
Abstract
Parent-provided, daily, early intensive bimanual stimulation (BB–Bim) at home is feasible when parents are coached weekly by an occupational therapist. BB–Bim seems to improve functional interactions between the hands among infants at high risk of unilateral cerebral palsy.
Children with cerebral palsy (CP) reach 90% of their potential gross motor abilities around age 5 yr, or even earlier if the child has severe CP (Rosenbaum et al., 2003). The development of manual function, as measured by the Assisting Hand Assessment, has already been described for children with unilateral CP ages 18 mo to 12 yr (Nordstrand et al., 2016), with variations depending on the severity of the initial damage. It seems that most children reach a plateau phase by age 3 yr. More recently, the development of hand function during the first year of life in children with unilateral CP was described through use of the Hand Assessment in Infants (HAI; Sakzewski et al., 2019), showing three trajectories of hand function development depending on the initial HAI score. The HAI was also used to describe developmental curves in typically developing children (Krumlinde-Sundholm et al., 2017), showing that bimanual hand use increases rapidly and that hand use is symmetrical in most children (Ek et al., 2019). These results can now be used to identify infants with atypical hand use, especially those with suspected unilateral CP.
The first year of life is a critical period for providing interventions that target hand motor development. For children with unilateral neonatal brain injury, promoting activity of the affected hand during this period is suggested to be more effective than at a later age (Basu, 2014). However, intervention programs specifically aimed at the development of manual function remain rare (Novak et al., 2020; Spittle et al., 2015). Constraint-induced therapy (Eliasson et al., 2018) and complex programs that stimulate development along different axes, including manual stimulation, appear promising (Holmström et al., 2019; Morgan et al., 2016); however, it is difficult to measure their impact (Löwing et al., 2020; Nordstrand et al., 2015). Indeed, the children at risk of CP included in these studies are very heterogenous, and it is not possible to perfectly predict the risk of CP or the spontaneous evolution of the children. Moreover, the fast rate of development during the first 2 yr increases the difficulty of identifying whether changes result from the treatments.
The latest consensus in clinical practice guidelines for early intervention with infants at high risk of neurodevelopmental disorders (Hutchon et al., 2019), or specifically of CP (Morgan et al., 2021), emphasizes the importance of an enriched environment (Morgan et al., 2013) and parenting support for appropriate, responsive, and resilient parenting (Basu et al., 2018). In addition, a systematic review (Novak et al., 2020) summarizing the effectiveness of therapies delivered to children with CP suggests that intensive interventions, as well as interventions centered on personalized objectives at home, may improve outcomes. These elements are concordant and favor intensive therapies that could be proposed for infants with unilateral CP in their familiar environment. Eckberg Zylstra and Sidhu (2021) report that the use of a caregiver coaching model for the implementation of intensive motor training for a child with unilateral CP improved both child performance outcomes and scores on parent satisfaction measures. There is a real need to bring the family to the center of early intervention practice and to build up their individual capacity to promote their infant’s development (Elenko, 2021).
We thus developed a program called BB–Bim, which is a new, home-based approach in which parents are coached and empowered to provide early, intensive, daily bimanual stimulation through play sessions. The need for this study relates to the lack of literature on bimanual programs for infants with unilateral CP that can be implemented to support parents as caregivers in the child’s natural environment.
The aim of this study was to measure the feasibility of BB–Bim and its impact on hand function in infants with unilateral brain injury and underuse of one hand.
