
Abstract
This study’s rigorous tests of motor skills interventions support ways to manage motor difficulties in children with autism spectrum disorder (ASD). An occupational therapy intervention based on motor learning theory could benefit preschool children with ASD, especially in terms of manual coordination ability and overall gross and fine motor skills.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impaired social communication, interaction deficits, and the presence of restricted, repetitive patterns of behaviors (American Psychiatric Association [APA], 2013). Preschool children are generally more independent than infants or toddlers. One of the main developmental goals in the preschool period is to ensure that children are prepared and ready to attend primary school (Williams et al., 2019). However, children with ASD are at high risk of developmental delays in overall motor, cognitive, social–emotional, and language and speech development (Kodak & Bergmann, 2020). Early intervention aims to help children and their families with these developmental problems. In addition to the core symptoms of ASD, studies have indicated that as many as 80% to 90% of children with ASD have significant motor difficulties, and about 10% of them are at risk of motor abnormalities (Bhat, 2020; Green et al., 2009; Hilton et al., 2007). However, in clinical or educational settings, few children receive interventions that target improvement in their motor abilities (Bhat, 2020). Evidence of the effectiveness of interventions or treatments to improve motor abilities is lacking, especially for preschool children with ASD.
Motor abilities are needed to perform and execute tasks and to participate in activities and occupations (American Occupational Therapy Association, 2020; Schmidt & Lee, 2013). Delayed or impaired motor abilities are negatively associated with other developmental delays, psychosocial well-being, and positive occupational participation (Bhat, 2020; Blaesi & Wilson, 2010; Chi & Lin, 2021; Clearfield, 2011; Eskenazi et al., 2009 ; Holloway & Long, 2019; Holloway et al., 2018; Travers et al., 2021; Wilson & Knoblich, 2005). Studies focusing on motor problems among children with ASD can be traced back to 1943 (Kanner, 1943). However, the majority of studies looking at motor problems among children with ASD have been conducted in the past two decades. Children with ASD have been reported to have motor problems, including decreased muscle tone (Ming et al., 2007; Shetreat-Klein et al., 2014), insufficient muscle strength (Alsaedi, 2020; Pan, 2014), poor postural control (Alsaedi, 2020; Green et al., 2002, 2009; Hilton et al., 2007; Liu & Breslin, 2013; Molloy et al., 2003; Paquet et al., 2016; Whyatt & Craig, 2012), and poor gross and fine motor skills (Alsaedi, 2020; Green et al., 2002, 2009; Hilton et al., 2007; Liu & Breslin, 2013; Nobile et al., 2011; Pan et al., 2009; Staples & Reid, 2010; Whyatt & Craig, 2012), have been reported. Among children with ASD, motor difficulties are related to motor control problems, such as atypical sensory feedback generation and modulation, poor coordination, and poor sequencing and planning ability (Alsaedi, 2020; Dirksen et al., 2016; Fournier et al., 2010; Green et al., 2002, 2009; Hilton et al., 2007; Liu & Breslin, 2013; Nobile et al., 2011; Pan et al., 2009; Staples & Reid, 2010; Whyatt & Craig, 2012).
Presently, the evidence of motor problems among children with ASD is sufficient. However, evidence of the effects of interventions or treatments for these motor problems is lacking, especially for preschool children with ASD. Most prior motor skills interventions that have been shown to have positive effects on motor skill performance have primarily been used with school-age children with ASD (ages 4–18 yr; Cheldavi et al., 2014; El-Shemy & El-Sayed, 2018; Henderson et al., 2016; Pan et al., 2017; Rafie et al., 2017; Rafiei Milajerdi et al., 2021; Sansi et al., 2021; Sarabzadeh et al., 2019; Sarol & Çimen, 2015; Toscano et al., 2018). Only two studies have specifically examined motor skills interventions for 4- to 6-yr-old children with ASD (Bremer et al., 2015; Ketcheson et al., 2017).
Table A.1 in the Supplemental Appendix (available online with this article at https://research.aota.org/ajot) summarizes the effects of motor skills interventions among children with ASD reported in previous studies. These motor skills and physical activity interventions show promising results for improving motor skill competence among children with ASD. Motor skills interventions based on motor learning theory could improve children’s motor skills performance and are commonly used by occupational therapists. These interventions focus mainly on locomotor (i.e., running, hopping, leaping) and object control (i.e., throwing, catching, kicking) skills.
