
Abstract
Making Meaning is a group intervention that shows promise for improving spiritual well-being for people with multiple sclerosis.
There are currently just under 1 million people diagnosed with multiple sclerosis (MS) in the United States (National Multiple Sclerosis Society, 2019). People with neurodegenerative diseases such as MS report feeling overwhelmed as they navigate an illness that can impair quality of life and achievement of life goals (McGuire et al., 2015). The trajectory of MS can be unpredictable, and an increased risk of depression and the presence of anxiety have been identified as contributors to a decreased quality of life (Andersen et al., 2020; Büssing et al., 2013; McGuire et al., 2015; Sytsma et al., 2020).
Research has consistently linked spiritual well-being to improved coping, mental and physical health, and medical outcomes in people with chronic illness, including MS (Johnson et al., 2011; Munoz et al., 2015; Nsamenang et al., 2016). Spirituality and religion are sometimes viewed as being synonymous; however, there have been calls in the literature to separate them and define spirituality as a search for meaning, peace, and wholeness, separate from religious affiliation (Nichols & Hunt, 2011). Spiritual well-being, an aspect of health-related quality of life, coheres with this approach to spirituality. It can be conceptualized as having two components: (1) the way people experience meaning and purpose in their lives and (2) how they connect to the present moment, to themselves, to nature, and to the sacred (Nsamenang et al., 2016). Evidence supports the idea that health care practitioners should receive pertinent training and address spiritual practices from the client’s perspective (Nichols & Hunt, 2011; Roger & Hatala, 2017 ; Wirth & Büssing, 2016).
Few spiritual interventions for people with MS have been mentioned in the literature. One study indicated that a psychoeducational wellness group addressing the impact of social, intellectual, emotional, and spiritual factors on well-being in participants living with MS resulted in improved depression, anxiety, perceived stress, and pain (McGuire et al., 2015). Experimental studies of spiritual group interventions for patients with MS in Iran demonstrated considerable positive effects on hope and quality of life (Afshar et al., 2021; Ghavi et al., 2021; Hajibabaei et al., 2020; Rahnama et al., 2021). In one study, a spiritual life review intervention for patients with neurodegenerative diseases, including MS, consisted of a transcribed interview with a board-certified chaplain documenting the person’s spiritual path and words of wisdom. Participants improved or maintained their quality of life and spiritual well-being (Sytsma et al., 2020). In a different study, patients with brain cancers and unspecified progressive neurologic conditions created a spiritual legacy document, a record of their spiritual journey preserved for their loved ones and medical team. This intervention was deemed interesting and satisfactory to participants, easily implemented, and practical (Piderman et al., 2015). Occupational therapists have identified an important relationship between involvement in spiritual growth experiences and mental health–related quality of life in women with MS (Tyszka & Farber, 2010). These studies suggest that assisting clients in reframing personal and spiritual growth goals and activities as they navigate the fluctuating abilities and limitations caused by MS is a suitable role for occupational therapists. Although some models address spirituality and its role in occupational therapy practice (Hemphill, 2020; Townsend & Polatajko, 2013), some occupational therapists have identified barriers to using spirituality in client care, including a lack of assessments and insufficient preparedness in academic curricula (Morris et al., 2014 ; Pham et al., 2020).
The Model of Occupational Wholeness (MOW) provides an assessment and intervention framework occupational therapy practitioners can use to address spirituality in client care. It centers on the idea of doing as the medium humans use to fulfill their needs of being, becoming, and belonging (Yazdani & Bonsaken, 2017). The MOW builds on previous models (Hitch et al., 2014a, 2014b; Wilcock, 1999) by considering being, becoming, and belonging in relation to occupational balance and encompassing an assessment and intervention framework that includes the formation of conceptual visual aids (Bonsaken & Yazdani, 2020; Yazdani & Bonsaken, 2017). In the MOW, being is a sense of self-understanding and a need for time and space to connect with oneself. Becoming is an extension of being and includes a sense of hopefulness and growth. Belonging is an extension of being and, at its deepest level, involves a felt connection with things, places, and other people experienced during doing (Bonsaken & Yazdani, 2020; Yazdani & Bonsaken, 2017). The MOW adds to previous research by considering being, becoming, and belonging in relation to occupational balance and including an assessment and intervention framework (Bonsaken & Yazdani, 2020; Yazdani & Bonsaken, 2017).
