
Abstract
This study identifies differences in sensory processing between patients with a primary diagnosis of depression and those with a primary diagnosis of substance use disorder. Providing appropriate sensory experiences may allow patients to function at an optimal level by improving their ability to self-regulate emotions and behaviors.
Sensory processing deficits and related disorders are often recognized and treated in pediatric settings, but these resources usually diminish after a person becomes an adult. Additionally, adults with atypical sensory preferences or sensory processing disorders (SPDs) who were not diagnosed as children often need to navigate their adult years without any education or intervention that may assist with future functioning and engagement. May-Benson (2011) endorsed the fact that sensory processing difficulties are present throughout the course of life and that there is little change in sensory processing from childhood to adulthood. She recognized that adults with SPD often present with comorbid mental health problems and that the symptoms of SPD are often misattributed to those mental health issues.
Sensory information processing patterns in mental health treatment have been studied with varying and, sometimes, limited results, often ending with a call for further research in the area of sensory integration and mental health disorders. Engel-Yeger et al. (2018) explored the relationship between symptomatology and the sensory profiles of people with unipolar and bipolar affective disorders, as well as which sensory preferences may respond better to antidepressant medications. Their results indicated that participants with a preference for reduced sensation seeking, hypersensitivity, enhanced sensory avoidance, and lower ability to register information responded better to antidepressant medications, as indicated by lower depression levels. Rieke and Anderson (2009) found that adults with obsessive–compulsive disorder (OCD) scored higher in the areas of sensory sensitivity and sensation avoiding, which was consistent with symptomatology in OCD literature. Additionally, these adults scored higher on low registration and lower on sensation seeking. Engel-Yeger and Dunn (2011) identified a relationship that was consistent with symptomatology by assessing the relationship between sensory processing difficulties and trait and state anxiety in healthy adults. They found that participants with sensory hypersensitivity, as well as those with low registration of sensory input, showed elevated trait and state anxiety, and sensation avoiding was found to be the significant predictor for state anxiety.
Another article highlighted research that was related to schizophrenia and sensory processing, including problems with motion processing and perception as well as difficulty in visual processing contributing to problems with emotion identification (Champagne & Frederick, 2011). With the Adolescent/Adult Sensory Profile (AASP), people who had been diagnosed with schizophrenia were found to score higher than most people in the areas of low registration and sensation avoiding quadrants and were found to score lower in the area of sensation seeking (Brown & Dunn, 2002). Additionally, Brown and Dunn (2002) identified a configuration of scores on the AASP that are compatible with symptoms of posttraumatic stress disorder (PTSD). These include increased arousal such as hypervigilance and increased startle response (high scores in the sensory sensitivity quadrant), avoidance of stimuli (high scores in the sensation avoiding quadrant), and numbing of responsiveness (high scores in the low registration quadrant). With regard to participants with symptoms of depression, Serafini et al. (2017) showed a relationship among depression and higher sensory sensitivity and sensation avoiding behavior and a significant relationship with lower registration of sensory input. Another study (Yano et al., 2019) discussed the positive relationship between sensory processing sensitivity and depressive symptoms. Those people who perceived more stressors and became easily overaroused were prone to learned helplessness and other symptoms of depression.
Other studies discussed sensory processing in adults with substance use and dependency. Bashapoor et al. (2015) found that people with substance dependence disorders process sensory information in a different way from a control group, and Borges et al. (2017) cited a sensory imbalance as an implication for decreased resilience in adults with drug use. Stols et al. (2013) suggested that atypical sensory processing patterns exist with people who abuse substances and hypothesized a relationship between these patterns and anger behavior. Engel-Yeger (2014) found a difference in sensory processing for people with a substance use disorder (SUD) in the areas of sensory sensitivity and sensation avoiding when compared with a control group. However, although SPD was more prevalent among people who were dependent on substances, it was hard to distinguish whether people were susceptible to substance abuse as a compensatory mechanism or whether the sensory processing concerns were a result of changes in the brains of people who abuse substances (Engel-Yeger, 2014). In either case, it is important to understand these sensory needs when providing treatment and for encouraging long-term recovery success. Kelly et al. (2021) studied sensory patterns in a slightly younger population (ages 14–24 yr) attending an alcohol and drug treatment service. They also found that the participants’ sensory processing patterns were significantly higher than the norm in the areas of low registration, sensory sensitivity, and sensation avoiding. They reported high rates of comorbid probable PTSD, psychological distress, and low quality of life, which could be additional factors that affect sensory processing (Kelly et al., 2021).
