
Abstract
This study highlights the importance of a holistic approach in occupational therapy for patients with distal radius fractures (DRF) and reveals that standard measurements might overlook key challenges that they face. By adopting broader evaluative methods, occupational therapists can better address patient-specific needs and enhance their rehabilitation outcomes.
Distal radius fractures (DRFs) have consistently been reported as one of the most common injuries in people older than age 50 (Court-Brown et al., 2018; Pietri & Lucarini, 2007). The aging population is expected to experience an increasing number DRFs in coming years (Stirling et al., 2018; Ydreborg et al., 2015). People with a history of fractures, in particular those with an age-related increased risk of falls (e.g., osteoporosis), have a heightened risk of future fractures (Miyamura et al., 2020). Although DRFs do not result in high mortality (Benzinger et al., 2019), many people continue to report residual wrist pain and disability even 1 yr after the fracture (Cowie et al., 2015; Jellad et al., 2014; MacDermid et al., 2003; Moore & Leonardi-Bee, 2008). Long-term functional outcomes for people with a DRF have been reported in different studies on the basis of results from patient-reported outcome measures (PROMs). These studies indicate that people report persistent pain and disability despite healing of the fracture site (Lalone et al., 2017; Landgren et al., 2019). PROMs cannot capture all areas of function, activities, or aspects of importance to the individual.
Some studies have used patient-centered measures, such as the Canadian Occupational Performance Measure (COPM; Law et al., 1990). Results have shown that pain and disability decrease the person’s ability to use the injured hand during activities of daily living (ADLs) and occupation. Impairments and activity restrictions are expected to limit occupational performance (Dekkers & Nielsen, 2011; Nielsen & Dekkers, 2013). People with persistent pain and disability will experience limitations in different occupational performance areas, such as family roles, self-care, productivity, and leisure (Dahlqvist & Rosén, 2016; Dekkers & Søballe, 2004; Nielsen & Dekkers, 2013; Schleis, 2017; Ydreborg et al., 2015).
To describe and analyze the functional consequences of various health conditions, the World Health Organization (2001) developed the International Classification of Functioning, Disability and Health (ICF; see also Stucki et al., 2002). The ICF Core Set for Hand Conditions was developed from the general ICF to highlight priority structural, impairment, and disability concerns in people with hand injuries (Kus et al., 2012).
Disability assessed through an ICF lens overlaps with occupational performance. Understanding the concerns of a person after a DRF can help guide rehabilitation. Therefore, the purposes of this study were to describe the scope and distribution of self-perceived occupational performance and satisfaction with the performance of daily activities in patients with DRF when linked to ICF codes. A secondary aim was to describe the association between occupational performance as measured by the COPM, disability as measured by Patient-Reported Wrist Evaluation (PRWE; MacDermid et al., 1998), and the Participation Behavior Questionnaire (PBQ; Farzad et al., 2017).
Method
After receipt of institutional review board approval, we prospectively enrolled 120 patients in a cross-sectional study over the course of 4 mo. We included patients who met the following three criteria: (1) age ≥18 yr, (2) DFR with an onset of 12 to 14 mo prior, and (3) the capability to provide informed consent. Patients with (1) any concurrent tendon or nerve injuries or (2) self-reported pain conditions, and those with (3) any underlying diseases, such as diabetes or arthritis, were excluded (Figure 1).
