
Abstract
The results of this study showed positive outcomes for a reablement intervention that focuses on goal-oriented instrumental activities of daily living for patients with stroke.
Participation in activities of daily living (ADLs) is one of the primary goals of rehabilitation for patients with stroke. Restrictions in performing instrumental ADLs (IADLs) could decrease participation in activities at home and in the community, such as housekeeping, shopping, and walking outside (Tomioka et al., 2016). IADL performance is a crucial index representing the level of participation of patients with stroke. Patients with stroke experience different degrees of impairment in physical and cognitive function, which leads to their dependency in IADLs and restricts their social functions (Einstad et al., 2022; Tiznado et al., 2021). Inability to perform IADLs has also been found to be associated with increased mortality and poor recovery among patients with stroke (Seixas et al., 2019). IADL training is expected to enhance independence in IADLs at home and in the community for patients with stroke, but evidence to support its practice is needed.
ADLs contain three aspects: actual performance, ability, and self-perceived difficulty (Han et al., 2020). The aspect of actual performance describes what individuals actually do in their real environment. Assessing actual performance can help clinicians and researchers verify individuals’ degree of dependence in ADLs in real-life contexts. The aspect of ability refers to individuals’ capabilities to carry out ADLs. Assessing ability provides objective information on individuals’ physical incapability or capability to perform ADLs. The aspect of self-perceived difficulty refers to individuals’ perception of the level of difficulty they experience while attempting ADLs without assistance from others. Assessing self-perceived difficulty is beneficial in recognizing individuals’ need for assistance (Lee et al., 2014). Thus, assessing IADLs with these three aspects in mind could help clinicians understand individuals’ ADL status more comprehensively in IADL intervention.
Reablement, also called restorative care, is an intensive rehabilitative intervention (e.g., multiple visits) for people with limitations in carrying out daily activities that may last for 6 wk. The goal of reablement is to optimize the chances for living independently, to achieve a substantial life, and to decrease the need for assistance from others (Zingmark & Kylén, 2022). Compared with the traditional form of rehabilitation, reablement stresses resettling and restoring physical independence and social engagement in one’s community (Clotworthy et al., 2021). This intervention is based on a person-centered and goal-oriented approach that emphasizes clients’ thoughts about and the demands of daily activities. Reablement intervention has shown statistically significant improvement with a moderate effect size in the aspect of ability and small effect sizes in the aspects of actual performance and self-perceived difficulty for stroke patients’ performance of basic ADLs in the home environment (Han et al., 2020). To the best of our knowledge, no studies have investigated the effectiveness of reablement intervention on IADLs for patients with stroke. Therefore, the purpose of this study was to explore the effects of reablement intervention on IADL tasks taken from the three aspects of ADLs for people with stroke. We hypothesized that IADL reablement would produce benefits for patients with stroke in carrying out IADLs.
Method
Participants
We conducted a single-blinded, randomized crossover study. Patients with stroke were recruited from the Department of Physical Medicine and Rehabilitation at two hospitals in northern Taiwan. The inclusion criteria were (1) diagnosis of stroke; (2) age >20 yr; (3) slight to moderate severe disability (modified Rankin Scale score of 2–4); (4) ability to maintain a sitting position for 30 min; (5) ability to follow instructions; and (6) willingness to participate in this study and provide signed informed consent. The exclusion criteria were a diagnosis of dementia and a history of orthopedic disease or peripheral nerve injury. All participants provided written informed consent approved by the Ethics Review Board of the two hospitals. This study was registered with ClinicalTrials.gov (NCT04399759).