Although previous research studies investigating motor skills interventions based on motor learning theory have shown the effectiveness of the interventions with some promising results, only six studies published between 2010 and 2022 investigated the effectiveness of motor skills interventions for children with ASD. The empirical evidence gathered thus far is insufficient, and the dimensions of the outcome measures are limited (Bremer et al., 2015; Cheldavi et al., 2014; El-Shemy & El-Sayed, 2018; Pan et al., 2017; Sansi et al., 2021; Sarabzadeh et al., 2019). Some researchers have conducted physical activity interventions (such as physical education, sports, recreation, dance, and physical exercise) to improve motor skills performance. Previous studies have also indicated that children with ASD could improve their motor abilities through physical activity (Henderson et al., 2016; Ketcheson et al., 2017; Rafie et al., 2017; Rafiei Milajerdi et al., 2021; Sarol & Çimen, 2015; Toscano et al., 2018). Although each of these studies included a control group, none of the control groups received the intervention or they were on the waiting list without a dose-matched intervention. We could not exclude the effect of different dosages in the experimental groups because those participants spent more time practicing their motor skills exercises than the participants in the control group, who did not receive any intervention.
The first pilot randomized controlled trial (RCT) with nine young children with ASD (age 4 yr) implemented a motor skills intervention for 6 wk (Bremer et al., 2015). After the intervention, the children’s motor skills had significantly improved in comparison with the control group, who did not receive the intervention. Moreover, Bremer et al. (2015) found no significant differences between two intensities of the same intervention dosage in terms of motor skills improvement. Increasing the intensity of the motor skills intervention was not more effective at improving motor skills, adaptive behavior, and social skills, suggesting that intervention dosage could play an important role in study outcomes regardless of the intensity.
In the dosage-matched interventions, children with ASD improved their motor abilities through physical activity (see Table A.1 in the Supplemental Appendix). Previous studies have found that cognitive-oriented physical activity rehabilitation programs (i.e., exercises with cognitive demands such as attention, cognitive flexibility, inhibitory control, and working memory) have significant positive effects on motor skills performance among children (Zamani sani et al., 2021; Greco, 2020; Halperin et al., 2013; Hilton et al., 2014; Pan et al., 2017; Samsudin & Low, 2017). Previous studies have noted similarities between motor problems among children with ASD and those among children with attention deficit hyperactivity disorder (ADHD; Biscaldi et al., 2015; Pan et al., 2009). The cognitive-oriented physical activity rehabilitation program Exercise for Cognitive Improvement and Rehabilitation (EXCIR) was developed for children with ADHD to improve their attention span and level of physical activity (Nejati & Derakhshan, 2021). Therefore, EXCIR could also have positive effects for children with ASD. Many children with ASD show a natural affinity for using technology and learning through the use of computers (Kumazaki et al., 2020; Valencia, Rusu, Quiñones, & Jamet, 2019). To date, no published studies have compared the efficacy of motor skills interventions and physical activity interventions based on different approaches for preschool children with ASD. Therefore, there remains a gap in our knowledge regarding the efficacy of different motor interventions. It is critical to fill this gap with comprehensive research to identify the optimal treatment types for this population. Thus, we used a cognitive-oriented physical activity rehabilitation program as a comparison intervention in the current study.
Outcome measures are primarily focused on motor performance, including the Bruininks–Oseretsky Test of Motor Proficiency–Second Edition, Movement Assessment Battery for Children–Second Edition (MABC–2; Henderson et al., 2007), Peabody Developmental Motor Scales–Second Edition, and Test of Gross Motor Development–Second Edition. These motor assessments can help facilitate an understanding of children’s motor capabilities and performance; however, one of the disadvantages is that there is a gap between the assessment and performance in natural settings. Only a few studies have used the Vineland Adaptive Behavior Scales (Bremer et al., 2015), Child Health Questionnaire physical summary score (Toscano et al., 2018), and Pediatric Quality of Life Inventory, Physical Functioning subscale (Sarol & Çimen, 2015), to collect parents’ subjective views of their children’s motor performance and physical ability in daily life through self-report questionnaires. The disadvantage of self-report questionnaires is that parents may have perceptions that differ from their child’s actual performance and feelings. However, no published studies have explored the impact of motor skill interventions on self-care performance; thus, this study aimed to provide insight into this gap in the literature.
Many studies have targeted motor difficulties among children with ASD using motor skills or physical activity interventions and have reported mixed results (Busti Ceccarelli et al., 2020; Healy et al., 2018; Monteiro et al., 2022). The evidence for the efficacy of motor skills interventions based on motor learning theory for preschool children with ASD is insufficient. To date, no definitive conclusions have been made regarding the efficacy of different motor interventions. An effective, evidence-based intervention that could be used for preschool children with ASD is needed and would provide a foundation for further exploration. The participants and outcome assessors in many of the previous studies were not blinded to the group assignments. To address this, a rigorous RCT with a dosage-matched comparison group is needed to examine the efficacy of motor skills interventions on the functional performance of children with ASD. This study examined the efficacy of the Motor Skill Occupational Therapy Intervention ON ASD (MOTION–ASD) and Cognitive Orientation Exercise (CO–EXC) programs to improve motor skills performance, self-care performance, and adaptive behaviors among preschool children with ASD.