Although sensory processing had been studied among those with mental health disorders and those with substance use disorders, to our knowledge, no study to date has reported a direct comparison of sensory processing among these patients. To address this, we performed a retrospective study to compare the sensory processing preferences of patients with a primary diagnosis of depression with those of patients with a primary diagnosis of SUD, both groups having been admitted to an adult acute inpatient mental health center that treats patients with psychiatric and/or addiction recovery needs. These diagnoses were selected because of the high prevalence of each among our cohort of admitted patients. We assessed sensory processing as part of routine care using the AASP. Identifying patterns between these specific diagnoses and sensory processing preferences could inform treatment needs and improve quality of care.
Method
Participants
This is a retrospective cohort study of adult patients, ages 18 to 64 yr, who had been admitted to an adult acute inpatient psychiatric and addiction recovery center between July 1, 2018, and June 30, 2021. Within this cohort, we identified participants with a primary diagnosis of either depression or SUD at the time when they completed the AASP as part of their occupational therapy evaluation. If a patient had multiple admissions during the time period studied, they were only included once. The study was reviewed as exempt by the MaineHealth Institutional Review Board.
Data Collection
We collected demographic (age, gender identity, race) and clinical (including comorbid diagnoses, medication use, clinical event occurrences, and length of stay) data for each patient from their electronic health records. Data from the AASP, a self-evaluation of general behavioral responses to everyday sensory experiences, were also available in the medical record. The AASP includes 60 questions that are answered on a Likert scale, and it is designed to provide an increased awareness and understanding of a person’s sensory processing preferences and thus assist with intervention planning based on a person’s sensory preferences. Scores are calculated by four quadrants: ▪ Low Registration: Items identify behaviors such as missing stimuli or responding slowly. ▪ Sensation Seeking: Items identify behaviors that include enjoying or creating additional stimuli or looking for environments that provide sensory stimulus. ▪ Sensory Sensitivity: Items identify responses such as noticing behaviors (startle response), distractibility, and discomfort with sensory stimuli. ▪ Sensation Avoiding: Items identify responses and behaviors such as deliberate acts to reduce or prevent exposure to sensory stimuli or efforts to make exposure more predictable.
The AASP provides normative data so that a person’s scores for the four quadrants can be expressed in terms of the sensory processing patterns of people in the same age group. Scores for each quadrant are ranked as much less than most people, less than most people, similar to most people, more than most people, and much more than most people (for Low Registration, 15-18, 19-23, 24-35, 36-44, and 45-75; for Sensation Seeking, 15–35, 36–42, 43–56, 57–62, and 63–75; for Sensory Sensitivity, 15–18, 19–25, 26–41, 42–48, and 49–75; and for Sensation Avoiding, 15–19, 20–26, 27–41, 42–49, and 50–75, respectively).
Data Analysis
Demographic, clinical, and AASP data were summarized using descriptive statistics, both overall and after stratification by primary diagnosis subgroup. Continuous data are shown as mean (SD) or median (interquartile range), as appropriate, and categorical data are shown as frequency, n (%). We used t tests to evaluate differences in AASP scores between primary diagnosis subgroups. We combined the five classifications of normalized AASP scores into three groups (“less/much less than most people,” “similar to most people,” and “more/much more than most people”) and evaluated differences in the distribution of these categories between primary diagnosis subgroups using the chi-square test or Fisher’s exact test, as appropriate. All analyses were performed using IBM SPSS Statistical Software (Version 28).