Method
Design
This single-case experimental design (SCED; Krasny-Pacini & Evans, 2018; Romeiser-Logan et al., 2017) was a multiple baseline design across participants, or a multiple AB design, in which A was a baseline phase and B was the 8-wk BB–Bim intervention phase. The duration of the baseline phase was randomized at inclusion and was between 4 and 7 wk. The study flowchart is presented in Figure A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Participants
Inclusion criteria were infants ages 3 to 12 mo at the time of inclusion, with a unilateral brain lesion documented by brain imaging at birth or at the time of initial parental concerns and with underuse of one hand reported by the parents and quantified by the HAI. At least one parent had to be willing to actively participate in providing BB–Bim, and the family had to live within an acceptable distance of the assessment center from which the occupational therapist (Rachel Bard-Pondarré) conducted visits. Infants were not eligible if they had a lack of interest in objects, suggestive of associated autism disorders, which would influence bimanual exploration. Epilepsy uncontrolled by medication was also an exclusion criterion, because it would be a major bias if the child was not sufficiently alert for the stimulation. The BB–Bim team informed all child neurologists in the area about the ongoing project. They identified and approached the parents of potential participants, providing flyers and information sheets. With parental consent, contact details were forwarded to the BB–Bim team, and the family was screened for eligibility through a combined assessment visit (medical doctor and occupational therapist). If eligible, fully informed, written parental consent was obtained, as well as specific consent for image rights. Six infants were included.
BB–Bim Intervention
The parents were taught and encouraged to provide bimanual stimulation for 20 min/day, 6 days/wk for 8 wk. The stimulation involved a play-based activity with toys chosen to elicit the use of both the impaired and the unimpaired upper limbs during bimanual activities. Children’s interests, motivation, and cognitive and perceptual capacities develop during the first year of life and must be considered when selecting toys and tasks to promote bimanual skills. The toys were thus initially selected by the therapist and the parents and updated during the program if necessary to ensure that they still presented engaging properties and provided the right challenge according to the child’s development and level of ability. The stimulation dose did not need to be administered in a single session but could be spread out over the day. The exact duration could vary according to the family routine and occupations. During stimulation, the infant had to be positioned as upright and stable as possible to facilitate goal-directed arm movements with the attention focused on the play situation. Parents were supported by weekly home coaching visits from the occupational therapist, and they were asked to keep a written logbook to record the stimulation sessions they performed.
Assessments
Assessments were performed at each weekly occupational therapy visit. The study flowchart presented in the Supplemental Figure A.1 shows the assessment schedule.
The feasibility and relevance of BB–Bim were assessed by the number and length of stimulation sessions documented by the parents in the logbook and by a parental questionnaire completed at the final visit. The questionnaire consisted of 10 questions asking about the home setting feasibility of the stimulation, the relevance of the intensity and duration of BB–Bim, satisfaction with the therapeutic coaching and support, perception of self-competency and parents’ perception of BB–Bim efficacy. Responses were rated on a continuous scale ranging from 0 (not at all) to 10 (yes, perfectly).
The HAI (Ek et al., 2019; Krumlinde-Sundholm et al., 2017) was performed weekly by the occupational therapist to assess the quality of goal-directed uni- and bimanual actions. The HAI, developed with a Rasch model analysis, consists of a 10- to 15-min semistructured play session, which is video recorded. Seventeen items are rated on a 3-point scale (0 = no performance, 1 = ineffective performance, and 2 = effective performance) based on the manual abilities of each hand separately (12 items; raw score range = 0–24 for each hand) and bimanual hand use (5 items), The final sum score, ranging from 0 to 50, is converted on a scale ranging from 0 to 100 units, with higher scores representing better hand function. An asymmetry score is also generated. The HAI has good to excellent interrater and test–retest reliability (Ullenhag et al., 2021), with intraclass correlation coefficients of .96 to .99, and low smallest detectable differences: 2 points for the Each Hand measure and 3 points for the Both Hands measure.
Goals were defined with Goal Attainment Scaling (GAS; Krasny-Pacini et al., 2013, 2016) at the time of inclusion and were reassessed weekly. Goals had to specifically concern the use of upper limb motor skills in concrete situations of daily life (e.g., holding a bottle, taking off socks, taking out or putting in a pacifier, holding a biscuit) in which the parents had clearly noted an asymmetry of use between the upper limbs. The final score was expressed on a 5-point ordinal scale, ranging from −2 to and +2, and the three- milestones GAS methodology was used. This explicitly describes the initial (−2) level, the expected (0) level, and the most favorable (+2) level, whereas intermediate points (–1) and (+1) are implicit.