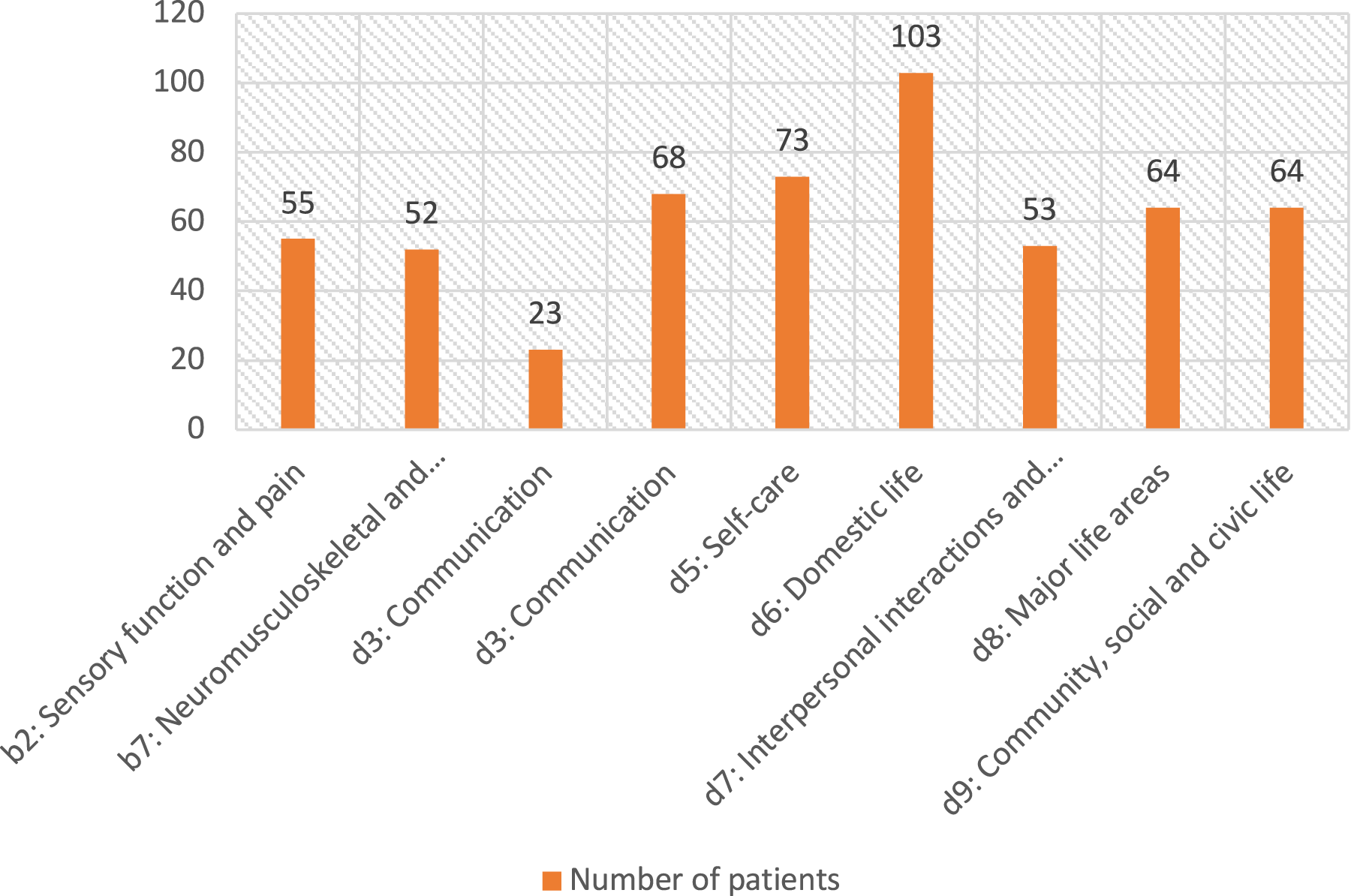
Number of patient-reported difficulties in different areas of the ICF.
The data collection consisted of the recording of sociodemographic data and the completion of several self-report health status questionnaires. We retrospectively identified patients who met the inclusion criteria from their records in the database of a trauma center from an outpatient hand surgery clinic. A research assistant called the patients and approached them to inquire about participation and present informed consent. Then, an occupational therapist completed a COPM measure while interviewing patients to address their occupational performance and satisfaction with that performance. The interview lasted 1 hr and focused on activities the patient wanted, needed, or was expected to perform. Patients were also asked to describe their disability and occupational performance extending beyond that required to complete the COPM.