Method
Study Design
This study used a triple-blinded, two-group, randomized controlled design to examine the efficacy of the MOTION–ASD and CO–EXC programs. Participants, intervention providers, and outcome assessors were blinded to the study groups. After recruitment and enrollment, participants in this study were randomly assigned to the MOTION–ASD group or the CO–EXC group and engaged in an 8-wk intervention with the same dosage and frequency for both groups. Figure 1 shows the Consolidated Standards of Reporting Trials (CONSORT; Schulz et al., 2010) flow diagram of study recruitment, treatment allocation, and assessment.
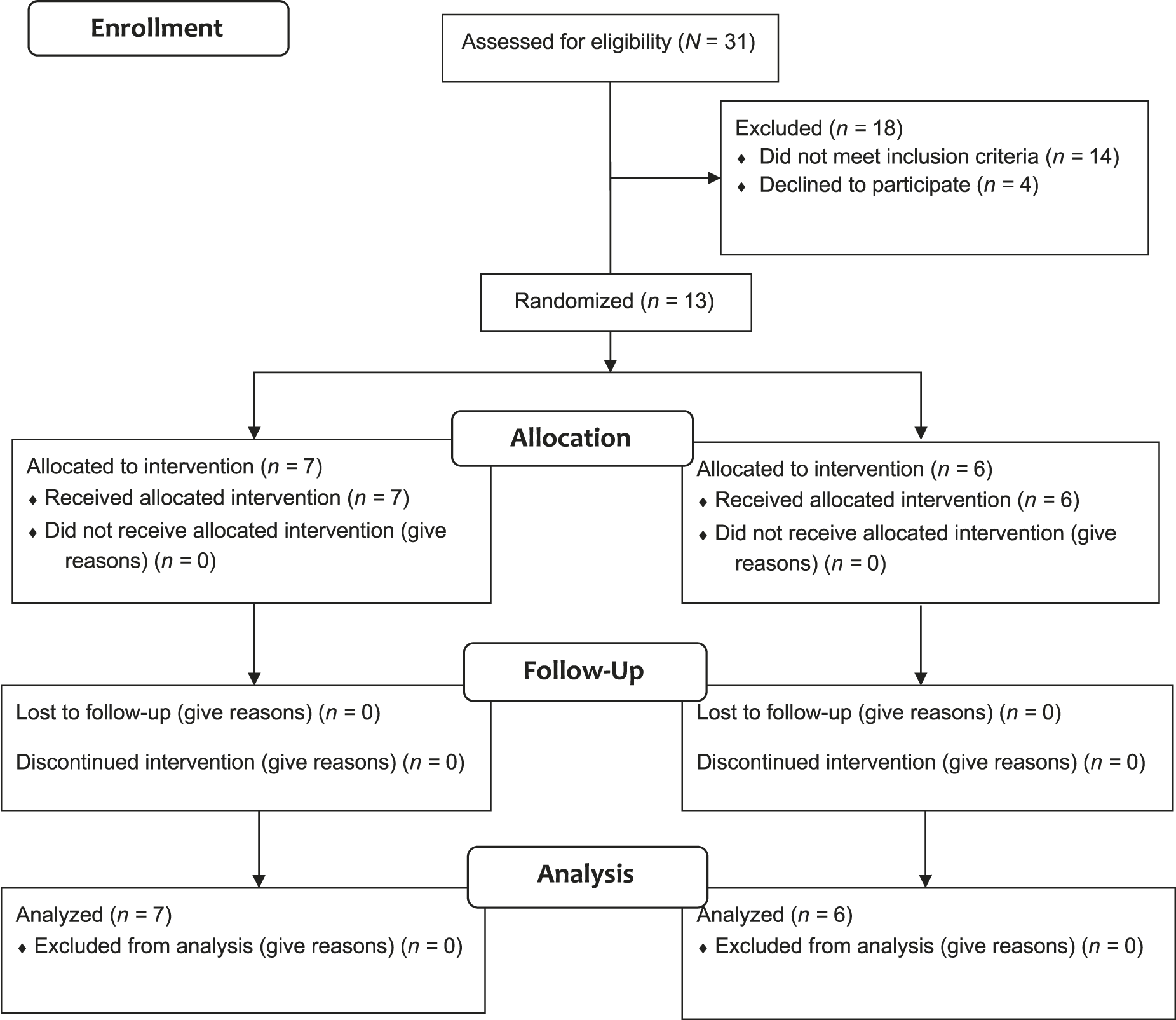
CONSORT flow diagram of study recruitment, treatment allocation, and assessment.