Although the MOW does not address spirituality explicitly, the notions of being, becoming, and belonging may be viewed as viable expressions of spirituality. One concept analysis of spirituality in persons with chronic illness defined spirituality as consisting of the following components: a journey consisting of hope, growth, and change; connectedness with a divine or supreme being; and connectedness with others (Domocmat, 2014). These concepts can be connected to the MOW notions of becoming, being, and belonging, respectively. According to the MOW’s propositions, one’s need for becoming focuses on the extension of existence beyond the present, the need for being centers on the need for existence, and the need for belonging focuses on the feeling that one’s existence is part of something bigger (Yazdani & Bonsaken, 2017).
In this study, our aim was to determine whether Making Meaning, a weekly group intervention based on the MOW that addresses spiritual well-being, is feasible to use with patients with MS. We include a review of preliminary data on the intervention’s impact on spiritual well-being and identify possible barriers and facilitators.
Method
Design
In this study, we took a mixed-methods approach to program evaluation in accordance with guidelines recommended by Bowen et al. (2009) to determine the feasibility of the Making Meaning spirituality intervention. The team collected participant qualitative and quantitative data simultaneously at pretest and posttest. The group facilitator completed an observation guide after each session. Two student observers completed a parallel guide during the intervention and at each session’s conclusion (Appendix Table A.1). They all entered data online to a secure drive. The University of Kansas Medical Center institutional review board reviewed and approved this study.
Setting and Participants
The Making Meaning group intervention was offered as an elective in the regular programming at a community center providing services for people with MS in a midwestern U.S. city. Initially designed for people with progressive MS, the program is now open to individuals age ≥18 yr diagnosed with any type of MS who report physical or cognitive disability that limits work or daily activities. The community center’s mission is “to enhance the quality of life for people with progressed MS” (https://www.msachievementcenter.org/program). The MS Quality of Life Index (Consortium of Multiple Sclerosis Centers Health Services Research Subcommittee, 1997) is used at intake. Members come 1 day/wk and participate in small groups facilitated by therapists, a social worker, and health profession students. Groups include exercise, occupational therapy, connections, brain balance, and electives. Attendance records for 42 participants who took part in at least one session were available for analysis. Twenty-two participants provided qualitative data for analysis, and 10 individuals had pretest and posttest scores and attended at least half the sessions, meeting the inclusion criteria for the quantitative outcome measure analysis.
Intervention
The Making Meaning group intervention uses psychoeducational and activity components to address spiritual well-being. It uses the MOW to provide a framework for exploring spiritual practices and how members can incorporate them into daily routines and activities to improve spiritual well-being and coping with chronic illness. Each session includes an opening/centering ritual, a brief check-in with members, an introduction to the creative activity and theme for the session, and discussion questions. During the activity, discussion allows members to explore deeper insights and share how the activity may relate to their spiritual practice (Table 1). Finally, a closing component enables members to share their intentions for continuing or engaging in new spiritual practices in the coming week.
Overview of Making Meaning Sessions
Note. MOW = Model of Occupational Wholeness.