Procedures
Each participant received both interventions, IADL reablement and health education, for a 6-wk period, administered at the participant’s home or a community location. The order in which participants received the interventions (i.e., IADL reablement or health education first) was assigned randomly. The allocation sequence was produced from a random-number table using Excel software. Half of the sample was allocated to receive the IADL reablement intervention while the other half received health education intervention. The washout period between the two interventions was 4 wk. One examiner who was blinded to the participants’ allocation administered all measures. The examiner completed a 4-hr training to become familiar with the administrative procedures of the measures and the scoring criteria. The outcome measures were all standardized and included the Frenchay Activities Index (FAI), Lawton Instrumental Activities of Daily Living Scale (LIADL), Canadian Occupational Performance Measure (COPM) Performance score, and Participation Measure–3 Domains, 4 Aspects (PM–3D4D). The individualized and client-centered COPM was used to identify two to three IADL tasks as goals for each participant. The outcome measures were administered 4 times: at baseline, after the first intervention, after the washout period, and after the second intervention. To enhance consistency, a single occupational therapist provided the two interventions to all participants.
Interventions
The IADL reablement program consisted of goal- directed IADL training. It was administered for 50 to 60 min once a week for 6 wk, which was according to the actual implementation standard in Taiwan. The IADL reablement program was implemented in the participant’s home or community environment. In the first week, the occupational therapist confirmed the participants’ goals (i.e., IADL tasks), implemented one IADL task, and observed the participants’ difficulties performing that task. In the second week, participants received training in the IADL task. The occupational therapist observed participants’ performance, graded the task that challenged the participants, modified the method so that they could succeed, and provided strategies for carrying out the task. In the third to sixth weeks, participants received training in one to three IADL tasks. The occupational therapist modified the method and provided different strategies for carrying out the IADL tasks, if needed. Appendix A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot) provides an example of the IADL reablement program.
Approximately half of stroke-related deaths occur as a result of inadequate management of stroke risk factors (Avan et al., 2019). Health education about stroke, treatment, and services is important to reduce disability and improve quality of life for patients with stroke (Ding et al., 2022). The health education intervention consisted of 6 wk of one 30-min one-on-one health education session per week at the participant’s home. It included a specific topic for each week (first week, stroke types and risk factors; second week, stroke symptoms; third week, stroke treatments; fourth and fifth weeks, prevention and diet for stroke and related diseases; sixth week, long-term care services and the concept of reablement without actual practice of any IADL tasks).
Outcome Measures
Actual Performance
The FAI was administered by interview to assess the frequency with which the participant carried out the 15 IADL items in three domains (i.e., Domestic, Outdoors, and Leisure and Work). Each domain consists of 5 items. The Domestic domain includes preparing main meals, washing up after meals, washing clothes, light housework, and heavy housework. The Outdoors domain is composed of local shopping, social occasions, walking outside for more than 15 min, actively pursuing a hobby, and driving car or going on bus. The Leisure and Work domain contains travel outings or car rides, gardening, household or car maintenance, reading books, and gainful work. The frequency of performing the 15 item activities is scored on a 4-point scale ranging from 0 (never or none) to 3 (everyday or every week; Holbrook & Skilbeck, 1983). Each domain score ranges from 0 to 15, and the total score ranges from 0 to 45. A higher score indicates more frequent engagement in IADL activities. The FAI’s test–retest reliability has been examined for patients with stroke (Lu et al., 2012).
Ability
The LIADL includes eight IADL items that assess the ability to perform IADL tasks (i.e., using the phone, shopping, preparing food, doing household chores, doing laundry, taking transportation or driving, taking medications, and handling finances; Lawton & Brody, 1969). The total score ranges from 0 to 23, with a higher score demonstrating a better ability to perform IADLs. The LIADL has been applied in the Multi-Aspects Assessment Instrument to assess the level of disability among people receiving long-term care services in Taiwan (Department of Long Term Care Services, 2019). The LIADL has good internal consistency, test–retest reliability, and convergent validity with older adults (Isik et al., 2020; Kadar et al., 2018).
The COPM is a semistructured interview used to understand participants’ self-perceived goals (i.e., IADL tasks); it was used in this study to assess their self-perceived performance and satisfaction with goals. Participants rated two to three IADL tasks on a scale ranging from 1 to 10 to ascertain a score for their performance. A higher score demonstrates greater self-perceived performance on the IADL task. The COPM has sufficient test–retest reliability among patients with stroke (Cup et al., 2003). In this study, we used the COPM Performance score to assess the aspect of ability.
