language as well as social and cognitive development. Joint attention intervention studies have shown improved skills for children with autism (Eschenfelder & Gavalas, 2017). These studies determined that training improved autistic children’s skills in initiating and sustaining joint attention and social interaction skills (Muzammal & Jones, 2017; Shih et al., 2021 ; Weisberg & Jones, 2018). Olafsen et al. (2006) revealed that children in the intervention group received significantly higher scores for initiating attention, initiating object demands, and responding to social interaction than those in the control group. They also observed that children who received a joint attention intervention maintained coordination for significantly longer periods and improved their developmental skills (Olafsen et al., 2006). In a study by Whalen and Schreibman (2003), interventions included basic intervention training as well as natural behavior modification techniques and components of discrete trial training. In the posttreatment evaluation and 3-mo follow-up, positive responses were observed in social interventions, imitation, play, and spontaneous speech (Whalen et al., 2006), and joint attention was maintained.
We noticed improvements in children’s skills through their reciprocal social interactions and social relating skills; the children were encouraged to use and imitate various gestures, which increased their ability to shift attention from one activity to another and to maintain attention during the activity. For example, when a child was talking to her therapist, she was able to continue talking to her therapist when she saw a friend passing by in the hallway, and she said goodbye, waving as she left. Moreover, effect sizes confirm the effectiveness of the treatment. Occupational therapy intervention that is based on joint attention applied to the study group seems to have a high clinical effect on social communication.
The second finding in this study is that children generalized the skills they learned from child-centered intervention sessions to other behaviors. For instance, the children who learned to wait for their turn to switch to the toy they wanted during the session were more patient and flexible while waiting their turn in other contexts (e.g., at home, at kindergarten). Similarly, when their visual perception abilities improved, they were better able to avoid potentially hazardous stimuli in playground (e.g., barriers, ramps, and stairs). During the family interviews after the session, the families gave feedback that the children were more successful in their preschool activities.
Some studies have stated that the skills gained in intervention sessions are difficult to generalize to different people or settings (Kasari et al., 2006; Whalen & Schreibman, 2003). Practitioners in preschool programs provide interventions that include individual learning opportunities for children in their natural routines and activities (Hinojosa & Kramer, 1997). Many studies have shown the effectiveness of occupational therapy interventions with children with autism (Case-Smith & Arbesman, 2008; Kadar et al., 2012; Simpson, 2015 ; Watling & Dietz, 2007). Some of these studies were based on sensory integration (Case-Smith & Bryan, 1999; Schaaf et al., 2012); some on auditory integration (Dawson & Watling, 2000; Mudford et al., 2000); and some on social, emotional, and behavioral interventions (Eldevik et al., 2006 ; Field et al., 2001). These studies in the literature resulted in reduced hyperactivity, decreased impulsivity and stereotypical behaviors, and improved on-task behaviors among children with ASD.
During our intervention, we tried to create coherent environments that prevented ASD-related behaviors among children. One of our main aims was to eliminate or modify the causes of behavioral issues. When children displayed troublesome behaviors, we focused on modeling, guiding, hinting, teaching, and reinforcing. In light of the practices described in the literature (Hayward et al., 2009; Pas et al., 2016; Su Maw & Haga, 2018), for example, when a child aggressively threw a toy in the present study, we retrieved the toy from the place where it was thrown and calmly explained and demonstrated how to play with the toy, using verbal and gestural prompts. The child was then asked whether he wanted to play with the toy, and the toy was then extended to them. Positive reinforcement was provided when the child looked at the extended toy or reached out to it. Such reinforcement was also provided when inappropriate behavior did not occur in a certain time interval; for example, when the child did not throw objects in a 2-min interval, he was given a toy that he wanted very much. Another child, who had a tantrum to get the item he wanted, was encouraged to say the name of the item that he wanted.
At the same time, we provided structure and a routine for behavioral problems when verbal communication was insufficient; that is, we made an effort to implement prevention strategies by changing the environment and providing a suitable environment for the children in the study group. Weighted blankets, rocking chairs, and a quiet, peaceful sitting corner were supplied to provide calming proprioceptive inputs and help the children to get organized and feel safe. In addition, social stories and visual representations were used to reinforce classroom rules and reveal desired behaviors during occupational therapy practice. As a result of our study, improvement was observed in all subscales for the ABC in the study group. We think that the strategies we used to achieve this improvement are effective. We believe that, when developing new occupational therapy interventions, it is critical to include sensory, auditory, behavioral, and social approaches to behavioral disorders.
Visual perception requires both spatial and temporal integration of information (Spillmann & Werner, 2012). The weak central coherence theory suggests that people with ASD have deficits in the high-level processes that consistently integrate elements of the visual component (Hsu & Hinojosa, 2013; Van der Hallen et al., 2015). This causes children with ASD to treat elements as separate components rather than as a unified whole (Kaiser & Shiffrar, 2009). Studies have revealed that children with ASD have deficiencies in detecting movements during low-level visual stimulation, emotional processing, and facial expressions, even at very young ages (Evers et al., 2011; Guy et al., 2019). In their studies, Ambrose et al. (2020) and Swanson and Siller (2013) discussed eye tracking and joint attention in children with ASD and observed differences in gaze use and interactive joint attention. In addition, children with ASD expressed difficulties in flexible changing of gaze and social learning (Ambrose et al., 2021; Swanson & Siller, 2013).