Results
Descriptive Data
Among 897 patients evaluated for inclusion in the study, 364 (40%) were not evaluated by an occupational therapist, 221 (25%) were evaluated but were not assessed by AASP as part of their occupational therapy treatment, 42 (5%) were given the assessment but did not complete it, 59 (6%) represented subsequent admissions, and 211 (24%) were eligible for inclusion in the study.
Demographic data are presented in Table 1; of the 211 patients included, 121 (57%) had a primary diagnosis of depression, and 90 (43%) had a primary diagnosis of SUD at the time of AASP completion.
Demographic and Clinical Characteristics of the Study Group, Overall and Stratified by Primary Diagnoses
Note. Mean ages, in years, were as follows: 33.8 (SD = 10.5) for the total population, 32.3 (SD = 10.6) for the depression group, and 35.7 (SD = 10.2) for the substance use group. IQR = interquartile range; PRN = as needed.
aIncludes diagnoses of all types of depression, such as depression, unspecified; major depressive disorder; bipolar disorder, depressed; depression with suicidal ideation; and depression with psychotic features.
All non-Hispanic.
cIncludes Asian, n = 1; other, n = 1; more than one race (Hispanic), n = 1; and unknown, n = 2.
dIncludes Black/African American, n = 1; and Native American/Alaska Native, n = 2.
Data are shown as median (IQR) or frequency, n (%).
Includes medication for sleep, pain, anxiety, or agitation/irritability/anger.
Sensory Processing
Table 2 shows AASP quadrant scores, stratified by primary diagnosis group. The depression group had significantly higher scores on low registration (p = .002), sensory sensitivity (p = .013), and sensation avoiding (p ≤ .001). In contrast, the SUD group scored significantly higher for the sensation seeking quadrant (p = .002).
Sensory Processing Scores, Overall and Stratified by Primary Diagnosis
Note: AASP = Adolescent/Adult Sensory Profile.
Figure 1 illustrates that the findings summarized in Table 2 persisted after AASP quadrant scores were normalized against scores for an 18- to 64-yr-old population; there was a significant difference between primary diagnosis subgroups across all AASP quadrants that mirrored the findings shown in Table 2. The depression group was more likely to rank higher than the normative population in the quadrants of low registration, sensory sensitivity, and sensation avoiding, whereas those in the SUD group ranked similarly to the normative population across all four quadrants. However, as illustrated in Figure 1, 86% (n = 77) of the SUD group scored atypically for at least one of the four sensory processing quadrants, 52% (n = 47) scored atypically on two or more of the quadrants, and 26% (n = 23) scored atypically on three or four quadrants. The frequency of atypical responses within quadrants for the SUD group were as follows: Atypical scores for low registration occurred 47.8% of the time (n = 43), atypical scores for sensation seeking occurred 41.1% of the time (n = 37), atypical scores for sensory sensitivity occurred 36.6% of the time (n = 33), and atypical scores for sensation avoiding occurred 46.7% of the time (n = 42).