The intervention was offered in eight weekly sessions, each lasting 45 min. Center members attend 1 of 3 days/wk programming is available; therefore, the same group facilitator provided the Making Meaning intervention 3×/wk to three different groups of participants in a midafternoon elective programming slot. Because of various circumstances, including a global health pandemic and inclement weather, an alternate elective was not provided, resulting in all center members who were present participating in the Making Meaning group intervention. The program was designed as an in-person experience. Modifications for virtual delivery were developed in advance of implementation, given the likelihood of center closures because of inclement weather and public health concerns. A doctoral-level occupational therapy student, who collaborated in the development of exemplar activities, served as the group facilitator as part of her capstone experience. Two second-year doctoral-level occupational therapy students served as observers and provided physical assistance as necessary. During implementation, the facilitator received weekly on-site mentorship from the program’s occupational therapist, who has expertise in MS care, and a short debrief after each session with the program’s social worker (3×/wk). The group facilitator also collaborated with Melissa Ross Bowen, who is an occupational therapist and an ordained clergyperson, at the conclusion of each week. Before the program’s onset, the team gathered local resources for direct spiritual care should referral for more intensive spiritual care be necessary.
Data Sources
Quantitative data included participant pre- and posttest scores on the Functional Assessment of Chronic Illness Therapy–Spiritual Well-Being 12-Item Scale (FACIT–Sp–12; FACIT Group, 2021) and attendance records. The FACIT–Sp–12 is a 12-item scaled outcome measure that examines faith, a sense of purpose, and meaning in life. It has been used in previous studies of spiritual intervention for people with MS (Johnson et al., 2011; Nsamenang et al., 2016 ; Sytsma et al., 2020). Qualitative data included participants’ written or typed responses to open-ended questions and the notes and reflections of the group facilitator and two student observers. We were concerned about the vulnerability and fatigue level of our participants and accepted their abbreviated responses to qualitative questions despite the fact that they resulted in an insufficient scope and depth of data and thus qualitative analyses of limited efficacy.
Data Analyses
