
Abstract
This article identifies the common assessment tools utilized by pediatric occupational therapists and brings awareness to the inconsistent identification and integration of occupation-based assessment tools within pediatric clinical practice.
The two primary cornerstones of the occupational therapy profession are (1) an understanding of the positive influence of occupation on one’s health and (2) the importance of the therapeutic use of occupation in clinical practice (American Occupational Therapy Association [AOTA], 2020; Wilcock & Hocking, 2015). The practical application of these foundational concepts has been termed occupation-based practice, defined as the ideal practice method in which the therapist promotes the client’s active participation in occupations during the process of evaluation and intervention (Fisher & Marterella, 2019). Although these ideals hold true for clients of all ages, they are particularly important for pediatric clients because children’s active engagement in occupations is integral to their development (Kreider et al., 2014).
Best practice for pediatric occupational therapists includes administering evaluations, developing an occupational profile, and analyzing occupational performance (AOTA, 2020). The practice of first gaining an understanding of the child as an occupational being and then measuring occupational performance and skills is considered a top-down approach (Case-Smith & O’Brien, 2015). Occupational therapists are uniquely trained to analyze clients by means of a top-down approach because of the profession’s focus on assessing clients’ performance of occupations holistically through activity analysis (AOTA, 2020). The incorporation of occupation into practice is unique to the profession and exemplifies its original foundation: that “man, through the use of hands as they are energized by his mind and will, can influence the state of his own health” (Reilly, 1962, p. 3).
These core occupational beliefs require that pediatric occupational therapists provide occupation-based services, beginning with the selection of occupation-based assessment tools to determine a child’s engagement in occupations. A variety of assessment tools are available for use in pediatric occupational therapy practice. Mulligan (2014) posited that pediatric occupational therapists must select assessment tools by considering their purpose; whether they are designed for the child’s age and abilities; their psychometric properties, including normative data characteristics, reliability, and validity; and pragmatic factors, including the length of time needed for administration, therapist competency, space, and cost.
Today, assessment tools are considered an essential component of the evaluation process because the information they provide is used to develop an occupational profile and identify limitations in areas of occupational performance (Hinojosa & Kramer, 2014; Schell et al., 2014). Assessments can include formal standardized assessments that measure the client’s performance on test items that are scored by the therapist according to the assessment guidelines or informal measures in which the therapist uses a given situation or skilled observation to obtain data (Schell et al., 2014). In addition, therapists should consider each tool’s occupation-centeredness; occupation-based assessments echo the profession’s occupational focus by incorporating occupation throughout service delivery, and they reflect a top-down approach (Case-Smith & O’Brien, 2015; Laverdure et al., 2019).
Despite the ideal use of a top-down approach and the profession’s movement toward occupation-centered practice, pediatric occupational therapists report minimal utilization of occupation-based tools (Bagatell et al., 2013; Kiraly-Alvarez, 2015; Mulligan, 2014). It is occupational therapists’ responsibility to recognize that “the presence, absence, or limitation of specific body functions and body structures does not necessarily determine a client’s success or difficulty with daily life occupations” (AOTA, 2020, p. 17). It is primarily through the process of assessing a client’s engagement in occupations that occupational therapists can determine the appropriate occupation-based interventions (AOTA, 2020). The prioritized placement of occupation is consistent with the global focus on occupation identified in the Centennial Vision, echoing occupational therapists’ responsibility to meet clients’ occupational needs (AOTA, 2017); the occupational renaissance embracing occupational therapists’ recapturing of the profession’s lost identity (Whiteford et al., 2000); and the emphasis on the profession’s occupational roots to consider clients as occupational beings (Molineux, 2004).
To ensure that the initial focus of the evaluation targets the quality and quantity of children’s engagement in occupation, best practice recommends the incorporation of occupation-based assessments (AOTA, 2015; Case-Smith & O’Brien, 2015). Definitions of occupation-based assessments and skill-based assessments are unavailable in current literature. For the purposes of this study, we defined occupation-based assessments as assessment tools that use a top-down approach, beginning with an analysis of the client’s interest in and ability to perform occupations; these assessment tools may specifically target occupations that are meaningful to the individual, their caregiver, or both. Conversely, we defined skill-based assessments as assessment tools that measure a client’s body functions, performance skills, or both using a bottom-up approach, beginning with an analysis of the client’s impairments and specific skills.
