
Abstract
The Cognitive Orientation to daily Occupational Performance approach can be a cost-effective, short duration, task-oriented treatment for stroke patients.
A stroke occurs when a blood vessel that carries oxygen and nutrients to the brain is either blocked by a clot or ruptures, causing damage that can affect how the body works (American Stroke Association, 2022). According to the World Stroke Organization (2022), 1 in 4 people over age 25 will have a stroke in their lifetime. After a stroke has occurred, there is permanent brain damage, which may lead to long-term disability (National Heart, Lung, and Blood Institute, 2020).
Occupational performance is the execution of daily occupations resulting from the dynamic transaction among the person, the occupation, and the environment (American Occupational Therapy Association, 2020). Approximately 75% of stroke survivors experience difficulties with the occupational performance of everyday activities, such as dressing, feeding, sleep, and work (Sturm et al., 2002). Occupational therapists involve clients in activities of daily living (ADLs) and maximize their independence by helping them develop skills and confidence or using assistive technology, if necessary (American Occupational Therapy Association, 2021). The therapeutic approaches available are often categorized as top-down or bottom-up. The literature shows that top-down approaches are more effective than bottom-up ones in improving ADL function because they focus on occupations that are meaningful to the client (Weinstock-Zlotnick & Hinojosa, 2004) and promote more realistic and functional goal setting.
The ultimate goal of rehabilitation is to help people progress out of the therapeutic environment and function well in their daily lives (Krakauer, 2006), but most interventions do not explicitly address generalization and transfer to the real world (Zelinksi, 2009). Although clients usually improve in specific skills over the course of therapy, the challenges they encounter after leaving therapy lead to considerable barriers to further progress (Houldin, 2018). Ahn (2016) conducted a review of the types of approaches most commonly used to address occupational performance in stroke patients; the findings revealed that most interventions do not take into consideration the client’s context, which contradicts the definition of occupational performance.
The Cognitive Orientation to daily Occupational Performance (CO-OP) is a top-down approach developed in the early 1990s, mainly for children with developmental coordination disorder (Missiuna et al., 2001). Since then, its use has expanded to include pediatric and adult populations with cerebral palsy, traumatic brain injury, and stroke. The principal characteristic of CO-OP is its client-centered approach. Second, it is aimed at training the client in the execution of the task itself, as opposed to improvement in body functions and skills that has traditionally been the focus of neurodevelopmental approaches (ICANCOOP, 2022). The third feature of the CO-OP is the concept of problem-solving, that is, guiding clients to solve problems related to execution of a particular task, using the global cognitive strategy goal–plan–do–check and thus helping the client discover domain-specific cognitive strategies (ICANCOOP, 2022). Therefore, skill acquisition and generalization of skills and strategies in everyday life are the main objectives of the CO-OP.
The CO-OP includes trained and untrained goals. Trained goals are self-selected activities that clients identify as the primary ones on which to focus the CO-OP intervention. Untrained goals are self-selected activities that are not addressed during the CO-OP (McEwen et al., 2015). Untrained goals are used to assess the degree of generalization and transfer of the acquired skills.
The CO-OP incorporates various features to support generalization, that is, variable practice, guided discovery, a focus on strategy use, and self-efficacy (Polatajko et al., 2001). Statistically significant and clinically important improvements have been observed in children with developmental coordination disorder (Polatajko et al., 2001), autism spectrum disorder (Rodger et al., 2007), and attention deficit hyperactivity disorder (Gharebaghy et al., 2015).
Borujeni et al. (2019) conducted a scoping review that aimed to summarize previous studies of various experimental designs and present the characteristics of CO-OP protocols used in a heterogeneous adult population, including stroke, traumatic brain injury, and cognitive difficulties. Conclusions about the effectiveness of these protocols have not been made, as clearly stated by the authors. Ahn (2017) performed a systematic review that aimed to describe the goals and intervention protocols of CO-OP studies of adults with stroke published between 2005 and 2015. The review included studies of various experimental designs, of which 2 were controlled trials and 5 were case studies or case series. Ahn (2017) concluded that the goals set by clients were mostly related to ADLs and instrumental activities of daily living (IADLs), but the actual impact of the CO-OP on occupational performance was not within the scope of the review.