Participants
Initially, we recruited 31 potential participants from clinics, hospitals, and early intervention centers. The inclusion criteria were as follows: (1) ages 48 to 71 mo; (2) diagnosed with ASD by a registered pediatric psychiatrist according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; APA, 2013); (3) score ≥30 on the Childhood Autism Rating Scale– Second Edition (CARS–2; Schopler et al., 2010); (4) score ≥70 on the Test of Nonverbal Intelligence–Fourth Edition (TONI–4; Brown et al., 2010); and (5) scores in the amber zone (risk of developmental delay) or red zone (developmental delay) in any of the subscales of the MABC–2 (Henderson et al., 2007). Children who had any other neurological or physiological diagnoses or impairments and who were unable to follow one-step simple directions were excluded. When contacted, 4 eligible participants declined to participate because of the coronavirus pandemic. After applying the inclusion criteria, 13 children with ASD ages 4 to 5 yr and their parents were randomly assigned to the MOTION–ASD group (n = 7) or the CO–EXC group (n = 6). The MOTION–ASD and CO–EXC interventions are described in the Intervention section.
Recruitment at clinics, hospitals, and early intervention centers was active from December 2021 to January 2022. No participants dropped out before the end of the study. As shown in Table 1, the participants had no significant differences in demographic characteristics. All of the children were male because males are 4 times more likely than females to be diagnosed with ASD (Maenner et al., 2021). The children with ASD ranged in age from 4 to 5 yr, with a mean age of 4.91 yr. The ASD symptom severity of the children ranged from mild to severe, with a mean score of 34.3 (SD = 4.4). The mean score on the MABC–2 was 4.5 (SD = 2.7), indicating difficulties with performing motor tasks.
Characteristics of the Sample
Note. CARS2–ST = Standard Version of Childhood Autism Rating Scale–Second Edition; MABC–2 = Movement Assessment Battery for Children–Second Edition; TONI–4 = Test of Nonverbal Intelligence–Fourth Edition, Chinese Edition.
Measures
CARS-2
The CARS–2 is a 15-item rating scale developed to assess the symptom severity of ASD. A certified pediatric occupational therapist (Yi-Shan Sung) administered the scale; responses were made on a 4-point Likert scale ranging from 1 (age appropriate) to 4 (severely abnormal), with half-point scores possible for each item. Higher total scores indicate more severe autism symptoms. The cut-off point for the presence of autism is a score >30. Scores between 30.0 and 36.5 indicate mild to moderate autism, and scores >37 indicate severe autism. The reliability and validity of this scale are reported to be good, and Cronbach’s αs = .87 to .92, with sensitivity of .86 and specificity of .79 (Schopler et al., 2010).
TONI–4
The TONI–4 is used to assess intelligence with language-free and motor skill–reduced formats for children ages 4 to 15 yr. It has 60 items, arranged from easy to difficult, that assess two components of intelligence: abstract reasoning and problem solving. Cronbach’s α is .862, internal consistency ranges from .8 to .87, and test–retest reliability ranges from .84 to .90 (Brown et al., 2010). Because children with ASD present with language and speech delays, studies have recommended the use of a nonverbal intelligence assessment to reduce bias (Whyatt & Craig, 2012). Studies in which this assessment was used with children with ASD have shown its appropriateness as a measure for children with ASD (Bishop et al., 2015).
MABC–2
The MABC–2 was used to assess motor skills. This test has three age bands, covering ages 3 to 6 yr, 7 to 10 yr, and 11 to 16 yr. It consists of eight subtests, which make up three component motor domains: Manual Dexterity, Ball Skills, and Balance. This test can be administered by an occupational therapist and takes approximately 25 min to complete. Good reliability and validity have been built into this assessment (Henderson et al., 2007). The MABC–2 has high sensitivity (79%) and specificity (93%) for predicting motor impairment among children age 4 yr (Griffiths et al., 2017), and it has been reported to be appropriate for assessing motor problems among children with ASD (Green et al., 2002, 2009; Henderson et al., 2007; Hilton et al., 2007; Liu & Breslin, 2013; Whyatt & Craig, 2012). Because the MABC–2 has good specificity for predicting motor impairment, this tool was used to screen for whether children had motor problems (an inclusion criterion in this study).