Several studies have explored selection and use of assessments in pediatric occupational therapy practice, but none have addressed the occupational nature of the tools. Lee et al. (2018) examined assessment tools selected by pediatric occupational therapists in South Korea and categorized them into 10 occupational therapy practice domains. Although they identified the assessment tools most commonly selected by therapists (N = 105) in South Korea, they did not classify the tools as occupation based or skill based (Lee et al., 2018). Peters et al. (2019) conducted a similar study specific to the pediatric occupational therapy assessment tools most commonly integrated in research studies, focusing on children with cerebral palsy. The assessments were not further categorized into occupation-based or skill-based measures and did not extend across all diagnoses (Peters et al., 2019). Despite occupational therapy’s focus on prioritizing occupation-based practice, evidence for the use of occupation-based assessments in pediatric occupational therapy practice is lacking.
The aims of this study were to identify the assessment tools most commonly selected by pediatric occupational therapists and to examine pediatric occupational therapists’ identification of assessment tools as occupation-based. We hypothesized that pediatric occupational therapists would most commonly select assessment tools that are skill based and that they would incorrectly classify these assessment tools as occupation based.
Method
A descriptive cross-sectional quantitative survey research design was used for the study as the participants were examined once to gain insight about which assessment tools are regularly administered by pediatric occupational therapists (Plichta & Kelvin, 2012). The study protocol was reviewed for adherence to ethical guidelines and protection of human participants and received IRB approval.
Participants
Participants were recruited through targeted sampling and represent pediatric occupational therapists with access to social media. Targeted sampling allowed us to exert greater control over the sample to directly access the specific population under study (Watters & Biernacki, 1989). The infographic invitation to participate included a hyperlink and was sent to pediatric occupational therapy groups through social media accounts, including two separate Facebook pediatric occupational therapist groups (https://www.facebook.com/groups/80351866792; https://www.facebook.com/groups/224107177618988) with, respectively, more than 44,400, members and 9,400 members; the School-Based Occupational and Physical Therapists group (https://www.facebook.com/groups/566673666831986), with roughly 25,300 members; and Research4OT (https://www.facebook.com/groups/610802762263474), with more than 6,800 members. Participants were included if they were occupational therapists practicing in pediatrics, as determined by their providing direct patient care to individuals ages 0 to 21 yr. Participants were excluded if they did not have experience providing direct occupational therapy services to pediatric clients. Additionally, occupational therapy assistants were excluded because the assessment tool selection process is typically determined by the supervising occupational therapist. To confirm their voluntary participation, individuals answered a multiple-choice question that was presented electronically. In total, 347 individuals confirmed their consent and clicked the hyperlink to the researcher-created inventory; 2 were unwilling to participate in the study, and 8 indicated that they were certified occupational therapy assistants. Thus, a total of 337 pediatric occupational therapy practitioners completed the inventory.
Data Collection Instrument
The quantitative data were collected by means of an inventory created using Google Forms (Google, 2020); password-protected software automatically gathered data and compiled the total number of participants. The inventory consisted of two sections. The first section asked about years of practice, entry-level occupational therapy degree, highest degree earned, primary practice setting, and geographical location. The AOTA 2019 Workforce and Salary Survey (AOTA, 2019) was used to identify primary practice settings relevant to pediatric occupational therapy. Participants responded to the geographical location item from a dropdown menu of choices that included all 53 U.S. states and territories as well as countries listed in the World Federation of Occupational Therapists (2023) accredited programs directory.
The second section of the inventory consisted of a list of pediatric occupational therapy assessment tools. To create this section, we performed a thorough review of the assessment tools included in the Asher (2014), Case-Smith and O’Brien (2015), Law et al. (2017), and Mulligan (2014) textbooks and selected those specific to pediatric occupational therapy. We then sent a list of these assessments to five experienced pediatric occupational therapy practitioners and academicians to ensure that regularly used pediatric occupational therapy assessment tools were included. Ultimately, 75 assessment tools were included in the inventory. Although not identified as such on the inventory, 20 assessments were noted to be occupation-based because they exemplified a top-down approach and captured occupations that are meaningful to the individual, caregivers, or both.