Accelerometry was also used to quantify the movement of both upper limbs. Two lightweight three-axis wireless accelerometers (Axivity AX3, Axivity, Newcastle upon Tyne, United Kingdom) were secured to the infant’s wrists using a soft, custom-made bracelet. The results of the accelerometry analysis will be reported separately.
Data Analysis
Clinical and sociodemographic data are presented individually. Descriptive statistics, including means and standard deviations, were used to describe the results of the parent questionnaire.
An important part of SCED data analysis is the graphical analysis (Krasny-Pacini & Evans, 2018; Romeiser-Logan et al., 2017). Data for each criterion were plotted for each infant. Level lines (median) and trend lines (linear regression fit) were plotted for each phase, as well as the band representing the minimum and maximum of the baseline phase (to visualize overlap).
For the continuous variables (i.e., the different HAI scales), the stimulation effect was statistically investigated using a hierarchical segmented linear model, which allows for both the level and the trend effect. As data increments vary from one participant to another, a random slope (in the sense of the hierarchical model) is fitted. To avoid adjustment problems, outliers were not used in this analysis. Outliers are defined as points that are more than 2 standard deviations from the phase mean. This model tests whether there is a trend and whether the stimulation affects this trend or the level. Infants whose development was rapid and joined the normative curve during the baseline phase were not included in the stimulation effect analysis.
For GAS scores, the difference between Phase A and Phase B was calculated for each infant with the τ-U summary index (Parker et al., 2011).
A significance level of 5% was set for all analyses. Statistical analyses were performed with R software (Version 4.0.5).
Results
Enrollment started in May 2021 and was completed in January 2022. All 6 infants had experienced a perinatal stroke (Chabrier et al., 2021; Kirton, 2013), either an arterial ischemic stroke (n = 3) or a fetal periventricular venous infarction (n = 3). Figure A.2 in the Supplemental Material presents the inclusion flow diagram, and Table 1 shows the demographic and clinical characteristics of the 6 infants, the randomized duration of the baseline phase for each, and the significant target activity defined by the parents and delineated in the GAS.
Demographic and Clinical Characteristics of the 6 Infants Included in the BB–Bim Study
Note. BB–Bim = early bimanual parent-provided stimulation; HAI = Hand Assessment in Infants; PAIS = perinatal arterial ischemic stroke; PVI = periventricular venous infarction.
Feasibility and Relevance of the BB–Bim Program
Parents provided a mean of 3.4 to 6.2 of the 6 required stimulation sessions per week and rated the BB–Bim program as highly feasible (M = 8.2, SD = 1.3) and relevant in terms of intensity (M = 8.9, SD = 0.9), duration (M = 8.9, SD = 0.9), and therapeutic support (M = 9.6, SD = 0.2). They appreciated their active role (M = 8.6, SD = 1.2) and felt competent to perform BB–Bim (M = 8.6, SD = 1.2). Parents also reported a positive impact of the BB–Bim program on their child, with mean effectiveness rated 9.2 (SD = 0.6), and an increase in the amount of affected upper limb movement (M = 9.5, SD = 0.5) and use (M = 9.4, SD = 0.5). The details of these results are presented in the Supplemental Figure A.3, which shows both the compliance with the program (number of stimulation sessions performed) and the results of the parents’ perception report at the end of the BB–Bim program.
Impact of the BB–Bim Program on Upper Limb Use
Figure 1 shows plots of the change in HAI unilateral and total scores for each infant against the HAI normative curves (available until only 10 mo of age). For all infants, the change in preferred-hand unilateral score appears normal. BB2’s nonpreferred hand curve joins the normative curve very quickly, as does the HAI total score; thus, these data were not used to analyze the impact of the BB–Bim program.
