
Abstract
Children’s behavioral problems are an important consideration for occupational therapy practitioners working with preschoolers. The results of this study suggest that relationships exist between behavioral problems, sensory processing, and sleep among preschoolers.
Children’s behavioral problems are an important concern for their families and occupational therapy practitioners. It has been established that emotional and behavioral issues begin in childhood (Egger & Angold, 2006). Previous research suggests that behavioral issues and difficulties with sensory processing and sleep are related among children. Sensory processing is the ability to organize and interpret information received through the senses to produce a response, which is the interaction between the person’s neurological threshold and self-regulation of behavior (Dunn, 1997).
Several previous studies have shown that these patterns of sensory processing occur in all age groups, from infancy to older adulthood, and that people with neurodevelopmental disorders, such as attention deficit hyperactivity disorder and autism spectrum disorder, have distinct and more intense patterns of sensory processing (Delgado-Lobete et al., 2020; Dellapiazza et al., 2021; Wang et al., 2019). It has been established that sensory processing difficulties are associated with behavioral issues among children (Mulligan et al., 2021). For instance, sensory hypersensitivity is considered a risk factor for anxiety among children (Carpenter et al., 2019).
Sleep problems among children can lead to externalizing and internalizing behavior problems (Quach et al., 2018; Shanahan et al., 2014). A common distinction is made between externalizing and internalizing behavioral problems among children (Eisenberg et al., 2001). Externalizing behavior problems include aggression, impulsivity, hyperactivity, and delinquency, among others (Eisenberg et al., 2001; Holmbeck et al., 2008). Internalizing behavior problems primarily affect the internal world of a person, for example, reclusiveness, somatic pain and anxiety, inhibition, or depressive behavior (Eisenberg et al., 2001; Gilliom & Shaw, 2004). Additionally, 10% to 30% of children are reportedly affected by sleep disorders (Deshpande et al., 2022; Maski & Owens, 2016), highlighting the need for effective interventions to treat childhood sleep problems.
Research has established a link between sleep issues and sensory processing patterns (Rajaei et al., 2020 ; Vasak et al., 2015). For example, Rajaei et al. (2020) reported that sensory processing patterns are moderately correlated with sleep habits among children. When integrating the aforementioned information, we presumed that children’s sensory processing, sleep, and problem behaviors are interrelated. Thus, in this study we aimed to develop a structural causal model (SCM) of childhood behavioral problems triggered by the close relationship between sensory processing difficulties and sleep problems and to investigate the various ways in which these behavioral problems manifest. Moreover, a previous study (Reynaud et al., 2018) indicated that symptoms of sleep problems are different between externalizing and internalizing behavior problems. Therefore, we also attempted to elucidate sensory processing and sleep problems related to externalizing and internalizing problem behaviors, respectively.
Method
Participants and Procedures
After receiving approval from our university’s institutional review board (Approval No. 18-34), we began recruiting study participants. This research was conducted in accordance with the World Medical Association’s Code of Medical Ethics (https://www.wma.net/policies-post/wma-international-code-of-medical-ethics/).
The study included 168 children. Our target population consisted of children ages 3–5 yr enrolled in a preschool or accredited kindergarten (four facilities in total) in a Japanese prefecture. With the assistance of educators, we provided children’s parents with an informed consent form and a withdrawal form as well as copies of the Short Sensory Profile–Japanese version (SSP–J; Tani et al., 2015), the Japanese Sleep Questionnaire for Preschoolers (JSQ–P; Shimizu et al., 2014), and the Child Behavior Checklist for Ages 1.5–5 (CBCL; Funabiki & Murai, 2017). On receipt of the signed informed consent form, consent to participate in the study was recognized.
Measures
Short Sensory Profile–Japanese Version
The Sensory Profile (SP; Dunn, 1999) is a tool that was developed to comprehensively assess sensory processing issues among children ages 3–10 yr and is now widely used worldwide. SSP–J is the standardized Japanese language short form of the SP (Tani et al., 2015). This instrument is a parent-reported questionnaire containing 38 items organized into various scales based on seven section scores: tactile sensitivity, taste/smell sensitivity, movement sensitivity, under- responsiveness/sensation seeking, auditory filtering, low energy/weakness, and visual/auditory sensitivity. The greater the section score, the greater the level of difficulty.