Measures
COPM
The COPM was developed on the basis of the Canadian Model of Occupational Performance and Engagement to evaluate respondents’ self-perceptions of occupational performance and their satisfaction with that performance in the areas of self-care, productivity, and leisure. It is a semistructured, patient-specific outcome measure administered through a patient interview (Law et al., 1998). We used the COPM to describe and measure the qualitative and quantitative occupations perceived by the patients. During the interview, patients were asked to identify any occupations they would like, or need, to do but found difficult to complete because of their DRF. They were asked to define their occupational performance problems in three areas: (1) self-care (what a person needs to do, i.e., personal care and basic needs), (2) productivity (what a person is obliged to do, i.e., contribution to the social and economic fabric in the community), and (3) leisure (what a person wants to do, i.e., how to enjoy life). The patients were asked to rate the importance of these activities on a scale that ranged from 1 (not important at all) to 10 (extremely important). We then asked the patients to rate the five most important activities for performance, and their satisfaction with their performance, on a scale that ranged from 1 (not satisfied at all) to 10 (satisfied). To better define the affected domains of health. We calculated total performance and satisfaction scores by dividing the sum of the scores by the number of problems. Total scores can range from 1 to 10, with higher scores indicating better occupational performance and more satisfaction. The Persian version of COPM was used in this study (Dehghan et al., 2015).
PRWE
The PRWE is a reliable and valid measure containing standard items that ask about the respondent’s level of difficulty in performing different activities (Shafiee et al., 2022). It is a 15-item self-report questionnaire that evaluates disability with two subscales—Pain and Function—in patients with wrist and hand injuries. We used it to measure residual pain and disability. On each of these two subscales respondents rate their level of pain and disability on a scale that ranges from 0 (no pain/disability) to 10 (extreme pain/disability). Scores range from 0 to 100, with higher scores indicating more pain and disability. The Pain subscale contains 5 items with a score range from 0 to 50. The Function subscale contain 6 items related to specific activities and 4 items related to usual activities. The Function score is calculated by summing the score of all 10 items, divided by 2, and can range from 0 to 10. We used the Persian version of the PRWE, which is reliable and valid in assessing pain and disability in people with wrist and hand diagnoses (Farzad et al., 2019; MacDermid et al., 1998). A score ≥12.5/50 on the Pain scale is considered an indicator of persistent pain (Mehta et al., 2015). A PRWE score of >35/100 is considered as indicating a residual disability (Grewal & MacDermid, 2007).
PBQ
The PBQ was developed in the Persian context to evaluate participation in patients with hand and upper extremity injuries. It comprises a set of 30 self-report items that ask the respondent about the effect of the injury on their participation in important aspects of their life during the past few weeks. Each item is rated on a scale that ranges from 0 (totally disagree) to 3 (strongly agree). The total score is calculated by summing all item score; this total score can range from 0 to 90, with higher scores indicating more limitations in participation (Farzad et al., 2017). An item separation index of .91, person separation index of .96, and intraclass correlation of .97 indicated a good reliability of the PBQ. The PBQ questionnaire aligns well with the Rasch model. Its validity is confirmed by its unidimensionality and the absence of any misfitting items (Farzad et al., 2017).
Statistical Analysis
We conducted a post hoc power analysis, using G*Power software, that indicated that a sample of 120 patients would provide 95% power to detect a small correlation between disability as measured by the PRWE with participation as measured with the PBQ versus occupational performance as measured by the COPM. To address our study purposes, we used two interpretative (qualitative) phases and an analytic phase. The analytic phase was used to describe the sample and to determine the correlations between the variables, and the interpretive phase was used to link the results from the COPM to the ICF Core Set for Hand Conditions.
Qualitative Analysis
The recorded interviews were transcribed and qualitatively analyzed using thematic analysis. Meaningful concepts were extracted from the patients’ responses in the interviews. Axial coding was used to categorize and define the codes from the responses’ extracted meaning units (Williams & Moser, 2019). First, the extracted codes were categorized on the basis of the three areas of the COPM (self-care, productivity, and leisure). Then, the extracted meaningful units were linked with the ICF Core Set for Hand Conditions (comprehensive and brief versions) and the ICF Generic Set using the updated linking roles (Cieza et al., 2019).