The present review was conducted to systematically investigate the evidence for the impact of the CO-OP on the occupational performance of adults after stroke. More specifically, the intent was to explore both the statistical significance and the clinical importance of previous studies’ findings and to investigate any evidence available with regard to generalization of gains and skills transfer.
Method
Search Strategy
An electronic database search of PubMed, SCOPUS, ScienceDirect, OTseeker, and EBSCO was conducted by one of the two review authors (Antria Kiriakou) in consultation with a university librarian. The reference lists of the included studies were also searched to identify any additional relevant articles. The search terms used in this review to capture pertinent studies are listed in Table A.1 of the Supplemental Material (available online with this article at https://research.aota.org/ajot). Because of the limited number of studies related to the research question, no start date was set; all studies that met the inclusion criteria and were published through December 2021 were included.
Inclusion and Exclusion Criteria
Studies were included if they met the following four criteria: (1) randomized controlled trial (RCT) or pilot RCT; (2) participants >18 yr old with at least one stroke incident in their medical history; (3) an intervention adhering to CO-OP principles, as reported by Polatajko et al. (2001); and (4) outcome measures that assessed occupational performance. Studies were excluded if they were published in any language other than English.
Data Extraction and Synthesis
The titles and abstracts of the identified studies were screened to determine the ones potentially eligible for inclusion. The full-text versions of these articles were retrieved and assessed for eligibility. Studies that did not meet the inclusion criteria were excluded. Key information relating to the level of evidence, study design, inclusion criteria, participants, intervention and control groups, outcome measures, and key results were extracted by Antria Kiriakou and double-checked by Pavlina Psychouli. There were no cases of disagreements between the authors.
Analysis
Each study was assessed for risk of bias using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2; Sterne et al., 2019). For each study, we determined whether the risk of bias was low or high or whether there were some concerns. Levels of evidence were assigned on the basis of standards developed by the Oxford Centre for Evidence-Based Medicine (2009). Levels of evidence range from Level 1a (systematic review of homogeneous RCTs with or without a meta-analysis) to Level 5 (expert opinion without explicit critical appraisal).
As described in the guidelines of the U.S. Preventive Services Task Force (2012), we determined the overall strength of evidence by analyzing each study’s design, findings, and risk of bias. Levels of certainty can be summarized as follows: ▪ Strong strength of evidence: Indicates two or more Level 1a or Level 1b studies with consistent results from well-designed, well-conducted studies. ▪ Moderate strength of evidence: Indicates at least 1 Level 1a or Level 1b high-quality study or multiple moderate-quality studies that provide sufficient evidence to determine health outcomes, but confidence in the estimate is constrained. ▪ Low strength of evidence: Indicates a small number of low-level studies, flaws in the available studies, and some inconsistency in findings across individual studies.
Results
Study Selection
The search of databases identified 772 articles. After the removal of duplicates and title and abstract screening, the full text of 8 potentially relevant articles was reviewed (Ahn et al., 2017; McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Skidmore et al., 2014, 2015; Song et al., 2019; Wolf et al., 2016). Seven of these articles were found to meet the inclusion criteria (Supplemental Table A.2). One was excluded because it was the older version of an already-included study (Skidmore et al., 2014). No additional eligible studies were identified through reference list searches. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021) flow diagram is presented in Figure 1.