Self-Perceived Difficulty
The PM–3D4D is a 24-item self-report questionnaire used to assess three domains of participation (i.e., Social, Community, and Productivity), rated on four dimensions (i.e., diversity, frequency, desire, and difficulty). We used the difficulty dimension to verify self-perceived difficulty in this study. The Social domain contains 6 items related to communication with others. The Community domain includes 12 items that assess participation in outdoor activities in the community, and the Productivity domain consists of 6 items concerning work, managing house chores, and taking care of others. The summed score for the difficulty dimension of each domain ranges from 0 to 100. A higher score indicates less difficulty in participation. The PM–3D4D has good test–retest reliability, predictive validity, and responsiveness in patients with stroke (Chang, 2017; Chang & Ni, 2019).
Statistical Analysis
We applied χ2 and independent t tests to compare, respectively, the categorical and continuous variables in baseline characteristics between the IADL reablement intervention and health education intervention. The carryover effect of the outcome measures was checked using independent t tests for the two periods. If the t-test results showed no statistical significance, demonstrating negligible carryover effect, we conducted the customary statistical test for investigating group differences. The results of this study showed little to no significant evidence of a carryover effect (ps = .062–.994). The reason could be that the effects were short term without continued therapy. Thus, independent t tests were used to investigate the treatment effects between the two interventions. Change scores for the outcome measures of the two interventions were compared, in spite of the sequences. That is, we merged the data for each intervention in the two sequences to conduct our analyses. A p < .05 indicated a statistically significant difference. The effect size (Cohen’s d) was estimated to verify the size of group differences. The criteria for the effect size were as follows: 0.20 ≤ d < 0.50, small; 0.50 ≤ d < 0.80, moderate; and d ≥ 0.80, large (Chiu et al., 2016).
The sample size for a crossover study was estimated to be at least 23 participants provided a power of 0.80, a significance level of .05, and minimal detectable change of 7.19, which was calculated on the basis of a previous study (Post & de Witte, 2003).
Results