In accordance with the updated guidelines (Cieza et al., 2019), we considered the overall purpose of the patients’ responses and linked them to the most precise level possible of the categories from the ICF Core Set for Hand Conditions. Any other identified concept was identified as an additional concept. General concepts that could not be linked with the categories from the ICF Core Set for Hand Conditions but could be assigned to the general ICF categories were categorized as “unspecified.” When a meaningful concept was identified as a personal factor, it was labeled PF, and when a meaningful concept was not covered by the ICF, such as quality of life in general, it was labeled NC (not covered; Bernardelli et al., 2021; Cieza et al., 2019). We also categorized responses to either capacity or performance on the basis of patients’ definitions. Capacity is a person’s intrinsic ability to carry out tasks or actions independent of the environment, and performance captures how well the individual can perform those tasks in their real-life environment (Almansa et al., 2011).
To map and decide the extent to which the extracted codes were captured with the ICF Generic Set and the ICF Core Set for Hand Conditions, we used the ICF linkage indicators (MacDermid, 2014). Using the recommended formulas, we calculated Core Set representation ([number of unique ICF codes from the measure that appear in the Core Set/total number of the codes in the Core Set] × 100%), and Core Set unique disability representation ([number of unique ICF codes from the measure that appear in the Core Set/total number of the disability codes in the Core Set] × 100%).
Two researchers (Maryam Farzad and Motahar Hemmati) independently extracted the first concept and additional concepts and linked them to the ICF categories. In case of ambiguity, a discussion among members of the research team was held to interpret and reveal any additional concepts.
Quantitative Analysis
We examined measures of central tendency and distribution (e.g., proportions, means) to describe our sample. We used bivariate Pearson correlation coefficients to describe the associations between COPM, PBQ, and PRWE scores. The strength of a correlation was categorized as low (r = .30–.50), moderate (r = .50–.70), or high positive (r = .70–.90; Mukaka, 2012). All of the analyses were done with IBM SPSS Statistics (Version 24), and statistical significance was defined using p < .05.
Results
A total of 120 patients completed the requested questionnaires and were interviewed. The cohort’s mean age was 46 (SD = 17), and 66% were male (Table 1). In total, 434 meaning units were extracted from the interview and COPM subscales. Axial coding led to 73 codes in different areas of functioning. The extracted meaning units were categorized as self-care (n = 15; 21%), leisure (n = 12; 16%), and productivity (n = 16; 22%) and were linked to 30 ICF categories. Thirty of the raised problems were coded as pain, sensation, and movements of the hand and wrist, which are not categorized by the ICF.
Patient and Clinical Characteristics
Note. COPM = Canadian Occupational Performance Measure; OT = occupational therapy; PBQ = participation behavior questionnaire; PRWE = Patient-Rated Wrist Evaluation; PT = physical therapy.
The extracted codes from the COPM were linked to 29 (73%) comprehensive and 8 (26%) brief ICF Core Set for Hand Conditions, and 1 was linked to the ICF Generic Core Set. D930: Religion and spirituality was reported by patients and was not included in either the brief or comprehensive Core Set for Hand Conditions. In other words, 100% of the extracted codes were linked to ICF categories. Thirty-eight extracted codes were linked to the ICF comprehensive hand core set, which represented a 32% comprehensive core set representation. Core set unique disability representation indicated that the patients reported issues in 30 out of 38 activity and participation categories of the comprehensive ICF core set (78%).