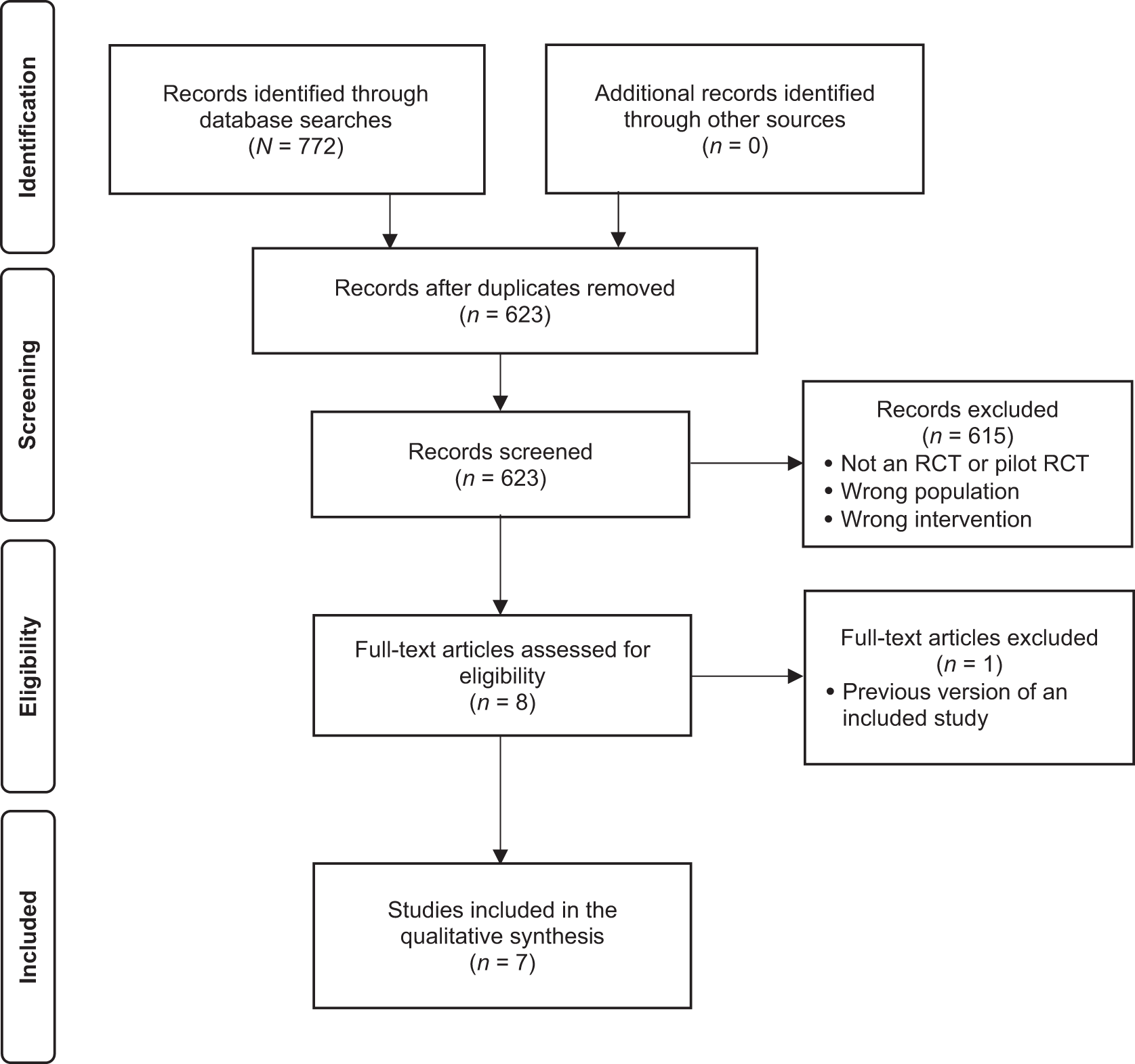
Flow of articles through the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) systematic review process.