The study enrolled 27 patients with stroke between September 2020 and April 2021. Twenty-two participants completed the two interventions and four assessments for analysis (Figure 1). Table 1 shows the baseline characteristics for the 27 participants. There were no significant differences between the two groups of participants at baseline (ps = .085–.899). In Period 1 of the study, 2 participants (14.3%) in the IADL reablement group and 1 participant (7.7%) in the health education group dropped out. In Period 2 of the study, when groups switched interventions, 2 participants of the remaining 12 (16.7%) dropped out of the IADL reablement group. In this study, participants identified six IADL goals that they wanted to achieve and received IADL training in the reablement program. These goals were as follows: walking outside (36.7%), using transportation (28.6%), housekeeping (12.2%), shopping (10.2%), communication management (10.2%), and meal preparation and cleanup (2.0%).
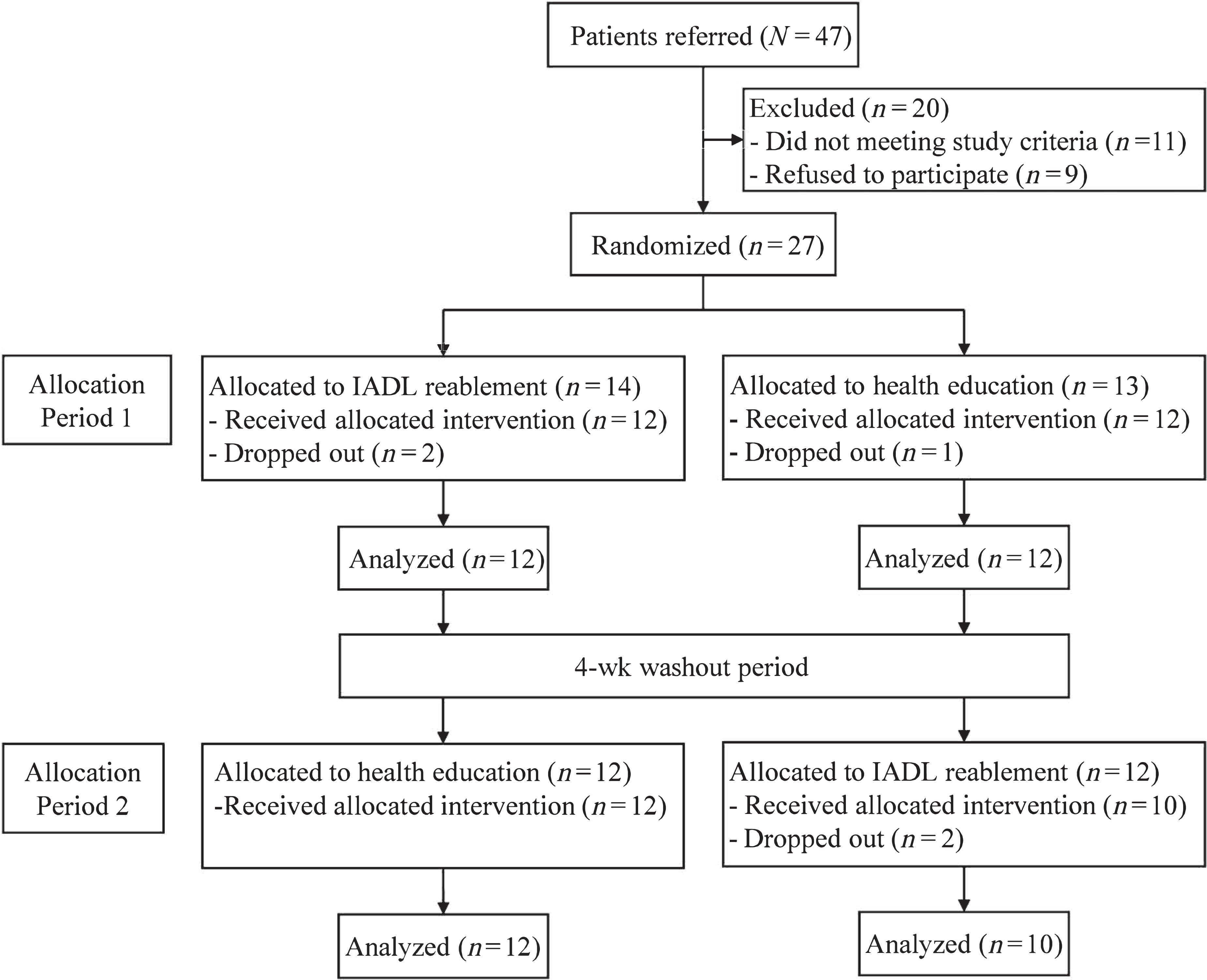
Flow of participants through the study.
Baseline Characteristics of Participants
Note. IADL = instrumental activities of daily living.
The t-test results showed no statistically significant differences in the actual performance outcomes between IADL reablement and health education (ps = .162–.468; Table 2). Small effect sizes (ds = 0.22–0.44) were noticed for the FAI. The participants showed better improvement on the FAI items for IADL reablement than for health education. For the ability outcomes, we found no statistically significant differences between the two interventions (ps = .148–.570; Table 3). IADL reablement resulted in greater progress on the LIADL and the COPM Performance items than health education. Small effect sizes (ds = 0.20–0.45) were found for two IADL items (i.e., doing household chores and taking transportation or driving) and COPM Performance. We found no statistically significant differences between the two interventions for the Community and Productivity domains of the PM–3D4D difficulty dimension (ps = .403–.408; Table 3). Small effect sizes were found for these two domains (d = 0.25).
Pretest and Posttest Outcomes Between the Two Interventions for Actual Performance as Measured With the FAI
Note. p values were derived from change scores. FAI = Frenchay Activities Index.
Pretest and Posttest Outcomes Between the Two Interventions for Ability as Tested With the LIADL, COPM Performance, and Self-Perceived Difficulty as Tested by the PM–3D4D
Note. p values were derived from change scores. COPM = Canadian Occupational Performance Measure; LIADL = Lawton Instrumental Activities of Daily Living Scale; PM–3D4D = Participation Measure–3 Domains, 4 Aspects.