BOT–2, Brief Form
The BOT–2, Brief Form (BOT–2–BF; Bruininks & Bruininks, 2010) is an individually administered test with goal-directed activities to measure the motor skills of individuals ages 4 to 21 yr. This test can be administered by a certified occupational therapist within 15 to 20 min. The BOT–2–BF assesses motor proficiency across eight domains: Fine Motor Precision, Fine Motor Integration, Manual Dexterity, Bilateral Coordination, Balance, Speed and Agility, Upper-Limb Coordination, and Strength. These eight domains are categorized into four motor-area domains: Fine Manual Control (Fine Motor Precision, Fine Motor Integration), Manual Coordination (Manual Dexterity, Upper-Limb Coordination), Body Coordination (Bilateral Coordination, Balance), and Strength and Agility (Speed and Agility, Strength). The raw score on each item can be converted to a point score, which is a type of standard score to evaluate motor performance. The total point score can be then converted to a standard score according to sex-specific norms. This test has good reliability and validity (Bruininks & Bruininks, 2010). The intraclass correlation coefficient (.80) is high for reliability. The BOT–2–BF has been reported to be appropriate for use for children with ASD (Bruininks & Bruininks, 2010). Many studies on motor skills interventions have also used this assessment as an outcome measure (El Shemy & El-Sayed, 2018; Pan et al., 2017; Rafie et al., 2017).
Assessment of Motor and Process Skills
The Assessment of Motor and Process Skills (AMPS; Fisher & Jones, 2012) is a standardized observational assessment of self-care and daily activity with good reliability and validity. Norms for those ages 3 to 103 yr and for different disability groups have been built into the AMPS. The AMPS is scored on a scale ranging from 1 (severe skill deficits) to 4 (readily and consistently) for motor and process skills; scores are calculated using AMPS computer software. The AMPS was developed using a many-faceted Rasch measurement model, with logit scores to represent self-care ability compared with age-matched peers (Fisher & Jones, 2012). A higher logit score indicates better self-care ability. Good reliability and validity have been built into this assessment; the Rasch equivalent of Cronbach’s α is .91 and .92, respectively, for the Motor Skills and Process Skills subscales. The test–retest reliability is .90, and children could demonstrate valid response patterns across AMPS items and tasks. The AMPS was used to further explore self-care performance, as in a previous study, which showed great promise (Chi & Lin, 2021). AMPS activities of daily living (ADL) motor skill scores <1.5 logits and AMPS ADL process skills scores <1 logit are indicative of poor ADL task performance. In this study, we used this assessment to understand functional performance related to motor and process abilities in daily self-care performance.
Vineland Adaptive Behavior Scales–Third Edition
The Chinese version of the Vineland Adaptive Behavior Scales–Third Edition (Vineland–3; Cheng et al., 2020) is used to understand children’s adaptive behaviors in daily living and school life. Adaptive behaviors are defined as the performance of daily activities required for personal and social sufficiency. This scale contains 14 subscales, each including 20 to 30 items for caregivers or teachers to complete; they represent adaptation in four main domains: Communication, Daily Living Skills, Socialization, and Motor Skills. Scoring is based on the frequency of the observed behavior for each item: 0 (never), 1 (sometimes), and 2 (usually). Taiwanese norms have been built into the Chinese Vineland–3, and there are three versions based on age: a toddler version for ages 2 to 5 yr, a child version for ages 6 to 17 yr, and an adult version for ages 18 to 90 yr. In this study, we used the Parent/Caregiver Form and the toddler version of the Vineland–3 for children ages 4 to 5. The reliability and validity of the Chinese version of the Vineland–3 have been confirmed in Taiwan. Its internal consistency has been established; the split-half reliability ranges from .87 to .99, and the test–retest reliability ranges from .62 to .93 (Cheng et al., 2020). The Vineland–3 has been reported to be appropriate for use with children with ASD. This assessment was used to gather daily performance information from parents to understand the effect of motor skills transfer or generalization in this study.
Intervention
Eight 90-min sessions were conducted once a week for both the MOTION–ASD and the CO–EXC groups. These sessions were conducted with a 1:1 therapist-to-child ratio. The occupational therapists in both groups were trained in advance to meet the principles and protocols of the intervention design. The research team provided in-person training and a manual to the therapists in each group. A 10-item self-evaluation checklist was completed by the occupational therapist to ensure that the intervention process met the principles and protocol of the study. The researcher (Ling-Yi Lin) supervised every session to ensure the quality of the intervention and answer any questions from participants or caregivers.
MOTION–ASD
MOTION–ASD is based on motor learning theory and was administered by a certified occupational therapist (Yu-Ru Jin) over eight sessions for four different motor skills domains: Postural Control, Locomotion, Object Manipulation, and Manual Dexterity. Each domain was administered within two sessions. The first session focused on the fundamental motor skills of a certain domain. In the second session, training was provided in skills that were more complex, required more planning, and involved coordinating demands. Every session included an introduction, a warm-up, three activities with random breaks between trials, a discussion, and a conclusion. Each session contained three activities, along with learning stages, and was designed and accompanied by appropriate augmented feedback from an occupational therapist. An example of the process is presented in Table 2 and highlights the three activities used in the first session of the Postural Control domain. The strategy consisted of letting the children make decisions and set appropriate goals and providing appropriate augmented feedback to encourage them to keep participating in the intervention session. The occupational therapist guided the children to connect their motor skills and daily occupations and helped them to understand their performance and learn to condition themselves through discussion and reviewing.