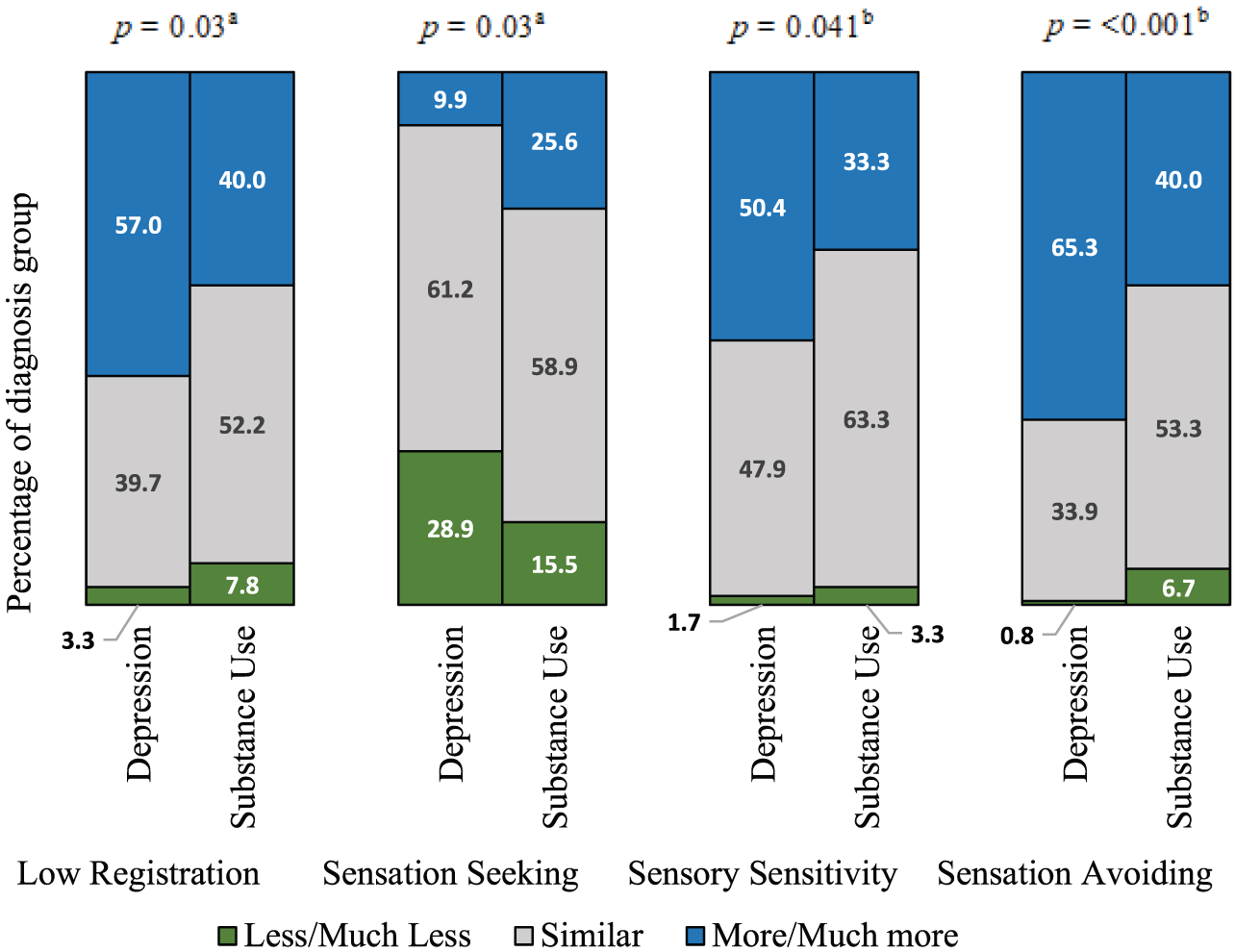
Graphical comparison of sensory processing between patients with a primary diagnosis of depression and those with a primary diagnosis of a substance use disorder, normalized to scores for 18- to 64-yr-olds.
Discussion
We have identified that patients who present to an acute care mental health clinic with a primary diagnosis of depression and those who present with a primary diagnosis of SUD have significant differences in their sensory processing profiles. Although our findings are individually consistent with the findings of others (Bashapoor et al., 2015; Borges et al., 2017; Engel-Yeger, 2014; Kelly et al., 2021; Yano et al., 2019), to our knowledge, this is the first time that the groups have been compared directly with each other. For example, our findings are consistent with those of Serafini et al. (2017), who found higher scores for sensory sensitivity, sensation avoiding, and low registration among those with depression. They are also consistent with those of Stols et al. (2013), who reported that 71.4% of patients with SUD scored in accordance with the norm. The majority of the latter study population cognitively avoided their anger or used depressants, which led the authors to suggest that substance use may be linked to an attempt to lower excitement levels. This may explain our finding that 40% of patients in the SUD group scored “more/much more than most” in the area of sensation avoiding.