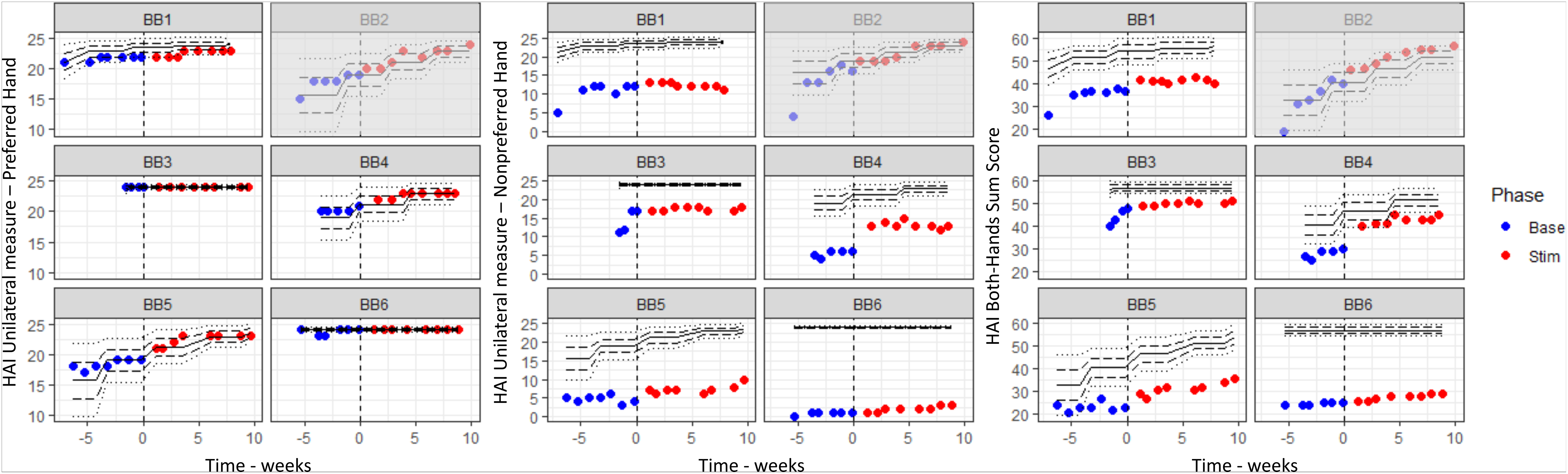
Plots of the change in HAI scores for each infant against the HAI normative curves: the preferred-hand unilateral score, the nonpreferred-hand unilateral score, and the both-hands total score.
The results of the regression model are presented in Table 2 for all HAI variables of the 5 infants analyzed. The regression model analysis shows a significant positive trend during baseline for the preferred hand, but no significant additional effect of the stimulation on the level (Phase B level) or the trend (Phase B tendency). For the nonpreferred hand unilateral score and the HAI asymmetry index, there was no significant effect of the stimulation. The stimulation resulted in a statistically significantly improvement in HAI bimanual and total score, which includes bimanual items. This can be visualized in the graphs of Figure 2, where the range of values of the baseline phase is projected to show the extent to which the points of the stimulation phase overlap (or not) with the points of the baseline phase. Figure 2 also presents the change in GAS scores, with a baseline naturally at −2 evolving positively with time and stimulation. The change was significant for 3 of the 5 infants included in the analysis, as shown by the τ-U calculations presented in Table 3.
Results of the Regression Model for HAI Scores
Note. df = degrees of freedom; HAI = Hand Assessment in Infants.
*p < .05. **p < .005. ***p < .0005.