Discussion
In this crossover design study over two periods, we found no statistically significant differences between IADL reablement and health education in aspects of IADL actual performance, ability, and self-perceived difficulty. The statistical significance pertains to the likelihood of the observed effect occurring due to chance. However, the effect sizes showed potential benefits for IADL outcomes for IADL reablement. With a larger sample or more homogeneous participant pool, statistical significance would probably have been achieved. Participants displayed greater improvement in actual performance measured by the FAI and better performance in IADL ability measured by the LIADL and COPM Performance score with the IADL reablement intervention than with the health education intervention.
Reablement supports context-dependent learning for participants. Participants who repeatedly practiced the IADL tasks in their familiar home environment were able to transfer the learned skills to real life. This advantage of reablement may have contributed to enhancement of and application to daily activities (Ingstad et al., 2021). In the aspect of actual performance, participants in this study more frequently performed the IADL tasks, such as washing up after meals, doing housework, and walking outside. Previous studies have also demonstrated that patients were involved and participated in daily activities in the process of reablement (Ingstad et al., 2021; Moe et al., 2017). In this study, participants did not set IADL goals for leisure and work, and their caregivers feared the risk of falling down while performing IADL tasks. Thus, the scores for IADL reablement revealed a trivial effect size for the Leisure and Work domain (d = 0.10) and a small effect size for the Domestic and Outdoor domains (ds = 0.38 and 0.26, respectively) of the FAI.
For the aspect of ability, there are two possible interpretations of the nonsignificant differences between the two interventions. First, approximately half of the participants had moderate to severe disability (modified Rankin Scale score = 4). They could not walk or attend to physical needs without help. Second, carrying out IADLs requires higher cognitive functions than basic ADLs. A previous study of a 6-wk reablement program of basic ADL training showed significant improvements in the aspect of ability for patients with stroke (Han et al., 2020). Therefore, patients with stroke may need intensive training (e.g., 3×/wk) or a longer duration (e.g., 12 wk) to learn and enhance their capability to perform IADLs.
Regarding self-perceived difficulty, small effect sizes were found between the two interventions in the Community and Productivity domains of the PM–3D4D. Participants showed decreased degrees of difficulty in two domains in IADL reablement compared with health education. Patients with stroke who practice IADL skills in the environment they perceive as optimal and safe can increase their confidence in attempting the IADL tasks, especially outdoor and productive activities (Ericsson, 2009). Therefore, participation in IADL tasks at home and in the community could decrease patients’ self-perceived degrees of difficulty.
Two study limitations were noted. First, we recruited participants from two hospitals in northern Taiwan; the heterogeneity of the participants and the small sample size may have limited the generalizability of our results. Second, the suitable frequency and duration of the reablement program has not yet been determined. We adopted a nonintensive schedule (i.e., once a week). Further studies may be conducted with an intensive schedule to investigate the effects of IADL reablement among patients with stroke.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Reablement is appropriate for improving IADLs from the aspects of actual performance, ability, and self-perceived difficulty at home and in the community. ▪ Reablement may be useful for increasing occupational engagement in IADL tasks.
Conclusion
The implementation of this IADL reablement intervention that focused on patients’ personal goal-oriented IADLs revealed positive outcomes. Compared with the health education intervention, the IADL reablement intervention demonstrated the potential to increase the frequency of performing IADLs, improve the ability to carry out IADLs, and decrease the degree of difficulty of carrying out IADLs from the patients’ perspective. Further studies are recommended to investigate the effects of implementing an IADL reablement intervention with a more intensive schedule and longer duration for patients with stroke.
Supplemental Material
Supplementary material for Reablement of Instrumental Activities of Daily Living for Patients With Stroke: A Randomized Crossover Trial
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050288.pdf for Reablement of Instrumental Activities of Daily Living for Patients With Stroke: A Randomized Crossover Trial by Pei-Tsen Chen and En-Chi Chiu in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This study was supported by Cardinal Tien Hospital (Grant No. CTH109AK-NHS-2237). We thank research assistant Fang-Chi Chi for providing the intervention and research assistant Min-Ling Shie for conducting the outcome measures. En-Chi Chiu and Pei-Tsen Chen serve as joint first authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.