Given the increased potential for a dysfunctional presentation because of the sensory processing patterns of patients with depression or a substance use disorder, a typical inpatient setting may present many barriers and challenges for these patients. If these issues lead to dysregulated states, the patient may have decreased engagement in facility activities, difficulty retaining presented information, and reduced problem-solving skills (Ostrove & Hartman, 2013). Each of these factors is a large determinant of a productive hospital stay. It is, therefore, important to consider potential obstacles to treatment when patients present either with an atypical sensory profile pattern or with a primary diagnosis (e.g., depression) that predisposes to this.
Limitations
The methodology for this study was not designed to account for internal validity factors such as comorbid diagnoses and instances of dual diagnoses. Of the total population, 191 (90.5%) of the patients received a comorbid psychiatric diagnosis (unrelated to substance use) by history, and 147 (69.7%) received a comorbid substance use diagnosis by history (either a second substance in the SUD group or at least one substance use diagnosis in the group with depression as the primary diagnosis).
Although the study provides a representative sample of typical patients who were admitted to the facility, this study was also limited to the patients who were able to complete an occupational therapy evaluation and who were then determined to benefit from completing the AASP and followed through. The assessment was not completed by all patients who were admitted during this time frame.
Future Research
Future research focusing on the sensory preferences of people who abuse substances, stratified by specific substance used, may be beneficial to further individualization of treatment approaches. For example, a person who abuses alcohol may have different sensory preferences than a person who uses stimulants. The expected effect of the substance may be a maladaptive response to sensory preferences.
Investigators also plan to complete future research proposing that adding a sensory intervention could positively affect the patient experience and could change clinical characteristics, such as reducing dependence on as-needed medications and less emotional and behavioral dysregulation that leads to increased supervision.
Additional hospital populations that could be studied to determine the benefit from increased access and availability to calming sensory accommodations include, but are not limited to, emergency departments, patients receiving chemotherapy, mothers in labor and obstetrics–gynecology areas, patients waiting for day surgery, and so forth.
Implications for Occupational Therapy Practice
The initial motivation for this research was to explore potential opportunities for individualizing care in a group environment, specifically by meeting sensory processing needs to improve emotional and behavioral regulation. The findings of this study have the following implications for occupational therapy practice: ▪ Atypical sensory processing is prevalent in adult populations. Occupational therapists should consider assessing sensory preferences and accommodating as able when implementing interventions, regardless of setting. ▪ An opportunity is available for occupational therapists to educate other treatment team staff about “person-first” thinking and adaptive versus maladaptive responses to sensory stimuli; for example, suggest thinking about what factors could have led to a negative response or behavior rather than assuming that a patient is “just acting out.” ▪ The potential exists to advocate for greater access to sensory interventions as standard care in adults. For example, in a mental health setting, consider providing a sensory environment, such as a sensory room, with a wide range of options to meet individual patient needs to assist with emotional and behavioral regulation.
Conclusion
The results of this study support the benefit of including sensory preferences when creating a comfortable and safe inpatient environment. However, the fact that these two populations scored significantly differently across the four quadrants illustrates the difficulty in providing interventions in a mixed population and should be considered when decisions are being made about what should be included and provided during care. Additionally, despite the mean scores for the substance use group being “similar to [those of] most people,” there were atypical observations within this study group that are worth addressing in treatment and in future research.
Providing the patients, as well as the staff working with this population, a better understanding of the role sensory processing preferences can play in the patient’s behavioral and emotional regulation is the start to improving overall treatment approaches and outcomes. Safe access to options to meet sensory processing needs, such as creating a sensory inclusive environment and culture, can allow patients to function better during the acute phase of illness, improve their ability to engage in treatment earlier in their admission and overall (especially for those susceptible to self-isolation as a way to avoid environmental stimuli and perpetuate symptoms of depression), and improve their overall satisfaction with treatment. Improving sensory experiences and opportunities can provide comfort during an uncomfortable time in a patient’s life.
Footnotes
Acknowledgments
This work was supported in part by Northern New England Clinical and Translational Research Grant U54GM115516. We thank Caroline Knight, RN, BSN, CCRP, and Wendy Craig, PhD, for their assistance and support of this project.