We classified an assessment as occupation-based if it was included in Mulligan’s (2014) list of occupation-based measurement tools. An additional 7 assessments were classified as occupation based because of their alignment with Fisher and Marterella’s (2019) definition of occupation-based practice and if the tool captured the performance of or interest in one or multiple occupations. To eliminate any bias, the assessments were presented in alphabetical order; a picture of the assessment was included to assist with identification. To promote clarity regarding the assessments included in the inventory, different versions of assessments were combined into one assessment prompt. For example, the Bruininks–Oseretsky Test of Motor Proficiency (BOT; Bruininks & Bruininks, 2005) and its second edition were presented in a single assessment prompt. The participants were asked whether they regularly used the identified assessment tool with the response options “yes” or “no.” The participants then selected whether they considered the selected assessment tool to be occupation based (“yes,” “no,” or “no exposure to tool for classification”). We collaboratively constructed the inventory; as noted earlier, it was reviewed by five experienced pediatric occupational therapy practitioners and academicians.
Data Analysis
The data were uploaded into IBM SPSS Statistics (Version 27) for analysis. Descriptive statistics were performed to indicate the years of practice, entry-level occupational therapy degree, highest earned degree, primary practice setting, and geographical location of the sample. Additionally, we calculated which pediatric occupational therapy assessment tools are most regularly used in clinical practice. First, all the assessments were ranked from most frequently used to least frequently used on the basis of the participants’ responses. Second, the occupation-based assessments were ranked from most to least frequently used. Next, the investigator (Alysha Skuthan) identified the number of occupation-based assessment tools selected by each participant and compiled a list of the assessment tools participants most commonly identified as occupation-based and those participants indicated they did not have exposure to, ranking them from least to most exposure. Then, the investigator compared the assessment tools selected by country of practice, years of practice, and across practice settings. Last, the investigator calculated the frequency with which occupation-based assessment tools were correctly identified as occupation-based and the frequency with which non-occupation-based assessment tools were incorrectly identified as occupation-based. Additionally, a nonparametric correlation was calculated of the participants’ correct identification of occupation-based assessment tools with the number of years in practice and the number of occupation-based tools used.
Mulligan (2014) identified 16 pediatric occupation-based assessment tools; we used these as a guide to identify the occupation-based assessment tools available for pediatric occupational therapists. After reviewing the assessments included in the inventory, we removed the Symbolic Play Checklist (Westby, 1980) because of its perceived lack of use in current clinical practice. Different versions of assessment tools were also combined into one item. Seven additional tools were considered to be occupation-based and were included as occupation-based tools. In total, 20 assessment tools were considered to be occupation-based, and we created an occupation-based assessment variable for relative comparison and nonparametric correlation.
Results
The demographic characteristics of the 337 participants who completed the inventory are included in Table 1. Almost half (44%) of participants had practiced for more than 10 yr, and almost a quarter (23%) had practiced for 1 to 3 yr. Additionally, most participants practiced in schools (42%) or in free-standing outpatient clinics (30%). The most commonly selected assessment tools in each practice setting are presented in Table 2. The percentage of participants who selected each assessment tool is included in Table 3. Therapists indicated that they used a variety of assessment tools, with some using a limited number of tools and others using many different assessment tools. The most commonly selected assessment tool was the Sensory Profile (86.4%), followed by the Beery–Buktenica Developmental Test of Visual–Motor Integration (Beery™ VMI; 85.2%). Four of the 11 most used assessment tools are considered to be occupation-based. We created a variable to examine the number of occupation-based assessment tools used by each participant. The number of commonly used occupation-based assessments is depicted in Figure 1. Most participants (84.3%) identified using one or more occupation-based assessment tool.
Demographic Characteristics of the Participants (N = 337)
Note. The participants for the study practiced in 46 of the 50 US states. The states with the greatest number of participants were California (n = 27) and New York and Texas (n = 22 for each).
Most Commonly Selected Assessment Tools by Practice Setting (N = 337)
Note. Boldface indicates an occupation-based tool. Beery® VMI = Beery–Buktenica Developmental Test of Visual–Motor Integration; BOT = Bruininks–Oseretsky Test of Motor Proficiency; DTVP = Developmental Test of Visual Perception; M–FUN = Miller Function and Participation Scales; PDMS = Peabody Developmental Motor Scales; PEDI = Pediatric Evaluation of Disability Inventory; SPM = Sensory Processing Measure.
Percentage of Participants Who Selected Each Assessment Tool and Classification of Tools as Occupation-Based (N = 337)
Note. Boldface indicates an occupation-based tool.