We analyzed the qualitative data using theoretical thematic analysis (Percy et al., 2015). Bowen completed open coding of all qualitative data units from the facilitator, 2 student observers, and 10 participants who met the inclusion criteria. Although this type of data analysis is driven by feasibility themes, and analytic preconceptions are acknowledged, we made a concerted effort to keep any theme-based language out of the codes at this stage of analysis and used codes that mirrored the participants’ language. Open codes were entered into a table on the basis of the interview guide questions. A second review of the transcript was conducted to ensure all data units were coded. Open codes were then sorted into categories on the basis of similarities in content patterns. We made an effort at this point to remain open to any emerging themes or structures that would be representative of the data. Finally, patterns that corresponded to preexisting themes were grouped with other patterns relating to that theme. The six theoretical themes used for this analysis were (1) acceptability, (2) demand, (3) implementation, (4) practicality, (5) adaptation, and (6) limited efficacy. Proposed foci of feasibility studies served as the source for these theoretical themes (Bowen et al., 2009). An overview of feasibility themes and data sources is provided in Figure 1.
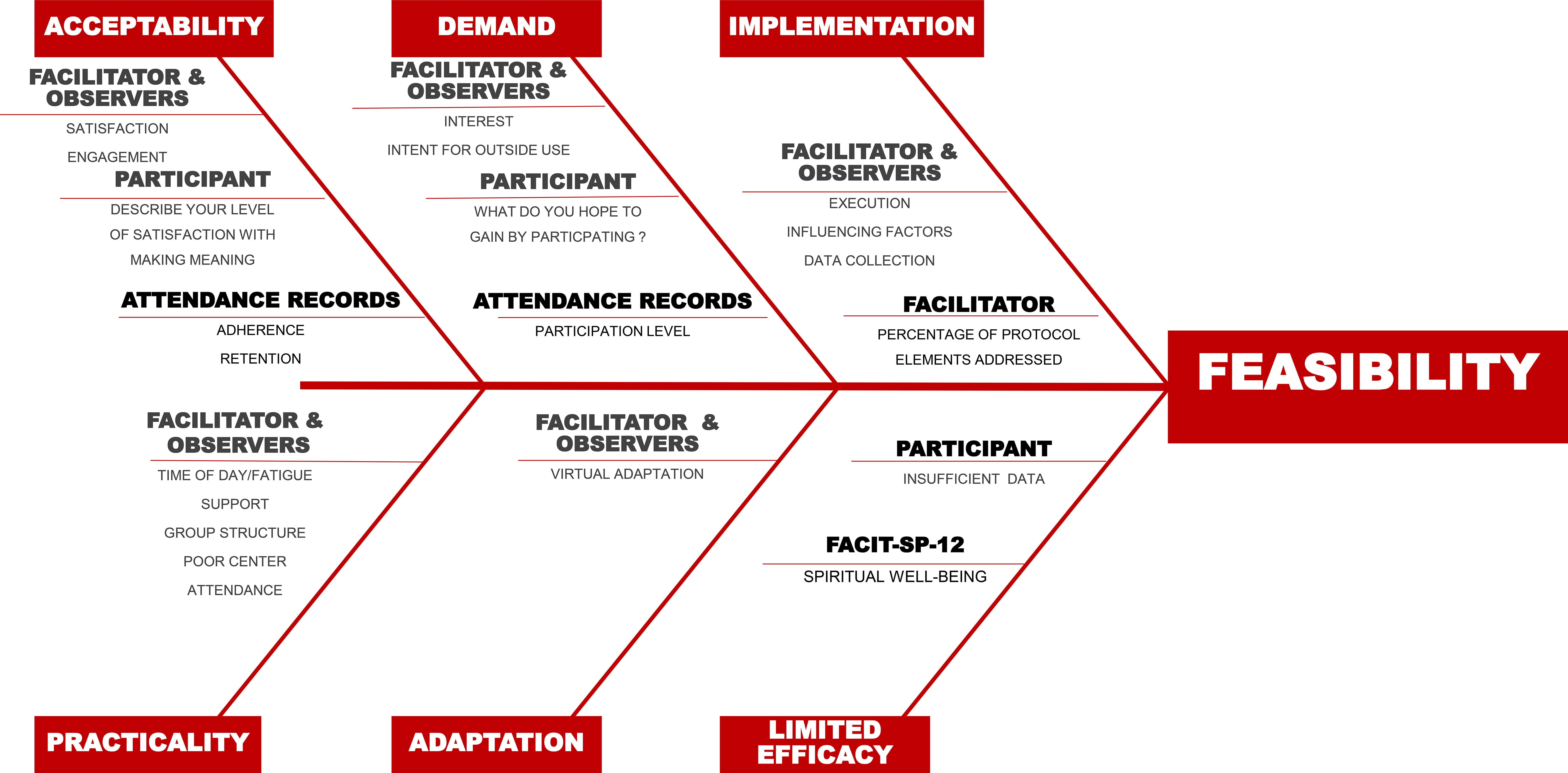
Feasibility themes and data sources.
Using descriptive statistics, we summarized attendance data from all participants (n = 42). The quantitative analysis included data from 10 participants who attended 4 or more sessions (50%). We calculated Cohen’s d effect sizes to examine the preliminary efficacy of the intervention based on the mean difference between pretest and posttest FACIT–Sp–12 scores.
Results
Forty-two participants attended at least one Making Meaning session. This group included 30 women and 12 men, with an average age of 63.9 yr. Average time since diagnosis was 25.4 yr. Sixty-three percent lived in a cohabitation setting. The highest education levels achieved were as follows: 32% high school, 44% undergraduate degree, and 24% advanced degree. Twenty-two participants provided qualitative data, and 10 completed more than half the interventions and provided pretest and posttest data. The results summarize the qualitative findings from 22 participants who provided qualitative data; quantitative results are limited to the 10 participants who attended at least half the sessions. Selected qualitative data, organized by patterns and themes, are provided in Table 2.
Feasibility Outcomes With Supporting Qualitative Data
Note. The data for Feasibility Theme 6: Limited Efficacy were quantitative only and are not included in this table. The scope and depth of qualitative data related to this theme were insufficient for analysis related to efficacy.