Most of the patients reported problems in three chapters of the ICF: (1) domestic life (n = 67, 55%); (2) community, social, and civic life (n = 64, 53%); and (3) major life area (n = 63, 52%). Domestic life was an important category reported by most patients with DRF 1 yr after the fracture. Their reported problems were linked to d620: Acquisition of goods and services, d630: Preparing meals, d640: Doing housework, d650: Caring for household objects, and d660: Assisting others. Based on the ICF definitions, these chapters cover different areas of functioning. Domestic life includes household cleaning and repairing, caring for personal and other household objects, and assisting others. Community, social, and civic life is about the actions and tasks required to engage in an organized social life outside the family, in community, social, and civic areas. Major life area refers to carrying out the tasks and actions required to engage in education, work, and employment and to conduct economic transactions.
Twenty-five codes were linked to Chapters d3, d4, and d5, which are suggested as representing activity limitations (Whiteneck & Dijkers, 2009), such as d360: Using communication devices and techniques (d3: Communication), d430: Lifting and carrying objects, d440: Fine hand use, d4401: Grasping, d4402: Manipulation, d4408: Turning or twisting the hands or arms, and d4458: Hand and arm use, other specified (d4: Mobility). These findings indicate that 34% of the extracted meaning units were related to activity limitations, fine hand use, and self-care. Forty of the extracted codes were linked to Chapters d6, d7, d8, and d9, which are considered as representing participation (Whiteneck & Dijkers, 2009), such as d660: Assisting others (d6: Domestic life) and d930: Religion and spirituality (d9: Community, social, and civic life). In other words, 54% of extracted problems were related to participation restriction. The most frequently described problems were related to patients’ performance (66%), not their capacity (34%).
Descriptive Quantitative Analyses
The mean PRWE score was 26.80 (SD = 23). In 1 yr after the DRF, 59 (49%) patients reported residual disability, and 43 (35%) reported persistent pain. The performance score was 7.64 (SD = 1.71), and the satisfaction score was 8.01 (SD = 1.66), indicating an acceptable level of occupational performance and satisfaction.
Table 2 shows the associations between the COPM and disability and participation in patients with DREs 1 yr after the fracture. A bivariate analysis indicated that occupational performance as measured by the COPM (r = .53) and satisfaction with performance (r = .62) were moderately correlated with participation as measured by the PBQ at the p < .001 level. Pain as measured by the PRWE was negatively correlated with satisfaction (r = –.54) and performance (r = –.48). Function as measured by PRWE was negatively correlated with performance (r = –.50) and satisfaction (r = –.62) as measured by the COPM. In other words, patients with a disability had lower performance and lower satisfaction with their performance. A greater level of occupational performance was significantly associated with a greater level of participation and satisfaction with performance. Participation as measured by PBQ had a medium negative correlation with pain intensity (r = –.42) and a moderate correlation with disability (r = –.50) as measured by the PRWE. A greater level of participation was significantly correlated with a lower level of pain intensity and disability (Table 3).
Linkage of the Problems Patients Raised in the Interviews and the Related Categories of the COPM With the ICF Core Set for Hand Conditions Categories
Note. Codes for three COPM subscales are as follows: SC = Self-Care (personal care, functional mobility, community management), P = Productivity (paid/unpaid work, household management, play/school), L = Leisure (quiet recreation, active recreation, socialization). COPM = Canadian Occupational Performance Measure; ICF = International Classification of Disability, Functioning and Health.
Correlation Between Different Patient-Reported Outcome Measures
Note. COPM = Canadian Occupational Performance Measure; PRWE = Patient-Rated Wrist Evaluation.
p ≤ .01.
Discussion
This study expands on prior studies that have found evidence that persistent disability exists after a DRF to elucidate the nature of these disabilities using a COPM and ICF framework and classification system. Patients reported problems related to their self-care, leisure, and productivity that were linked to different areas of functioning based on the ICF, such as mobility, assisting others, and spirituality. A small percentage of the patients (0.4%) reported problems performing religious and spirituality- related activities, which are not considered in the ICF Core Set for Hand Conditions. This study also determined that better occupational performance was correlated with a greater level of participation, less pain, and a lower level of disability.