Japanese Sleep Questionnaire for Preschoolers
The JSQ–P was developed and standardized as a culturally relevant sleep assessment scale for Japanese preschoolers ages 3–6 yr. According to the manual, the short form of the SP should be completed by a parent or another person with a thorough understanding of the child’s sleep. This instrument uses a 6-point scale (1 = strongly disagree, 6 = strongly agree) for 39 questions selected on the basis of factor analysis and fundamental characteristics, such as sleep and wake-up time. The total score ranges between 39 and 234, with higher scores indicating an increased risk for sleep disorders. It also includes 10 subitems as symptoms of sleep disorders: restless legs syndrome (RLS)–motor, RLS–sensory, obstructive sleep apnea syndrome (OSAS), parasomnias, insomnia or circadian rhythm disorders, morning symptoms, excessive sleepiness, daytime behavior, sleep habits, and insufficient sleep. Each item has a cutoff value.
Child Behavior Checklist for Ages 1.5 to 5
The CBCL is a globally accepted survey that allows parents to evaluate their children’s mental health and behavior from multiple perspectives (Achenbach, 2000). A standardized Japanese-language version of the CBCL has been developed and subsequently modified to include values typical of Japanese children ages 1.5–5 yr (Funabiki & Murai, 2017). The CBCL consists of subscales for externalizing and internalizing behavior problems, which include the following symptoms: (1) externalizing: attention problems and aggressive behavior and (2) internalizing: emotional reactivity, anxiety and depression, somatic complaints, and withdrawal.
Data Analysis
Stage 1: Extracting the Common Factor According to Exploratory Factor Analysis
To select important variables and exclude unnecessary variables, we extracted similar variables from the SSP–J and JSQ–P through factor analysis using the principal factor method (according to the Kaiser–Guttman rule). We then investigated the possible correlations between these variables using the direct oblimin method. Variables with a factor loading of ≥.4 were immediately selected, whereas those with a factor loading of ≥.3 or <.4 were excluded or included, according to discussions among the study investigators.
Stage 2: Structural Equation Modeling Analysis
We expressed our hypothetical model by using a covariance structure analysis of common factors extracted by the principal factor analysis in Stage 1, along with the variables of age and sex. Next, we evaluated the goodness of fit for the model using the goodness-of-fit index (GFI) and the root-mean-square error of approximation (RMSEA) to the coefficient. We then calculated the standardized coefficient (hereafter, path coefficient) to determine the relationships between the variables. Standardized path coefficients range from −1 to 1, with higher absolute values indicating stronger influence. In addition, we performed subanalyses with internalizing and externalizing behavior problems as outcome variables to determine the relationships between variables in each model on the basis of their respective path coefficients. All statistical data were analyzed with IBM SPSS Statistics (Version 27.0) and Amos (Version 28.0); probability values of <5% were considered significant.
Results
Of the 602 children whose parents we contacted for study participation, 229 gave informed consent (participation rate = 38.0%). However, we excluded 34 children not within the age bracket specified by the three questionnaires, 16 children with missing survey data, and 11 children diagnosed with a developmental disorder during presurvey screening. Thus, this study ultimately included 168 children. The mean age of the study population was 4.6 yr (SD = 0.6), and 85 children (50.6%) were female. Moreover, of the 168 parents who provided the survey responses, 161 were mothers (95.8%), 6 were fathers (3.6%), and 1 was a grandparent (0.6%).
Table 1 enumerates the results of the factor analysis. We extracted four factors from 13 selected survey items, and one item of SSP–J and three items of JSQ–P were excluded from further analysis. The first factor consisted of two items from the SSP–J and two items from the JSQ–P, designated by the term attention deficit after a discussion by an expert panel of three pediatric occupational therapy practitioners. The second factor included two items of the JSQ–P, designated as RLS symptoms. The third factor consisted of three items from the JSQ–P, designated as sleep problems. Last, the fourth factor included four items from the SSP–J, designated as sensory sensitivity. The Kaiser–Meyer–Olkin measure was .718, and Bartlett’s sphericity test result was p < .001, demonstrating that our factor analysis is valid.
Exploratory Factor Analysis (Principal Axis Factoring, Direct Oblimin Rotation)
Note. Kaiser–Meyer–Olkin measure = .718; Bartlett’s sphericity tests, p < .001. RLS = restless legs syndrome.
aItem on the Short Sensory Profile–Japanese version.
bItem on the Japanese Sleep Questionnaire for Preschoolers.