Feasibility Theme 1: Acceptability
Acceptability is a measure of how participants react to an intervention (Bowen et al., 2009). Qualitative data emerged in the form of two patterns that elucidate this aspect of feasibility: (1) satisfaction and (2) engagement. Quantitative acceptability measures included adherence and retention, including the attendance rate of participants who attended at least one group.
Satisfaction
Observations or expressions of gratitude for and enjoyment of the program were present in nearly all sessions. Participants called sessions “great” and “wonderful” and stated, “I love this.” They noted activities they thought were good ideas and expressed satisfaction with the variety of practices explored. There were occasional observations of dissatisfaction, most notably in Session 8, when some participants found the amount of program evaluation data collected overwhelming. Observations of satisfaction often increased when the group was involved in creating something they could take home, such as a gift for others. Observers also noted a particularly marked increase in direct expressions of satisfaction during a session focused on providing affirmations for peers.
Eighty-one percent of the 22 participants rated their satisfaction as positive. Participants expressed satisfaction with the spiritual, nonreligious nature of the group (“very satisfied—good project—glad it wasn’t just about religion”) and satisfaction despite poor attendance: “Although I was only able to attend 2 sessions, I enjoyed both and felt the subject matter was extremely valuable.” Four participants indicated lower levels of satisfaction. These included ratings of “2 out of 5,” “2.5 out of 5,” “fair,” and a statement that the group did not spend enough time on reflection and sometimes felt rushed. Higher ratings indicate greater participant satisfaction.
Engagement
Observations of engagement included group participants encouraging, supporting, and helping each other. They generally collaborated to generate ideas, and when a session required more individualized work the absence of collaboration was notable to observers. Group participants engaged in meaningful discussion and shared their creations or responses in most sessions. An observer noted that participants “seemed comfortable to share what’s on their minds.” The facilitator and observers described engagement in all eight sessions using terms like “joy,” “introspective and intimate sharing,” “gratification,” and “hopefulness.” Observers noted one exception to engagement on a day when group attendance was higher than usual and participants were completing program evaluation data collection.
The group facilitator and observers felt that facilitators of engagement included a balance of active and reflective activities, novel or fun activities, hands-on activities, and movement. Making Meaning sessions occurred at the end of a full day of programming; beginning the group with movement was uniformly considered a strength and its absence a weakness. The observers and facilitator viewed creative activities as a means of increasing a sense of control, ownership, and self-expression. However, there was variability in group and individual responses to creative activities.
Adherence and Retention
Adherence was a measure of attendance by participants who were already present at the center on a given day. Did they come to, or stay online for, the Making Meaning intervention? Participants were defined as members who had attended one or more Making Meaning sessions. The adherence rate was 88%. Further examination revealed that attendance at in-person sessions was 96% and for virtual sessions was 73%. More information can be found in Table 3.
Making Meaning Adherence Data: Participation for Persons Who Attended at Least One Making Meaning Session
Note. N = 42.
The retention rate for participants was 86%. Dropouts (n = 6) were defined as participants who attended at least one session and did not return for another throughout the program despite their presence at the center. Those who dropped out of the Making Meaning intervention also had low center attendance (47%) during the time the intervention took place.
Feasibility Theme 2: Demand
Demand, as a measure of feasibility, addresses the use of the intervention by the intended population (Bowen et al., 2009). Qualitative patterns illuminating the use of this intervention included interest level in and hopes for the group , and reference to the actual or intended use of the intervention content or material outside of the group. Participation level, calculated as a percentage of those present at the center who chose to attend the group, was a quantitative measure of demand.
Interest Level
The facilitator and observers noted participant curiosity, excitement, or eagerness at least 1 day of each session. The interest level in activities did vary among participants. Some appeared wary of activities such as the finger labyrinth or breathing exercises, whereas others demonstrated definite interest in them. Observers noted that participants were often interested in sharing with the group and listening to each other. The only observation of participants having difficulty sustaining interest in attending was during a virtual session.