We focused on patients who were 1 yr post DRF. The patients reported more difficulties in the areas of leisure and productivity 1 yr after the fracture; however, in the first stages of recovery they experienced more difficulties in self-care (Dekkers & Søballe, 2004). Five wk after a wrist fracture (Dekkers & Søballe, 2004), patients reported more challenges in their self-care than in other areas (self-care = 49%, productivity = 40%, leisure activities = 11%).
A comparison of the results of this study with those of previous reports of patients in the early stages after a fracture indicate that by overcoming the impairment (limited range of motion and strength), patients could perform their daily self-care activities more easily; however, they continue to report difficulties in the performance, work, and recreation domains of life that are most severely and continuously affected during their recovery 1 yr after a fracture (MacDermid et al., 2003). A scoping review on recovery after DRF showed that at 12 mo, the significant problems raised by patients were performing sports and leisure activities (38%; Halim & Weiss, 2016). Our findings also indicate that leisure and sports were challenging activities 1 yr after a fracture.
The most frequently reported issues in this study were doing housework, such as washing the dishes, tidying the yard, cleaning the house, using machines in the kitchen (e.g., a microwave), and disposing of garbage. A study that evaluated occupational performance in women with hand fractures showed that 78% of them reported problems in their ADLs 1 yr after the fracture (Nielsen & Dekkers, 2013). Despite the recovery in impairment limitations, such as muscle power and limited range of motion 1 yr after a wrist fracture, these findings show that patients report difficulty performing their daily activities, which should be considered when planning rehabilitation evaluation and interventions.
Our patients reported difficulties performing household activities and home chores (instrumental activities of daily living [IADLs]), such as opening a new jar or a tight-fitting lid with the affected hand, carrying a heavy object in the affected hand, and cutting meat using a knife with the affected hand 1 year after the DRF. Four other studies have discussed recovery in IADLs among clients with DRFs and indicated the same issues (Harris et al., 2005; Nielsen & Dekkers, 2013; Porter, 2013; Vergara et al., 2016). During the interviews, patients reported difficulties in communicating, assisting others, and activities related to their religion. These areas are like those reported by people with chronic conditions such as stroke, arthritis (Ewert et al., 2004), and multiple sclerosis (Johnson & Fraser, 2005; Khan & Pallant, 2007).
All the issues extracted from the COPM that were related to activity limitations were linked to ICF Chapter 4 (Mobility: d430: Lifting and carrying objects, d440: Fine hand use, d4401: Grasping, d4402: Manipulation, d4408: Turning or twisting the hands or arms, and d4458: Hand and arm use). The extracted content is covered by the Specific Activities subscale of the PRWE. A recent review also concluded that the functional problems reported by patients after a DRF are covered by PRWE (Halim et al., 2021).
Patients in our study also reported problems in the following areas: d7: Interpersonal interactions and relationships; d9: Community, social, and civic life; and d3: Communication. A qualitative study of people with a DRF with a mean time of 14 mo after the injury indicated that they reported issues in dealing with life situations, interpersonal relationships, and their social lives (Andreasson et al., 2020). These areas are related to life situations and can be considered participation; however, the boundary between the two dimensions of activity and participation in the ICF is unclear. In later phases after fractures, when an optimal range of motion has been gained, a person’s ability to participate in the usual activity and occupational performance is essential. Clinicians should include these considerations in their evaluations and implement strategies to improve occupational performance and participation (Goldhahn et al., 2014). Four items on the Specific Activities subscale of the PRWE ask about self-care, leisure, and productivity activities that can be considered participation restrictions (Farzad et al., 2020). However, the range of difficulties patients reported in the area of occupational performance and participation encompassed more than these four items. Other studies also have shown that participants report a wider variety of symptoms during an interview compared with when they are asked to complete a questionnaire (Gerber & Schraa, 1995; Homsi et al., 2006; Iverson et al., 2010).