Our SCM was developed on the basis of the structural equation modeling analysis of factors derived from factor analysis as well as the age and sex of the target children. Figure 1 illustrates our SCM of difficulties with sensory processing and sleep problems that can lead to behavioral issues among preschoolers. The final structural equation modeling analysis had an acceptable goodness of fit (GFI = .862, RMSEA = .087). With path coefficients of .65, .23, and .18, the model demonstrated the direct effects of attention deficit, sensory sensitivity, and sleep problems on behavioral problems. Indirect effects on behavioral problems of sensory sensitivity, sleep problems mediated by attention deficit, and RLS symptoms mediated by sleep problems were also demonstrated. The estimated total effect, which comprises the sum of direct and indirect effects on behavioral problems, was the largest with an attention deficit of .65. Although the direct effects of sensory sensitivity and sleep problems were minor at .23 and .18, respectively, the indirect effects via attention deficit resulted in total effects of .62 and .41, respectively, with a certain degree of influence on behavioral problems.
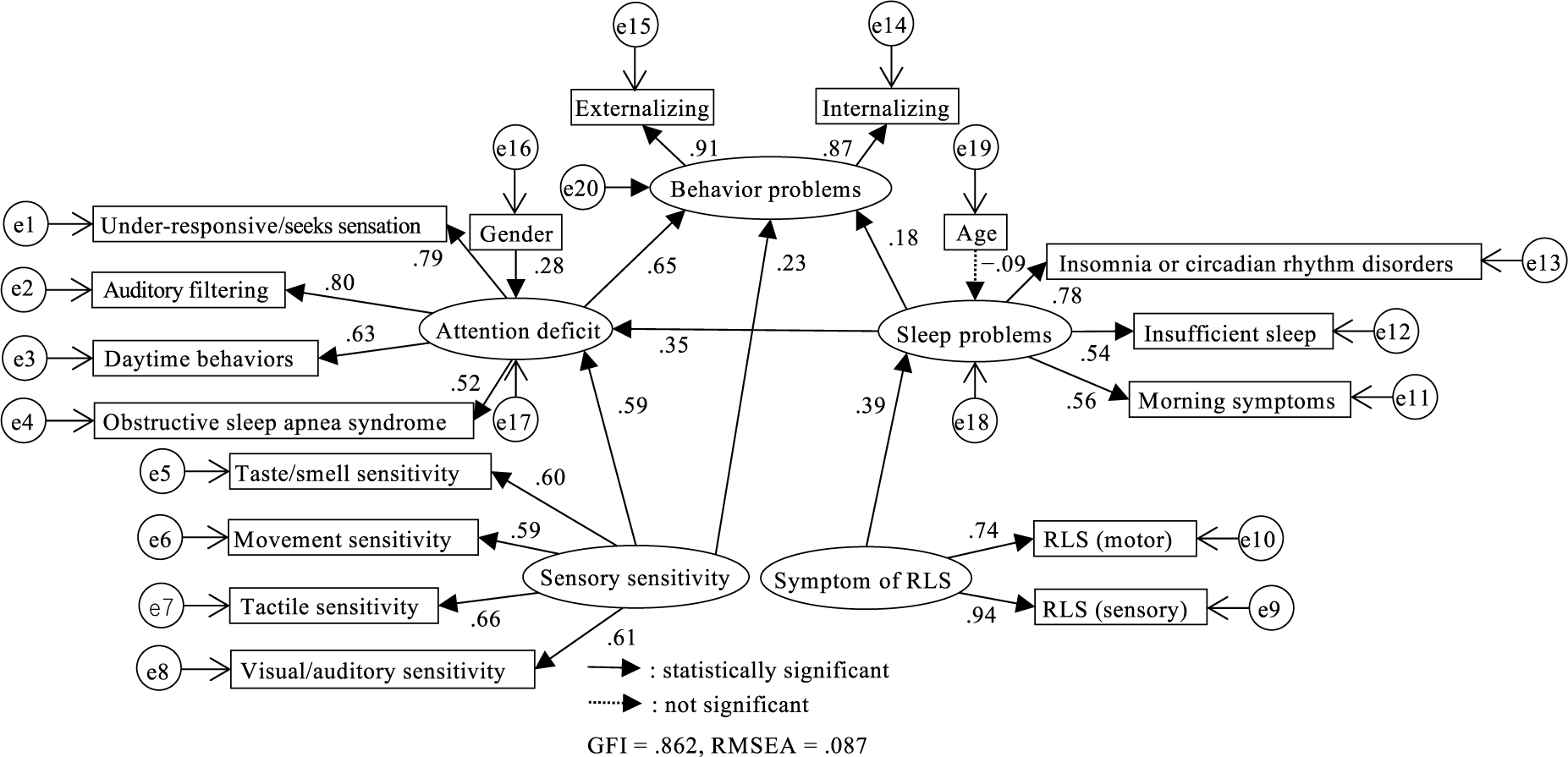
A causal model of sensory processing traits and sleep-affecting behavioral problems among children.