Study Characteristics
Characteristics of the included studies are presented in Supplemental Table A.2. Five Level 1b RCTs, conducted in Canada, Korea, and the United States, were included (Ahn et al., 2017; McEwen et al., 2015; Skidmore et al., 2015; Song et al., 2019; Wolf et al., 2016), along with 2 Level 2b pilot RCTs, conducted in Canada (Polatajko et al., 2012; Poulin et al., 2017). Studies included patients with acute and subacute stroke (<6 mo after the incident; McEwen et al., 2015; Skidmore et al., 2015; Wolf et al., 2016) and chronic stroke (>6 mo after the incident; Polatajko et al., 2012; Poulin et al., 2017; Song et al., 2019). One study did not mention whether their participants were in the acute or chronic phase (Ahn et al., 2017).
In all studies, the intervention groups received the CO-OP. In 4 studies (Ahn et al., 2017; McEwen et al., 2015; Polatajko et al., 2012 ; Wolf et al., 2016), the control groups received conventional occupational therapy. In the study conducted by Song et al. (2019), the control group received task-specific upper extremity training, and in the study by Poulin et al. (2017) they received computer-based executive function training. Finally, in the study conducted by Skidmore et al. (2015), the control group participated in what the authors called “attention control sessions,” which were designed to control the nonspecific effects of the CO-OP (i.e., dose and attention) by using workbook and open-ended questions focused on rehabilitation goals, activities, and experiences during CO-OP implementation.
Four studies included follow-up measurements: McEwen et al. (2015) at 3 mo postintervention or after discharge from the occupational therapy program, Poulin et al. (2017) at 1 mo postintervention, and Wolf et al. (2016) at 3 mo postintervention. Skidmore et al. (2015) reported findings at 3 and 6 mo after baseline assessment.
Risk of Bias
The quality appraisal of the studies is presented in Supplemental Table A.3. All articles were associated with a high risk of bias. The most common bias risk identified was lack of blinding procedures for the interventions and outcome measurements and a lack of follow-up measurements.
Study Outcomes
Trained Goals
The most common goals set by participants in the studies were related to ADLs and IADLs. Other frequently selected goals focused on leisure, social participation, and work.
All of the included studies measured occupational performance of trained goals using one or more of the following assessment tools: Canadian Occupational Performance Measure (COPM; Law et al., 2019), Performance Quality Rating Scale (PQRS; Martini et al., 2015), Stroke Impact Scale (SIS; Lin et al., 2010), FIMTM (Beninato et al., 2006), 1 and Assessment of Life Habits (LIFE–H; Noreau et al., 2004).
Five of the 7 studies used the COPM (Ahn et al., 2017; McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Song et al., 2019). Three of these studies showed statistical significance for both the Performance and Satisfaction domains postintervention (Ahn et al., 2017, p = .000; Poulin et al., 2017, p < .05; Song et al., 2019, p < .001). Polatajko et al. (2012) noted statistical significance only for the Performance domain (p = .02), whereas McEwen et al. (2015) did not detect statistically significant postintervention results (Performance, d = –0.1, 95% confidence interval [CI] [–0.8, 0.7]; Satisfaction, d = 0.1, 95% CI [–0.7, 0.9]). Poulin et al. (2017) and McEwen et al. (2015) included follow-up measurements; the first found statistically significant improvements in favor of the CO-OP (p < .05), but the latter did not reach statistical significance (Performance, d = 0.4, 95% CI [–0.5, 1.2]; Satisfaction, d = 0.1, 95% CI [–1.0, 0.8]).
Three of the 7 studies used the PQRS (Ahn et al., 2017; McEwen et al., 2015; Polatajko et al., 2012); 2 of these showed statistically significant improvements immediately postintervention (Ahn et al., 2017, p = .000; Polatajko et al., 2012, p = .02), in contrast to the third study (McEwen et al., 2015; d = 0.5, 95% CI [–0.4, 1.4]), which reached statistical significance at follow-up (d = 1.6, 95% CI [0.5, 2.7]).
Skidmore et al. (2015) used the FIM but reported numerical results only for the follow-up, when statistically significant improvements were demonstrated 3 mo (p = .006) and 6 mo (p = .004) after the end of intervention.