MOTION-ASD Protocol Example: Postural Control 1
CO–EXC
The CO–EXC, adopted from the Exercise for Cognitive Improvement and Rehabilitation (Nejati & Derakhshan, 2021), is a cognitive-oriented physical activity rehabilitation program aimed at improving attention, impulse control, cognitive flexibility, working memory, and levels of physical activity in children. The CO–EXC program involves 12 games focused on different cognitive abilities. Each game was conducted twice per session. The CO–EXC intervention included an introduction, warm-up, 3 of the 12 games, a discussion, and a conclusion. The occupational therapist used cognitive activities to help prepare the children, such as selected number jumping (the children jump to a mat only when a specific number is shown on the screen; interference control), limb movements (sustained attention), and clap–no-clap (inhibitory control). For example, when doing the selected number jumping, the child was asked to jump on the smaller of two presented numbers with different amounts and sizes of numbers. The discussion and conclusion sections were led by an occupational therapist to help the children review everything that they had practiced in the session and to make connections to school scenarios and daily activities.
Procedure
Parents or caregivers who were interested in the study could contact the primary investigator (Ling-Yi Lin) using the information on the flyer. The procedure was explained to the participants, and the primary investigator made the appointments for enrollment assessment in the laboratory. All parents signed informed consent forms before the study. The enrollment assessments, including the CARS–2, TONI–4, and MABC–2, were reviewed by a certified occupational therapist (Yi-Shan Sung). After reviewing the enrollment assessments, the participants were randomly assigned into the experimental group or the control group using a table of random numbers. In the preintervention assessments, children were assessed with the BOT–2–BF and AMPS tests by two other certified occupational therapists (Sung and Lin), who were blinded to group assignment. At the same time, parents were asked to complete the Vineland–3. The interventions were conducted in a National Cheng Kung University laboratory. After finishing the preintervention assessment, children began their interventions within 2 wk and attended all eight sessions. The postintervention assessments were the same as the preintervention assessments. Children were assessed within 1 wk after the last intervention session. The follow-up assessments occurred 1 mo after the postintervention assessment and used the same measures as the postintervention assessment.
Statistical Analyses
IBM SPSS Statistics (Version 22.0) was used for data analysis. Independent t tests were used to analyze the differences between the two groups in descriptive data and baseline characteristics, including autism severity, nonverbal cognitive ability, and motor ability. Nominal data were examined using the χ2 test. Fisher’s exact tests were used when more than 20% of the values were less than the expected value of 5 in a contingency table. Repeated-measures analysis of variance (ANOVA) was used to compare the effects and time interactions within and between groups on BOT–2–BF, AMPS, and Vineland–3 scores at three time points. The significance level was set at p < .05.
Results
No significant between-groups differences were found on all baseline measures. The mean score on the BOT–2–BF was 37.8 (SD = 9.3), indicating below- average motor ability. Children with ASD had a mean score of 1.4 (SD = 0.4) logits on the AMPS Motor Skills subscale and 0.5 (SD = 0.5) logits on the AMPS Process Skills subscale. Furthermore, 53.8% of the children with ASD scored below the cutoff score of 1.5 logits on the Motor Skills subscale, and 84.6% scored below the cutoff score of 1 logit on the Process Skills subscale. The mean score for the Vineland–3 Motor Skills domain was 85.2 (SD = 16.8), indicating moderately low motor ability. Four children with ASD had an adaptive behavior composite score of <70. Table 3 presents the BOT–2–BF, AMPS, and Vineland–3 data for the children with ASD at different time points, in comparison with age-matched normative data.
Repeated-Measures Analysis of Variance for Outcome Measures
Note. BOT–2–BF = Bruininks–Oseretsky Test of Motor Proficiency–Second Edition, Brief Form; AMPS = Assessment of Motor and Process Skills; Vineland–3 = Vineland Adaptive Behavior Scales–Third Edition, Chinese Version.
aGroup × Time interaction from preintervention to postintervention.
*p < .05. **p < .01.