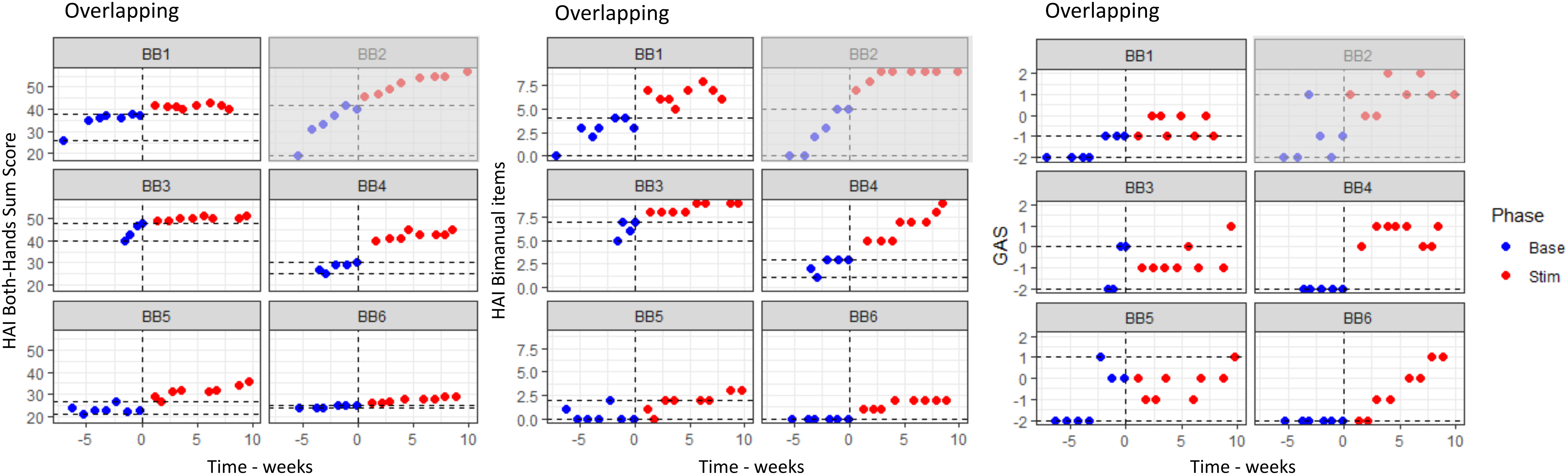
Plots of the change in and overlapping of HAI both hands sum score, HAI bimanual items, and GAS score.
Results of τ-U (Without Trend Correction) for the GAS Scores of the 5 Infants Included in the Analysis
Note. GAS = Goal Attainment Scaling.
*p < .05. **p < .005.
Discussion
This study is the first to evaluate a new, home-based, early intensive bimanual stimulation program. The SCED design enabled individual consideration of participants while providing evidence for both the intervention’s feasibility and its impact on bimanual function in infants with unilateral CP.
The BB–Bim intervention, which includes 8 wk of parent-provided stimulation, was reported by parents to be highly feasible, although some did not meet the study’s target criteria of six weekly stimulation sessions. Parents mainly felt competent to perform the stimulation and sufficiently supported by the therapist. The count of training hours was difficult because parents did not always stimulate their child in a specific session but rather throughout the day when interacting. This was one of the reasons that we chose to have parents perform the stimulation, to maintain intensity and maximize self-initiated activity in the everyday environment. This method of providing stimulation through pervasive changes to everyday activities may be more deliverable than therapy blocks with regard to infant lifestyle and attention span, as highlighted by Basu et al. (2017). Another reason was to empower the parents and support that fact that parents know their child best, that they were in charge, and that they were competent. Self-efficacy should be a key element of interventions addressed to parents of children with CP to elicit a process of empowerment that can improve the well-being of the family as a whole (Guillamón et al., 2013). All parents appreciated taking an active part in the program and found it effective in improving upper limb movements and functional use. This positive outcome may have been influenced by the weekly visit from the therapist, who empowered, motivated, and supported families to deliver appropriate and effective stimulation while keeping a balance with other occupations to avoid overburdening the parents.
The positive impact of the BB–Bim intervention on bimanual function was not only perceived by the parents but was also objectively measured with the HAI and GAS. A positive change in specific bimanual activities (expressed by GAS scores) as well as the HAI bimanual items and consequently the HAI total score was found for all the infants (whatever their age or HAI level at inclusion) as an effect of the intervention. This suggests that the bimanual stimulation was well targeted. Furthermore, even the babies who were more severely affected showed an improvement, similar to the Small Step Program (Holmström et al., 2019), which is especially encouraging because children with severe impairment often progress little in the first year (Eliasson et al., 2018; Morgan et al., 2016; Sakzewski et al., 2019). In contrast, the stimulation program did not affect the nonpreferred hand alone or the asymmetry of use between the hands. All infants increased the use of their affected hand, but we could not link this to the introduction of the intervention. This finding may suggest, in contrast with the conclusions of Löwing et al. (2020) regarding hand function, that BB–Bim participants did learn what they practiced: Bimanual stimulation improves bimanual interactions, whereas for babies modified constraint-induced therapy improves only the affected hand score (Eliasson et al., 2018).