Participants expressed interest in connecting, hearing from and supporting each other, and learning more about spirituality and its importance for well- being at the outset of the group. Several participants revealed hopes for discussing and discerning purpose and supporting each other in the experience of “life [with] MS.”
Intention to Use the Intervention Outside the Group
Participants occasionally referenced previous practices, intent to use the intervention outside the group or share it with others, and how the intervention applied to navigating life with MS. In one session, they made goals to be undertaken outside the group, and they expressed pleasure with take-home activities.
Participation Level
The participation level was the percentage rate of participants attending the group based on overall center attendance. Overall participation was 80%, in-person participation was 94%, and virtual participation was 59%. Beginning in Week 3, Making Meaning was the only elective because of shortened programming related to the coronavirus disease 2019 (COVID-19) pandemic, limiting the ability to draw conclusions on demand for the intervention. Details on participation levels are provided in Table 3.
Feasibility Theme 3: Implementation
Implementation is the extent of success in delivering an intervention as planned and proposed (Bowen et al., 2009). Patterns of qualitative data that define this measure of feasibility include execution strengths and weaknesses, factors influencing implementation ease or difficulty, data collection, and percentage of protocol elements addressed. Bowen compared facilitator notes with the group protocol to generate a percentage of protocol elements that were addressed and a description of any substantive additions or deletions.
Execution Strengths and Weaknesses
Qualitative data revealed intervention strengths, including providing examples, visual support for directions, concise and clear directions, prompts to decrease the need for written output, clear and explicit explanation of session purpose and connection to the MOW, and options for using assistive technology. Weaknesses included time management concerns (most frequently involving varying completion rates and wait times) and occasional groups when examples, visual supports, or explanation of activity purpose were inadequate or rushed.
Factors Influencing Implementation Ease
Observer notes revealed traits of the group facilitator that created ease of implementation, including emotional intelligence, active listening, group leadership, and transparency. The facilitator and observers noted other factors that influenced intervention implementation, including the availability of supplies, distractions resulting from people entering and leaving the room, and providing appropriate background music.
Data Collection
The group facilitator and student observers agreed that program evaluation data collection, in particular the number of short-answer questions, was burdensome, and participants needed a more substantial explanation of their purpose. The team completed all pretest data collections, and one of three posttest data collections, virtually. Observers noted that in-person data collection improved with both paper and electronic options and staff supporting completion. On the basis of their observations, they made suggestions for improvement, including combining two forms into one for the virtual option and making clear the expectation that data collection will occur during the session.
Percentage of Protocol Elements Addressed
To ensure the fidelity of the Making Meaning intervention, the group facilitator (1) kept field notes of the elements and activities addressed in each session and (2) checked activities against the group protocol. Data revealed that the facilitator made no substantive deletions or additions in 19 of 23 sessions (83%). The facilitator made deletions and additions in response to time management rather than content-related concerns.
Feasibility Theme 4: Practicality
Practicality is the ability of the current context of the intervention to support the delivery of the intervention program (Bowen et al., 2009). Patterns of qualitative data consistent with this measure of feasibility included the time of day providers offered the group, the presence of support staff, group structure, and poor center attendance.
Time of Day
The Making Meaning group intervention was offered as an elective from 2:15 to 3:00 p.m. during the regular schedule at the end of a day of programming that included a series of 45-min groups. The groups included physical rehabilitation, psychological support, social activities, and health education. Fatigue was observed in virtual and in-person sessions but more frequently during the latter. Observers noted the most pronounced fatigue when participants returned for their first full-day sessions after attending virtually because of the COVID-19 pandemic. They described participants’ willingness to persist through marked fatigue and remain engaged in group activities and noted that movement breaks helped combat fatigue.