Pretest–Posttest Comparisons
After the 8-wk intervention period, significant differences in BOT–2–BF Manual Coordination and Vineland–3 Motor Skills domain scores were evident between the two groups. The scores of children in the MOTION–ASD group were much higher than those of children in the CO–EXC group. The results of the repeated-measures ANOVA showed that there were significant Group × Time interactions for the Manual Coordination subtest of the BOT–2–BF, F(1, 11) = 5.042, p = .046, η2 = .314, and the Motor Skills domain of Vineland–3, F(1, 11) = 5.114, p = .045, η2 = .317. In addition, we compared change scores for the outcome measures between two time points. There was a strong effect of time on BOT–2–BF Fine Manual Control, Body Coordination, and the point score for total motor skills and AMPS Motor Skills and Process Skills subscales in both groups after the 8-wk period, indicating that the motor abilities and daily self-care performance of children in both groups improved with time. However, no significant between-groups differences were found in strength and agility. Table 3 presents the results for the full model.
Follow-Up Tests (Maintenance)
Repeated-measures ANOVAs with time (postintervention and follow-up) as a within-subject factor revealed that there were no statistically significant differences between mean scores on the BOT–2–BF and the AMPS Motor Skills and Process Skills subscales at posttest or follow-up, indicating a maintenance effect. The results revealed that all children in the MOTION– ASD group had continuous improvement above their posttest levels on the point score for total motor skills for the BOT–2–BF. Six of seven children in the MOTION– ASD group (i.e., 85.7%) showed continuous improvement in scores on the BOT–2–BF Fine Manual Control and Body Coordination domains and AMPS Motor Skills and Process Skills subscales after the program ended.
Discussion
The results indicate that motor skills intervention based on motor learning theory increases the functional performance of preschool children with ASD. This research provided three main findings: (1) Children in the MOTION–ASD group showed significantly greater improvements in BOT–2–BF Manual Coordination and Vineland–3 Motor Skills domain scores than those in the CO–EXC group; (2) scores on BOT–2–BF Fine Manual Control, Body Coordination, and point score for total motor skills and AMPS Motor Skills and Process Skills showed significantly greater improvements with time for both groups; and (3) many improvements in fine manual control, body coordination, and total motor skills and motor and process abilities in daily self-care performance made throughout the interventions were retained at the posttest and 4-wk follow-up.
This study built on the motor skills intervention results from Bremer et al. (2015) and Ketcheson et al. (2017), which showed promising effects on children’s motor ability. Previous studies have found that fundamental motor skills interventions could be effective at improving the object manipulation ability of children with ASD (Bremer et al., 2015; Ketcheson et al., 2017; Pan et al., 2017; Rafie et al., 2017). In this study, we found significant between-groups differences in scores on the BOT–2–BF Manual Coordination and Vineland–3 the Motor Skills domains. Significant improvements were seen among the MOTION–ASD group, supporting previous research. MOTION–ASD based on motor learning theory could benefit preschool children with ASD, especially in terms of manual coordination and overall gross and fine motor skills. One explanation might be that MOTION–ASD targets specific motor skills to foster better skills acquisition among children. The other explanation might be that the low therapist-to-child ratio in the intervention enhanced the use of feedback (Pan et al., 2017), was more intensive, and provided more structured and supportive opportunities for practicing skills (Bremer et al., 2015).
The two-way repeated-measures ANOVA indicated that time was a significant factor for motor skills and self-care performance, with combined groups, meaning that there were significant differences between the pretest, posttest, and follow-up assessments. We found statistically significant improvements in BOT–2–BF Fine Manual Control, Body Coordination, and total motor skills and AMPS Motor Skills and Process Skills scores for both groups after treatment. These results indicate that time involvement is critical because the children received the same dosage of interventions. In terms of previous research, Bremer et al. (2015) and El Shemy and El-Sayed (2018) demonstrated that young children with ASD who received the same dosage of the same intervention showed significant improvements in motor skills after treatment. In this study, the CO–EXC group also had significant improvements in motor skills and self-care performance. These results parallel the findings reported in previous empirical studies (Hilton et al., 2014; Pan et al., 2017). Pan et al. (2017) reported that children with ASD who received motor skills training combined with executive function training (i.e., inhibitory control and attention) had improvements in motor skills proficiency. This supports the benefit of cognitive-oriented motor skills training for preschool children with ASD. However, to date, no published studies have compared interventions with the same dosages based on different approaches. This study adds to what is known about the efficacy of two different motor interventions in enhancing the motor skills of preschool children with ASD. Both the MOTION–ASD and CO–EXC interventions provided significant benefits for preschool children with ASD in terms of their fine manual control, body coordination, and total motor skills.