Figures 2 and 3 depict the SCMs derived from the findings of subanalyses that used externalizing and internalizing behavior problems, respectively, as outcome variables. In the SCM with externalizing behavior as an outcome variable (GFI = .882, RMSEA = .080), no significant difference was found between the enhanced direct effects of attention deficit and sensory sensitivity on externalizing behavior, whereas sensory sensitivity had a diminished direct effect (path coefficients = .74 and .03, respectively). Conversely, the SCM that used internalizing behavior as the outcome variable (GFI = .882, RMSEA = .079) revealed the direct effects of sensory sensitivity, attention deficit, and sleep problems on internalizing behavior, with path coefficients of .45, .37, and .19, respectively. In both models, sensory sensitivity and sleep problems indirectly contributed to behavioral problems by influencing attention deficits.
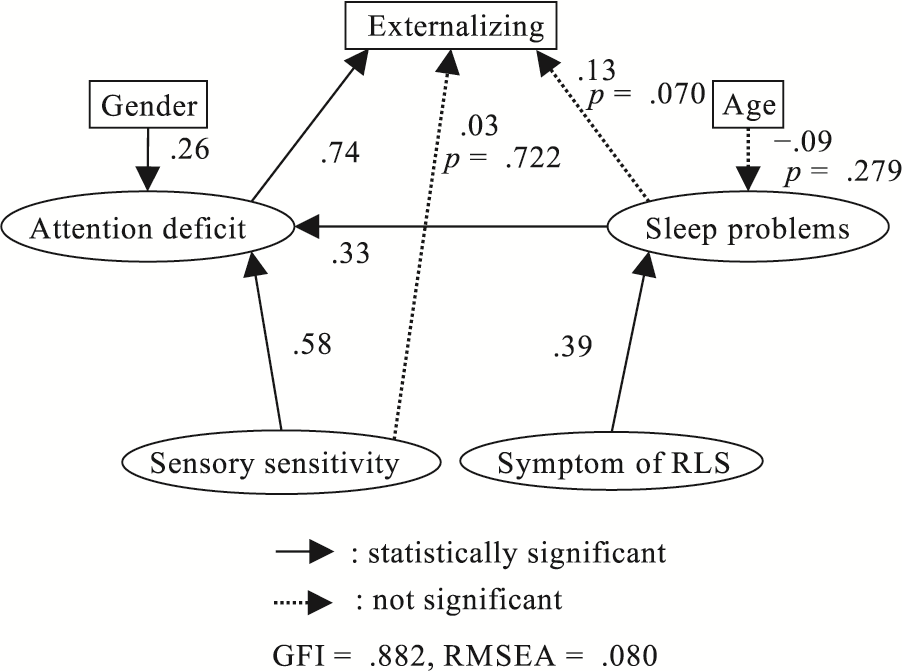
Causal model in which the externalizing subscale was used as the outcome variable.
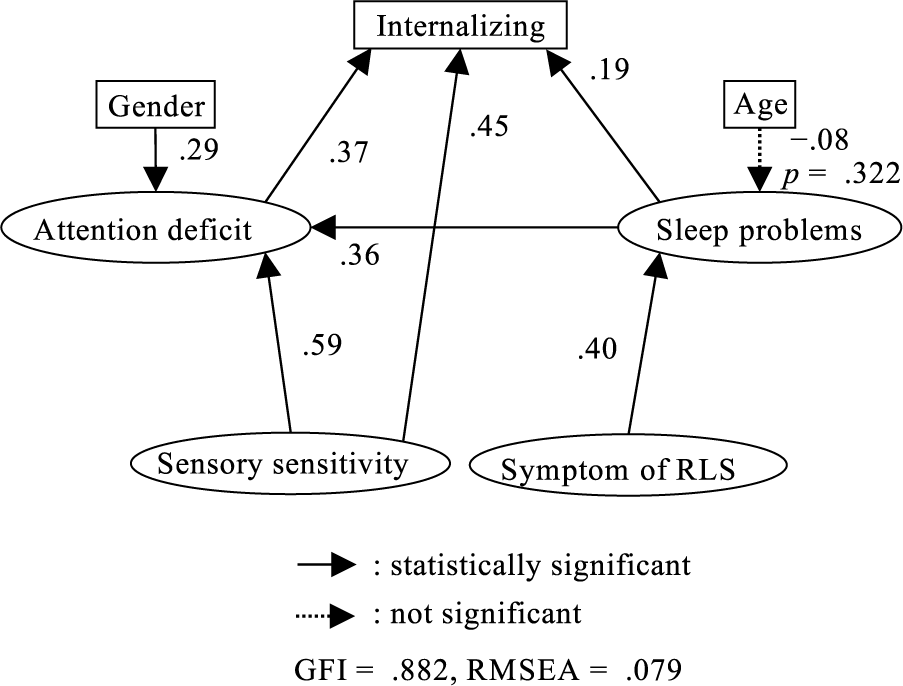
Causal model in which the internalizing subscale was used as the outcome variable.