A significant correlation between occupational performance as measured by the COPM and participation as measured by the PBQ confirms that the concept of occupational performance is similar to the concept of participation proposed by the ICF. That a higher level of occupational performance correlated with a lower level of disability as measured by the PRWE indicates that patients reported difficulties in their occupational performance despite displaying the capability to do tasks on the PRWE. Similar results were reported in a study conducted in Denmark that focused on the initial aftermath of an injury. A low correlation was reported between the COPM performance score and Disabilities of the Arm, Shoulder and Hand (DASH) score in a woman with hand fractures. (Dekkers & Nielsen, 2011). Because standardized items are consistent across patients, and the COPM captures the most relevant individualized items that vary across different people, a moderate correlation partially reflects this different structure. Another study reported that people with a DRF in the early stage have difficulty performing their usual activities as measured by the PRWE; however, 1 yr after a fracture they had difficulty performing specific activities (Harris et al., 2005). The Specific Activities subscale of the PRWE can be considered as assessing participation (Farzad et al., 2020) and should be administered separately, in the later phase of treatment.
Impairment is not a good indicator of functioning (Farzad et al., 2015; Harris et al., 2005). Physical impairment contributes to activity limitation; however, there is no direct relationship. In this study we confirmed that activity limitations as measured by the PRWE do not have a direct relation to participation as measured by the PBQ and performance as measured by the COPM. Levels of performance and participation are related to different personal and environmental factors. Commonly used PROMs often focus on activity restriction and impairment (Cantero-Téllez et al., 2019; Farzad et al., 2014; Imrie, 2004). Evaluation of functioning without considering participation cannot capture the complete picture of a person’s disability level (Farzad et al., 2014), which should be considered in evaluation and treatment.
The correlation between the objective parameter of the function (impairment) and subjective functional outcomes is controversial (Farzad et al., 2015; Karnezis et al., 2005; Young et al., 2003). Some studies have indicated that subjective parameters “pain” and “disability” are influenced by psychosocial factors and are less associated with objective parameters (Kwok et al., 2011). However, other studies have found a significant association between radiological outcomes and objective physical results or DASH scores. Some have reported a greater disability score in people with more complex fractures (Karnezis et al., 2005; Wilcke et al., 2007). The present study shows that pain, as measured by a subscale of PRWE as one indicator of impairment, is positively correlated with activity limitations (measured by the Specific Activities subscale of the PRWE) and negatively correlated with occupational performance and participation. One can conclude that the levels of occupational performance and participation are defined by factors other than symptoms and disability (Farzad et al., 2015). These findings further highlight the concept of perceived participation, which is not related to disability level (Cardol et al., 2002).
Our data are limited to recovery from disability among a population of patients with DRFs and cannot be generalized to other fracture or hand injury conditions. Because we focused on persistent limitations, our results do not reflect the disability experienced in the early phases of fracture healing and recovery. We also did not consider the side of the body the fracture was on, something that can be essential and affect the number of performance problems.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: One yr after a DRF, patients reported difficulties in occupational performance and participation despite improvement in PROM. Occupational therapists should consider occupation-based outcome measures in chronic stages of hand injuries. The COPM can be used as an outcome evaluation to get a better picture of patients’ occupational performance before discharge.
Conclusion
This research offers a comprehensive insight into the challenges faced by patients with DRF, even 1 yr postfracture. Although many ICF categories from the d chapters are relevant for these patients, leisure, domestic life (d6), and self-care (d5) are the predominant areas of difficulty. Using the COPM and interviews as assessment tools revealed a broader spectrum of occupational performance and participation issues than use of standardized outcome measures. A significant correlation was observed between patients’ pain levels, functional abilities, occupational performance, and satisfaction levels. Despite the advancements noted in PROMs, patients still grapple with specific occupational challenges. As such, for a holistic understanding and effective patient care, the emphasis should be on comprehensive, occupation-based outcome measures, especially in the chronic recovery stages of hand injuries.
Footnotes
Acknowledgments
Joy MacDermid was supported by a Canada Research Chair in Musculoskeletal Health Outcomes and Knowledge Translation and the Dr. James Roth Chair in Musculoskeletal Measurement and Knowledge Translation.