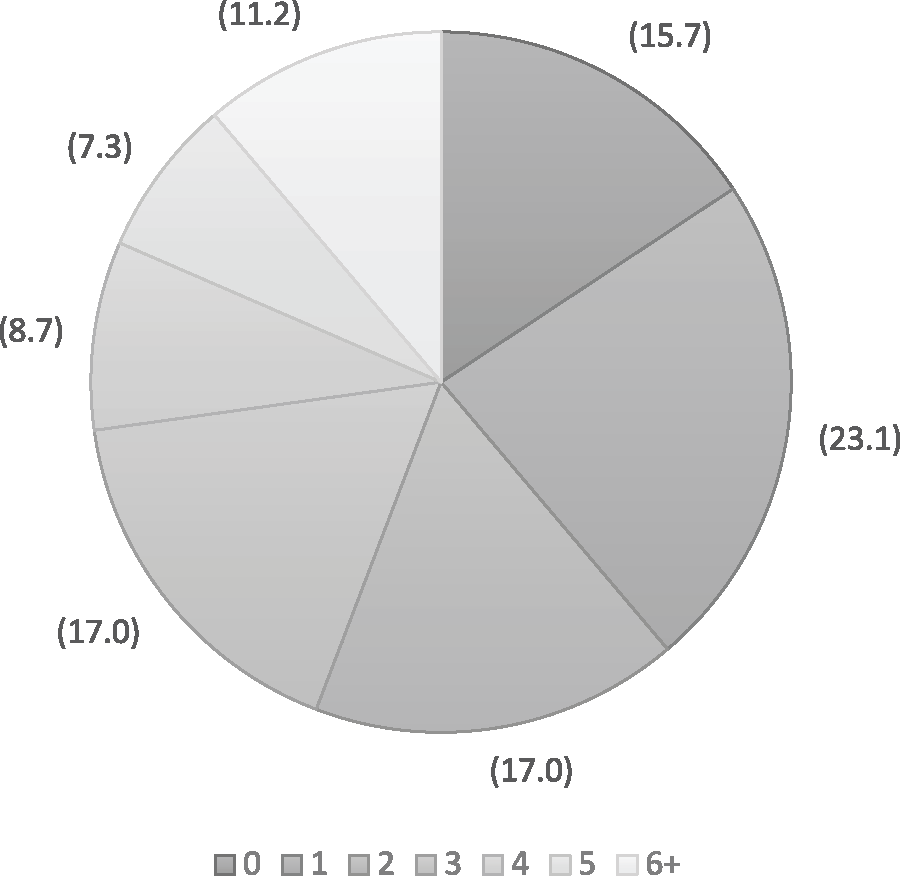
Percentage of participants’ selection of occupation-based assessments.
Additionally, participants identified whether they considered the assessment tools to be occupation-based or non–occupation-based or whether they had no exposure to the tool to be able to classify it (see Table 3). The results showed when an occupation-based tool was not identified as such and when a tool was identified as occupation-based when it was not. A low percentage of “yes” responses for an occupation-based tool indicates that participants did not recognize the tool as occupation-based. A high percentage of “yes” responses for a non–occupation-based tool indicates that participants misidentified the tool as occupation-based. Notably, the top two assessments participants indicated as occupation-based were the Sensory Profile (77.4%) and the Peabody Developmental Motor Scales (69.1%). Neither is considered to be occupation-based; rather, they are considered to be skill-based. In total, more than 90% of participants identified having no exposure to 30 of 75 presented assessments.
One participant correctly labeled all 20 occupation-based assessments as occupation-based, and 10 participants identified none of the occupation-based assessments correctly. A mean of 5.93 assessment tools were correctly labeled as occupation-based. Participants commonly misidentified skill-based assessment tools as occupation-based; the highest number of incorrectly identified assessments was 27.0. Eight participants accurately identified all non–occupation-based assessment tools as non–occupation-based. A mean of 6.53 assessment tools were misidentified as occupation-based.
Of the 20 assessment tools identified as occupation-based, the Miller Function and Participation Scales (Miller, 2006) was used by 30.6% of participants; the Print Tool (Olsen & Knapton, 2016), by 30.6%; the Pediatric Evaluation of Disability Inventory (Haley et al., 1992), by 30.3%; and the School Function Assessment (Coster et al., 1998), by 30.0%. Fewer than 30.0% identified using each of the other occupation-based assessment tools, indicating a significant lack of occupation-based assessment tools administered in clinical practice. The five assessments that participants most commonly identified as occupation-based were the Sensory Profile, Peabody Developmental Motor Scales, Canadian Occupational Performance Measure (Law et al., 2019), Sensory Processing Measure (Parham et al., 2007), and the BOT. Of these, only the Canadian Occupational Performance Measure is occupation-based, and 59.9% of participants correctly identified this measure as such.