Discussion
In this study, the first factor used in the factor analysis included two items from the SSP–J and two items from the JSQ–P, indicating that despite being developed for different purposes, these two assessment instruments share commonalities. On the basis of how the questions in each item were phrased, this factor was dubbed “attention deficit”: “Seeks all types of movement, thus interfering with daily routines” in the SSP–J and “Restless during the day” in the JSQ–P. In addition, the OSAS variable was chosen despite its relatively low factor loading. In addition to the core symptoms of respiratory events (i.e., snoring and labored breathing during sleep), the American Academy of Sleep Medicine (2014) includes daytime sleepiness and hyperactivity as diagnostic criteria for pediatric OSAS. The expert panel may have selected these factors as common factor components on the basis of these criteria.
Our results revealed that the four factors derived from factor analysis have direct or indirect effects on behavioral problems. Moreover, the results of this study indicated that although the direct effects of sensory sensitivity and sleep problems on behavioral problems were small, both influenced the attention deficit and thus had a relatively large overall impact on patients. This finding highlights the need for assessment and intervention for sensory sensitivity and sleep problems when preventing and ameliorating childhood behavioral problems. The results of our SCM subanalyses, which used the two types of behavioral problems (i.e., externalizing and internalizing behaviors) as outcome variables, deserve special consideration. In the SCM, with externalizing behavior as the outcome variable, sensory sensitivity and sleep issues had indirect effects on externalizing behavior via attention deficit.
Consequently, sensory sensitivity and sleep issues can contribute to externalizing behaviors if the symptoms of attention deficit are exacerbated. Moreover, the SCM that used internalizing behavior as the outcome variable demonstrated the direct effects of sensory sensitivity and sleep problems on internalizing behavior. Sensory sensitivity has been linked to anxiety among children (Carpenter et al., 2019). In a meta-analysis, sleep quality was associated with depression and anxiety among children (Becker et al., 2017). Consequently, our SCMs can be interpreted within clinical settings. Preventing or mitigating the severity of depression and anxiety among preschoolers can be accomplished by limiting their exposure to stimuli that can cause sensory hypersensitivity and implementing interventions that address improper sleep habits.
Limitations
This study has several limitations. First, given the low participation rate in this study, the generalizability of the results is questionable. However, given that the study sample results are comparable with the published reference values for the SSP–J and CBCL (Funabiki & Murai, 2017 ; Tsujii, 2015), we have not observed any specific issues in drawing general conclusions from the findings. Second, SCMs do not account for the potential of unmeasured confounding variables. For instance, parenting styles have been identified as a factor in behavioral problems among preschoolers (Berkien et al., 2012 ; Pan et al., 2021). Although we opted to exclude parenting styles in the scope of our surveys because of the risk of lower response rates associated with more survey questions, the goodness of fit of our SCMs would likely be improved if parenting styles were to be incorporated. Third, because this study was performed in Japan, it is expected that culture influences children’s sleeping habits. Therefore, it is difficult to generalize this study’s findings to other nations.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: ▪ Sensory processing and sleep status are important considerations when addressing behavioral problems among preschoolers. ▪ Externalizing behavior can be affected by attention deficit, and attention deficit may be related to sensory sensitivity and sleep problems. ▪ Internalizing behavior can be affected by sensory sensitivity, attention deficit, and sleep problems. Therefore, it can be mitigated by preventing preschoolers from being exposed to unpleasant sensations and improving their sleep behavior.
Conclusion
For the final path analysis of our SCM, on the basis of the hypothesis that sensory processing difficulties and sleep problems are closely related and may cause behavioral issues among preschoolers, an acceptable goodness of fit was observed. Therefore, sensory processing and sleep must be accurately evaluated to ameliorate their behavioral issues. In addition, the SCMs for externalizing and internalizing behavior problems revealed that four latent variables (attention deficit, sensory sensitivity, sleep problems, and RLS symptoms) have direct or indirect effects on the onset of externalizing or internalizing behavior.