Even if bimanual function improved for all infants during the study as shown by the HAI total score, the scores only joined the normative developmental curve for 1 infant. This was not a complete surprise because available developmental curves of hand function for infants with unilateral CP indicate three different main trajectories depending on the initial level, with greater distinctions between groups with increasing age; and even the high group trajectory does not join the normal developmental curve (Sakzewski et al., 2019).
The study limitations may partly explain the lack of an obvious link between improvements and the introduction of the intervention. We chose to include at least four measurement timepoints in the baseline phase and to randomize the duration of the baseline phase up to 7 wk to strengthen the study design and draw clearer conclusions. However, some parents began to provide informal stimulation as soon as they were included in the study; therefore, there may have been no real baseline phase. This behavior is understandable, because the parents read the information leaflet about the study and discussed the value of stimulation with the therapist, and the therapist came to their home once a week to administer the HAI. Several parents reported in informal interviews that during this phase they implemented repetitive stimulations in their daily routine. Therefore, this study should be replicated with a shorter baseline phase to avoid such bias.
The results of GAS are difficult to interpret for two reasons. First, the act of setting goals could have motivated the parents to start training toward them in the baseline phase. Second, it is difficult to distinguish whether the results arise from training toward a goal or the bimanual stimulation itself. This bias could have been evaluated by the inclusion of control goals relating to functions not trained by BB–Bim. The lack of examiner blinding and the lack of intervention reliability testing may also be limitations of this study, although the logbooks and weekly visits provided some procedural validity.
These first results are important for the future implementation of such an intervention in clinical practice, particularly given that upper extremity training outcomes do not differ according to whether parents or therapists provide training, if parents receive sufficient training and support (Rostami & Malamiri, 2012). Parents are able to provide relevant and intensive bimanual stimulation when coached weekly by a therapist at home, and this appears to improve bimanual function.
Implications for Occupational Therapy Practice
This single-case experimental design study focused on the feasibility of a new home-based bimanual stimulation program for babies with unilateral brain lesions and the effects on bimanual function as measured with the HAI. The results have the following implications for occupational therapy practice: ▪ Parents are willing to provide bimanual stimulation in their own environment on a daily basis when guided by an occupational therapist through weekly visits. ▪ Early bimanual stimulation can help babies develop their bimanual skills ▪ Occupational therapists should be trained to coach parents to help them find their own way of providing stimulation in their daily occupations.
Conclusion
This study supports the feasibility and the value of parent-provided, early bimanual stimulation for children with unilateral brain lesions. The implementation of BB–Bim in clinical practice as part of a complete interventional program following clinical guidelines for early intervention for children with, or at high risk of, CP (Morgan et al., 2021) is promising. Further exploration could focus on the effectiveness of BB–Bim in infants with bilateral brain lesions.
Supplemental Material
Supplementary material for Early Intensive Bimanual Stimulation Program (BB-Bim) for Infants at Risk of Unilateral Cerebral Palsy: A Randomized, Multiple-Baseline, Single-Case Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050232.pdf for Early Intensive Bimanual Stimulation Program (BB-Bim) for Infants at Risk of Unilateral Cerebral Palsy: A Randomized, Multiple-Baseline, Single-Case Study by Rachel Bard-Pondarré, Carole Vuillerot, Nahime Al-Abiad, Stéphane Verdun, Stéphane Chabrier and Emmanuelle Chaléat-Valayer in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We express our deepest gratitude to the children and their families participating in this study. We also warmly thank Béatrice Bertrand, who showed a great interest in this project and highly contributed to make it happen, and Eric Chabanat for his expert eye on the single-case experimental design and analysis. The study was approved by the ethics committee “Comité de Protection des Personnes Sud-Méditerranée I” in May 2021 and registered on ![]() with the identifier NCT04899284.
with the identifier NCT04899284.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.