An analysis of the relationship between years of practice and percentage of correctly identified occupation-based tools revealed no association (r s = .022). Additionally, we found no relationship between the percentage of accurately identified occupation-based tools and the number of occupation-based tools used (r = −.248).
Discussion
The results include information related to the participants’ demographic characteristics and identification of commonly selected pediatric occupational therapy assessment tools. Notably, pediatric occupational therapists most commonly identified using the Sensory Profile (Dunn, 1999), Beery VMI (Beery & Beery, 2006), Peabody Developmental Motor Scales (Folio & Fewell, 2000), and the BOT. All four of these assessments are considered to be skill-based; that is, the child is assessed on specific skills rather than the performance of occupations. The primary assessment tool selected was skill-based regardless of the participant’s years of practice or practice setting, indicating a lack of utilization of occupation-based assessment tools in clinical practice. Years of experience may not be a factor contributing to the selection of occupation-based assessments because new graduates are trained in the selection and administration of assessments by their fieldwork educators. Experienced therapists are habituated to the use of skill-based assessments because of reimbursement expectations, familiarity with skill-based assessments, or both. Therefore, newer graduates may not administer occupation-based assessments as a result of their fieldwork educators’ experience or expectations. They may also take on the skill-based culture of the clinic where they did their fieldwork.
Occupational therapists have the unique opportunity to shift the focus from skill-based deficits to occupational constructs through the selection of occupation-based assessment tools to initiate services that are uniquely occupational. Occupational therapists must advocate with third-party payers for the importance, relevance, and value of occupation-based assessments to set the stage for services that are not redundant with those of other providers. Practitioners should further advocate with management and employers to obtain occupation-based assessments and educate recipients of services about focusing care on the child’s occupational needs. The common use of skill-based assessments further compounds the misrepresentation of the scope of pediatric occupational therapy practice by focusing the assessment process on performance skills, which is not unique to the profession of occupational therapy.
When we looked specifically at occupation-based assessment tools, participants indicated infrequent use of occupation-based tools and a limited recognition of which tools are occupation-based. It is possible that participants used few occupation-based assessment tools but frequently used the same occupation-based assessment tool. Moreover, participants may have relied on an occupational profile as opposed to an assessment tool. In total, 15.7% of participants reported that they did not use occupation-based assessment tools, and 23.1% indicated that they used one occupation-based assessment tool.
A surprising number of pediatric occupational therapists incorrectly classified available assessment tools as occupation-based instead of skill-based. When therapists use skill-based assessments rather than occupation-based assessments, those skills may be misinterpreted as occupations, contributing to confusion among recipients of services and members of the interdisciplinary team regarding the scope of occupation in pediatric occupational therapy practice. A profession-wide classification of assessment tools may be beneficial to guide therapists during the assessment tool selection process to ensure incorporation of occupation-based assessment tools and creation of occupation-based goals that reflect occupation-based practice.
The results of this study aid in filling gaps in the literature and contradict certain findings detailing practice trends and progression. Assessment tools are vital to the evaluation process (Hinojosa & Kramer, 2014; Mulligan, 2014; Schell et al., 2014) and are intended to reflect an occupation-based approach (AOTA, 2015; Case-Smith & O’Brien 2015; Laverdure et al., 2019). The available literature does not conclusively identify a common assessment tool used by pediatric occupational therapists in the United States across all diagnoses. Peters et al. (2019) indicated that the Assisting Hand Assessment (Krumlinde-Sundholm et al., 2007) and the Pediatric Evaluation of Disability Inventory (Haley et al., 1992) were most commonly selected when working with children with cerebral palsy. Additionally, Lee et al. (2018) identified that the most common assessment tools used by pediatric occupational therapists in Korea—the Canadian Occupational Performance Measure, Wee Functional Independence Measure (Slomine, 2011), School Function Assessment (Coster et al., 1998), Knox Preschool Play Scale (Knox, 2008), Developmental Test of Visual Perception (Hammill et al., 1993), BOT (Bruininks & Bruininks, 2005), Evaluation of Social Interaction (Fisher & Griswold, 2008), and Denver Developmental Screening Test (Frankenburg & Dodds, 1967; Lee et al., 2018)—are reflective of specific practice domains. We found that the Sensory Profile (Dunn, 1999) and the Beery VMI (Beery & Beery, 2006) were the assessments most commonly selected by pediatric occupational therapists. Notably, both of these assessment tools are classified as skill-based. The literature supports the profession’s shift toward occupation or the top-down evaluation process (Case-Smith & O’Brien, 2015; Whitney & Hilton, 2013) and a shift away from the developmental assessment roots of the profession or a bottom-up approach; however, the results of this study suggest that pediatric occupational therapy practitioners have not yet made this change in the clinic.