Additionally, regardless of which intervention was applied, both motor skills interventions demonstrated positive effects on the functional performance of preschool children with ASD by providing an objective measurement of activity. These children increased their capacity to engage in self-care activities after the interventions. A Group × Time interaction was also observed in the Motor Skills domain of the Vineland–3, indicating that the effect of learned motor skills transferred or could be generalized to daily activities. The Motor Skills domain of the Vineland–3 is used to assess a child’s use of gross and fine motor skills in daily life (Sparrow et al., 2016). Previous research has indicated that motor skills (Jasmin et al., 2009) or visual–motor integration (Chi & Lin, 2021) and self-care performance are linked in young children with ASD. Our results show that preschool children with ASD in the MOTION–ASD group showed significantly improved gross and fine motor skills in daily activities. It is thus plausible to assume that improvement in fine and gross motor skills may lead to improvement in self-care performance. However, previous intervention studies have not directly examined the motor domain of adaptive behavior or self-care abilities. Only two studies have reported that children with ASD demonstrated an improvement in physical functionality in terms of overall life quality (Sarol & Çimen, 2015) and physical health (Toscano et al., 2018) after the application of a motor skills intervention. This result extends the current knowledge of the effect of interventions on motor-related functional performance.
Notably, neither group achieved significant improvements in strength and agility. The lack of an effect on strength and agility is inconsistent with previous studies (Pan et al., 2017; Rafie et al., 2017). One reason might be that the fitness training was not persistent in the intervention activities. The MOTION– ASD group mainly focused on fundamental motor skills acquisition. Although the CO–EXC group aimed to increase levels of physical activity, the activity dosage, speed, or energy expenditure was insufficient. Furthermore, our findings agree with those of Bremer et al. (2015), who reported that young children with ASD perceived no improvements in their adaptive behavior composite after the intervention. One potential reason for this finding may be the small sample size and sample characteristics. Among these preschool children with ASD, only 4 children had an adaptive behavior composite score of <70. It was difficult to improve this function in the short term when the children already had high baseline levels. Additionally, the adaptive behavior composite scores of the Vineland–3 may not have been sensitive to the minor changes that represented the overall adaptive behavior over a short period.
Although we used a rigorous triple-blinded RCT research design with a dose-matched group, the sample size was still small. Future studies should increase the sample size to conduct analyses of variance or analyses of covariance. Because children with ASD have global developmental delays, significant improvements might not be evident in all developmental domains after short-term interventions. Therefore, another limitation was that this study had a short-term RCT design. Although many of the children’s improvements in motor skills and self-care performance were retained from the posttest to the 4-wk follow-up, we were unable to draw conclusions about the long-term effects on their acquisition of motor skills and self-care ability. A long-term intervention program with follow-up tests is therefore warranted.
Implications for Occupational Therapy Practice
The findings of this study have several implications for pediatric occupational therapy practice: ▪ MOTION-ASD could benefit preschool children with ASD in terms of manual coordination ability and overall gross and fine motor skills. ▪ Occupational therapists could provide repetitive practice of the selected tasks and facilitate manual coordination ability and overall gross and fine motor skills. ▪ MOTION-ASD intervention did not show added value over the CO-EXC in self-care performance and other adaptive behaviors. Occupational therapists could provide both MOTION-ASD and CO-EXC interventions. ▪ We carried out rigorous tests of motor skills interventions that support ways to manage motor difficulties in children with ASD. Practitioners should consider providing preschool children with ASD with structured and strategic motor skills interventions that target specific motor skills and abilities.
Conclusion
This study was the first RCT with a rigorous triple-blinded and dose-matched comparison group design to examine motor skills performance, self-care performance, and adaptive behaviors among preschool children with ASD. Overall, the results showed that preschool children with ASD could benefit from the implementation of research-supported approaches to deliver motor skills interventions. Specifically, preschool children with ASD in the MOTION–ASD group showed significantly greater improvements in manual coordination ability and overall gross and fine motor skills than those in the CO–EXC group. However, the improvements on two standardized outcome measures were not evident in self-care performance and other adaptive behaviors, suggesting that the MOTION–ASD intervention did not show added value over the CO–EXC intervention. Further research in this area is necessary to gain a better understanding of the most effective means of delivering motor skill interventions.
Supplemental Material
Supplementary material for Efficacy of Motor Interventions on Functional Performance Among Preschool Children With Autism Spectrum Disorder: A Pilot Randomized Controlled Trial
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2023.050283.pdf for Efficacy of Motor Interventions on Functional Performance Among Preschool Children With Autism Spectrum Disorder: A Pilot Randomized Controlled Trial by Yu-Ru Jin, Yi-Shan Sung, Chia-Lin Koh, Shin Ying Chu, Hsiu-Ching Yang and Ling-Yi Lin in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This study was supported by grants from National Science and Technology Council (NSTC 109-2221-E-006-142 and 110-2511-H-006 -010-MY2). We thank the children and parents who participated in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.