Poulin et al. (2017) used the LIFE–H in their study but did not demonstrate any statistically significant differences either postintervention (p > .05) or at follow-up (p > .05).
The SIS was used by Wolf et al. (2016) to evaluate occupational performance; they observed small to large effect sizes postintervention and at follow-up for ADLs, the Hand Function domain, the Mobility domain, and the SIS in general. However, all of these results were statistically insignificant (Supplemental Table A.4).
For the COPM, the mean difference should be ≥2 points to indicate clinical importance (COPM, 2022), which was the case for the studies conducted by Ahn et al. (2017), Polatajko et al. (2012), and Poulin et al. (2017). Poulin et al. (2017) and McEwen et al. (2015) demonstrated clinical importance at follow-up, whereas Song et al.’s (2019) results did not reach clinical importance (Supplemental Table A.4).
For the PQRS, effect sizes >1, suggesting that the observed changes in occupational performance, were deemed clinically important (Martini et al., 2015). This applied only at follow-up and not postintervention for the study conducted by McEwen et al. (2015; Supplemental Table A.4).
In contrast, clinical importance for the FIM was associated with differences >3 points (Beninato et al., 2006), which was the case at both the 3- and 6-mo follow-ups in Skidmore et al.’s (2015) study (Supplemental Table A.4).
On the SIS, a change must be >5.9 for the ADL domain, >4.5 for the Mobility domain, and >17.8 for the Hand Function domain to be considered clinically important (Lin et al., 2010). In Wolf et al.’s (2016) study, clinically important differences were observed in the ADL and Mobility domains both postintervention and at follow-up and in the Hand Function domain only at follow-up (Supplemental Table A.4).
On the LIFE–H, the minimal detectable change, which may be correlated with the clinically important change, is 0.68 (Noreau et al., 2004). In Poulin et al.’s (2017) study, this was reached only at follow-up (Supplemental Table A.4).
In summary, all of these studies present a variability in effects of the CO-OP on trained goals, which in many cases are statistically insignificant but clinically important and vice versa.
Untrained Goals
Three of the 7 studies tested untrained goals in addition to the trained ones. The COPM was used by all 3 studies, but only Ahn et al. (2017) found statistically significant improvements in both the Performance (p = .001) and Satisfaction (p = .004) domains. Poulin et al. (2017) showed statistical significance only for COPM Satisfaction postintervention (p < .05) and at follow-up (p < .05), and McEwen et al. (2015) showed no statistical significance (Supplemental Table A.4). The PQRS was shown to have statistically significant differences in favor of the CO-OP by Ahn et al. (2017; p = .010) and by McEwen et al. (2015; d = 1.2, 95% CI [0.1, 2.2]) postintervention. However, the latter research group did not show the statistically significant results to be retained at follow-up (d = 1.1, 95% CI [–0.1, 2.3]).
In terms of clinical importance, Ahn et al. (2017) showed such improvements in COPM postintervention, and McEwen et al. (2015) showed them at follow-up. However, McEwen et al.’s (2015) postintervention results and Poulin et al.’s (2017) results at both postintervention and at follow-up did not reach clinical importance (Supplemental Table A.4). Regarding PQRS, both postintervention and follow-up changes were clinically important in McEwen et al.’s (2015) study (Supplemental Table A.4).
In total, the small number of studies that attempted to evaluate untrained goals yielded results that are inconclusive with respect to both statistical significance and clinical importance.
Discussion
In this systematic review, which aimed to explore the impact of the CO-OP on the occupational performance of adults after stroke, 5 Level 1b studies and 2 Level 2b studies with a total of 191 participants satisfied the inclusion criteria and were included. All studies were found to be associated with a high risk of bias, mainly because of the small sample numbers, which ranged from 8 to 49, and a lack of blinding procedures and follow-up measurements. Statistical significance was shown in many cases, although there was considerable variation among studies as well as between statistical significance and clinical importance of the findings. Most studies did not evaluate untrained goals, and the ones that did yielded variable results.