Limitations
A limitation to this study is that therapists may simply select assessment tools that are available in their practice setting and are not indicative of their knowledge of or preference for other assessment tools.
Implications for Occupational Therapy Education
The results of this study can be applied to the didactic phase of learning and clinical fieldwork opportunities. During the didactic phase, educators have the responsibility to follow the Accreditation Council for Occupational Therapy Education (ACOTE®; 2018) standards, which detail the necessary information students must learn to become occupational therapists. Although the ACOTE standards for occupational therapists include education related to assessments and theoretical foundations, it can be difficult for new graduates to apply these standards when practicing therapists do not demonstrate the most updated approaches. Revisions to the ACOTE standards that incorporate the differences between skill-based and occupation-based assessments and the importance of occupation-based assessments are needed.
It may be beneficial for fieldwork educators to collaborate with local clinics and facilities so that their practice reflects the most updated ACOTE (2018) standards. Further collaboration among educators in the classroom, fieldwork clinics, and regulatory agencies is imperative for the success of the profession and occupational therapists’ unique responsibility to improve occupational performance. In the lab and in the classroom, educators can create assignments that highlight the value and unique scope of occupational therapy practice through work such as that of Hooper et al. (2015), who examined the core subject of occupation and the key need for educators to incorporate and reflect occupation in the teaching and learning environments. Educators can guide the class to reflect on the client as an occupational being and on how occupation-based assessments provide the opportunity to integrate occupation into each facet of practice. Furthermore, fieldwork educators can create assignments that incorporate occupation, such as creating client-centered treatment plans, writing occupation-centered goals, or even reviewing available evidence that reflects occupation-centered practice.
Implications for Occupational Therapy Practice
Pediatric occupational therapy clinical practice should begin with the development of a client’s occupational profile followed by the selection of assessment tools relevant to the client’s specific needs. The results of this study indicate that pediatric occupational therapists most commonly use skill-based assessments and have difficulty identifying which are occupation-based versus skill-based. Pediatric occupational therapists must take ownership of and responsibility for their practice delivery, beginning with the selection of assessment tools that reflect occupation and aligning these assessment tools with occupation-centered theoretical foundations.
Pediatric occupational therapists must increase their awareness of the theoretical framework they are using throughout delivery of services. When therapists use only the developmental frame of reference (Creek, 2014), occupation is no longer the focus, and developmental milestones or skill mastery may instead take precedence. Therapists must combine the developmental frame of reference (Creek, 2014) with occupational models such as the Person–Environment–Occupation model (Law et al., 1996) and evidence-based practice to best capture a child’s occupational skills. Pediatric occupational therapists may possibly need a new framework that focuses on occupation in each facet of pediatric occupational therapy service delivery and reflects available occupation-based assessment tools. A framework such as the Dynamic Model of Occupation-Based Practice (Psillas & Stav, 2021) supports a practice that reflects the occupational nature of each therapeutic interaction by guiding professional reasoning around the constructs of occupation, meaningful and purposeful value, therapeutic intent, and engaged participation. Additionally, the associated Occupation-Based Practice Assessment (Stav et al., 2022) includes a scale to measure the occupation-centeredness of assessment tools. This scale quantifies the occupational focus to allow therapists and administrators to make informed choices when purchasing and selecting assessment tools.
This study has the following implications for occupational therapy practice: ▪ Pediatric occupational therapists are responsible for assessing a client’s occupational needs, not only developmental milestones. ▪ Pediatric occupational therapists must understand the occupational nature of assessment tools and select occupation-based assessment tools to uphold the foundational constructs of the profession.
Conclusion
This study identifies the tools most commonly selected by pediatric occupational therapists and provides insight into participants’ ability to identify tools as occupation-based. The participants most commonly used skill-based assessment tools and labeled such tools as occupation-based. No significant relationship was found between years of practice and the percentage of correctly identified occupation-based tools or between the percentage of tools accurately identified as occupation-based and the number of occupation-based tools. Analysis of how and why pediatric occupational therapists are not yet adopting the available evidence related to occupation-based assessment tools in their practice is needed.
Footnotes
Acknowledgments
We acknowledge the contribution and mentorship of the other committee members, Elise Bloch, EdD, OT/L, and Donna Colaianni, PhD, OTR/L, CHT.