However, no study has yet been conducted to examine the effects of joint attention interventions on visual perception. The third important finding in our study revealed that the 12-wk joint attention–focused occupational therapy intervention improved visual perception in children with ASD in the study group. It has been reported that simplified social environments and joint attention demand positively affect joint attention performance in children with ASD (Ambrose et al., 2020). Studies (Bejnö et al., 2021 ; Dargue et al., 2022 ; Gaines et al., 2016; Martin, 2016) have indicated that environmental changes (e.g., space, sensory aspects, lighting [daylight vs. artificial], furniture, fixtures, and materials) result in better participation among children with ASD; in light of these studies, we created a calm and supportive session environment with well-organized routines and reduced distraction, in which materials and toys were accessible. In this study, and also in the literature, the use of toys and objects that attract children’s attention during sessions and the provision of a simplified environment containing a small number of objects or toys are thought to be important for this.
Another result of our research is that, although the follow-up measurement showed an improvement compared with the pretraining measurement in the total results for communication, behavior, and visual perception, the significant difference between the follow-up measurements and the intervention measurements shows that some regression occurred. Whalen and Schreibman (2003) also reported a decrease in the positive effects of joint attention at a 3-mo follow-up. Krstovska-Guerrero and Jones (2016), who implemented an intervention to initiate joint attention for 4 children, reported an increase in positive effects in the 1- to 3-mo follow-up results, compared with the evaluation at the end of the intervention. In their 1-yr follow-up study, Kasari et al. (2010) emphasized that an intervention for caregivers of young children with autism resulted in increased joint involvement between caregivers and young children and increased children’s joint attention skills and variety of play. In our study, the difference between the results at the 3-mo follow-up evaluation and those before the intervention emphasizes the effectiveness of the training. However, the difference between the posttraining and 3-mo follow-up reflects concerns about the long-term preservation of effects on social communication, behaviors, and visual perception.
Implications for Occupational Therapy Practice
Combining holistic occupational therapy behavioral methods and child-centered play practices for preschool children with ASD can help them to develop skills relating to joint attention. When planning holistic occupational therapy practices for children with ASD, practitioners should consider the child’s individual interests; use the child’s chosen game and toy, which can serve as a therapeutic function in joint attention training; and enrich the environmental stimuli that support visual perception.
Conclusion
Previous studies concerning occupational therapy practices with children with ASD have focused on joint attention training (Ambrose et al., 2020, 2021 ; Eschenfelder & Gavalas, 2017; Tanner et al., 2015). Our study is unique in the occupational literature in that it addresses joint attention skills and visual perception together. It provides additional data on joint attention–based occupational therapy for children with ASD, covering dimensions such as communication, behaviors, and visual perception. With this limited participant set, we demonstrated that children with ASD could develop social communication, reduce ASD-related behaviors, and enhance visual perception through a 3-mo joint attention–based occupational therapy intervention. As Kasari et al. (2006) stated, children’s involvement in other interventions during a study may create difficulties in interpreting the results and determining whether the changes occurred solely because of the intervention they received. The most important limitation of our study is that all the children included in the study continued to participate in a general special education program. To keep the effect of this limitation to a minimum, we designed our study as a randomized controlled trial. In future studies, the addition of a third group that has never been involved in an intervention program may increase the level of evidence of the findings. In addition, our study included one follow-up evaluation but did not include interim evaluations; nor did it include both short-term and more long-term follow-ups. For future studies, following up regularly during and after the intervention to generalize the behavior and determine the duration of action is recommended. Besides further studies, families should be involved to determine whether they can assist in maintaining the positive effects of the intervention. In addition, assessment and intervention in our research were based on nonautistic social communication patterns. According to current theories, barriers to social interaction should be considered not only for an individual but also for all social factors (Milton et al., 2020). Differences in social perceptions and interpretations between autistic and nonautistic people cause a “double empathy problem” in which both people have difficulty empathizing with the other person (Mitchell et al., 2021). Considering the dual empathy approach, accepting nonautistic social communication methods as the gold standard can be seen as a limitation. The literature reports that research and practice with autistic students should focus on the inclusion of neurodiverse social styles, reflecting the neurodiversity perspective, and address interpersonal and environmental factors associated with participation rather than individual factors and social characteristics related to ASD (Chen et al., 2021, 2022 ; den Houting, 2019). Future occupational therapy practice research can examine social and other contexts for children with ASD, examine the social challenges and interactions of children with ASD, and incorporate these contexts into practice.
Footnotes
Acknowledgments
This study is registered with ClinicalTrials.gov (NCT05106166). The authors have no conflict of interest to disclose. This study did not receive financial support.