The COPM and PQRS are directly linked to the scope of the CO-OP, and this is why 5 out of the 7 studies used one or both of these tools. The complementary use of the PQRS is strongly suggested given that it provides a more objective assessment of the actual rather than the perceived performance of the specific activities that have been identified by the COPM. Three studies—Wolf et al. (2016), Skidmore et al. (2015), and Poulin et al. (2017)—used the FIM, SIS, and LIFE–H, respectively, to measure occupational performance. With the exception of the FIM, the rest did not show statistical significance but reached clinical importance postintervention or at follow-up. Using a battery of outcome measures may add reliability to the findings and help researchers explore areas other than occupational performance, which may also be targeted by the CO-OP.
We should note that a statistically significant change is not synonymous with a clinically important one. A clinically important change is considered the smallest change that may be perceived as beneficial to the person (Lin et al., 2010). The difference between these two values for an outcome measure is more than evident in the findings of the present review, in which some studies with statistically significant results (Poulin et al., 2017; Song et al., 2019) did not reach clinical importance. What is more interesting, though, is that some other studies (McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Wolf et al., 2016) did not demonstrate statistical significance even though the results were clinically important. This discrepancy in findings may be attributed to the small sample numbers and the use of means in the statistical analysis as opposed to medians, which would probably be more appropriate to illustrate the real individual differences in such small and diverse groups. The high incidence of underpowered studies in the field of rehabilitation was highlighted by Kinney et al. (2020), who concluded that the typical sample size used is insufficient to detect statistical significance.
Untrained goals were tested in only 3 of 7 studies, making it difficult to judge the effectiveness of the CO-OP for skill generalization. In most cases, these 3 studies showed statistically significant and clinically important results, but more methodologically sound studies are needed to form a clearer picture of the intervention’s impact on untrained tasks.
In most studies, the goals set by participants were related to ADLs or IADLs. McEwen et al. (2015) presented the widest variability in terms of the number of goals and occupational domains, but there is no indication that results might have been affected by the type of occupational domain.
The studies included in this review present several methodological limitations, as identified by the RoB 2. These limitations include small sample sizes, which were evident in almost every study; incomplete data for specific outcome measures; or inconsistent use of measures across evaluation phases (McEwen et al., 2015; Polatajko et al., 2012; Wolf et al., 2016), which may have led to bias (Sterne et al., 2019).
Because the CO-OP is a relatively new approach, most studies were pilot studies, case studies, or case series. Because one of the main concerns of the CO-OP is skills generalization and transfer to the real world, participants should be evaluated after multiple and longer follow-up periods to explore the long-term effects of the CO-OP. Finally, researchers should ensure that the allocation of participants is blinded and that group characteristics are similar at the beginning of the interventions so that results will be comparable.
Implications for Occupational Therapy Research
The findings of this systematic review have some implications for future research on the CO-OP in relation to stroke. RCTs that are adequately powered to detect statistically significant results should ▪ include standard long-term follow-up assessment procedures and timelines to explore the possibility of skills retainment, ▪ explore untrained goals to provide an insight into the potential for skills generalization, ▪ address clinically important outcomes in addition to statistically significant ones, and ▪ use appropriate statistical methods when sample numbers are small.
Conclusion
The CO-OP is a promising client-centered and occupation-based approach that may improve occupational performance after stroke, an area that is rarely the real focus of most neurorehabilitation approaches. The findings of this review revealed statistically significant and clinically important results after the CO-OP but also highlighted the need for future methodologically sound studies that will explore its clinical impact and address one of its most unique characteristics: the potential for skills generalization.
Supplemental Material
Supplementary material for Effects of the CO-OP Approach in Addressing the Occupational Performance of Adults With Stroke: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050131.pdf for Effects of the CO-OP Approach in Addressing the Occupational Performance of Adults With Stroke: A Systematic Review by Antria Kiriakou and Pavlina Psychouli in The American Journal of Occupational Therapy
Footnotes
1FIMTM is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
*Indicates studies included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.