Support Staff
The facilitator and observers generally viewed staff and student support in providing physical assistance or clarification of directions as a strength when present and a weakness when absent. Support included acting as a scribe for writing and creative activities, providing individualized clarification, and facilitating physical transitions. The presence of support persons was problematic in one instance when they outnumbered the participants present.
Group Structure
A decision to eliminate an alternate elective at the time of Session 3 facilitated attendance and encouraged members to try the group; however, it also resulted in new group participants entering the group in its last sessions as center attendance began to increase. During the wrap-up session, the facilitator and observers noted confusion in participants who had joined the group in the last two sessions and had not completed the initial MOW assessments.
Poor Center Attendance
Attendance rates for the group intervention, when considered as a percentage of all members, present at the center or not, were much lower for both virtual (30%) and in-person (50%) groups. Documentation of the reasons for center absence was inconsistent, but the most common reasons were illness or transportation issues. Center attendance did begin to improve in the last 2 wk of the intervention. Group attendance ranged from 3 to 8 persons until Sessions 7 and 8, when it increased to 11 participants for two groups.
Feasibility Theme 5: Adaptation
Adaptation considers how the intervention performs with changes to accommodate a new format or population (Bowen et al., 2009). This intervention was initially designed to be conducted in person, with virtual options provided as backup. Because of both the public health emergency created by the pandemic and weather closures, providers delivered 9 of 23 groups virtually.
The ability to adapt to virtual delivery allowed the intervention to occur as scheduled and created a space for participants to connect in a time of isolation. One observer noted the following: Being online and lacking some opportunities for social interaction has impacted a lot of the members, so giving them a chance to reflect on what they’re grateful for and what brings them joy was a good way to create some happiness. Everyone just seemed to be in a positive and good mood as a whole.
No direct participant data addressed virtual adaptation. The group facilitator and observers noted how some in-person activities translated well to the virtual format. Supports for virtual adaptation included increased visual information, step-by-step explanations, and multiple modes of access to materials in familiar formats (email, text, and Facebook). Barriers to virtual adaptation included multiple documents, unfamiliar virtual platforms, difficulty converting the MOW assessment framework for virtual administration, and a lack of hands-on activities. Group participants initiated adaptations as well. One group took the prompt for an in-person creative art activity “What words of wisdom would you like to pass on?” and not only shared the answer to the question in the virtual session but also expanded it. They initiated a discussion of practices associated with their “word of wisdom,” resulting in an engaging online group, despite the lack of hands-on activity.
Feasibility Theme 6: Limited Efficacy
Bowen et al. (2009) suggested that feasibility studies examine limited efficacy to learn whether “a new idea, program, process, or measure show promise of being successful with the intended population” (p. P453). In the present study, we explored the intended effects of the Making Meaning program on key intermediate variables measured by the FACIT–Sp–12. Ten participants attended at least 50% of the sessions and provided full pre- or posttest data. The total FACIT–Sp–12 averages for these participants were 33.5 (SD = 9.0) at pretest (Session 1) and 36.6 (SD = 5.4) at posttest (Session 8). Cohen’s d effect size based on the mean differences from pretest to posttest was moderate (d = 0.42). Mean differences varied by day of delivery, but the low sample size prevented us from exploring group differences. The scope and depth of the qualitative participant data we obtained were insufficient for analyses related to efficacy.
Discussion
Making Meaning, an 8-wk group intervention based on the MOW that focuses on spiritual well-being, is a feasible means of addressing spiritual well-being for people with progressed MS. Our evaluation of the program fills a critical gap in the limited literature addressing spiritual interventions with this population. The moderate effect size for improved spiritual well-being from pretest to posttest suggests that this group intervention holds promise as a means of addressing spirituality for people with MS. Previous research has linked spiritual well-being with a variety of favorable health outcomes (Johnson et al., 2011; Nsamenang et al., 2016; Roger & Hatala, 2017), making this finding a compelling reason to move forward with further study of this group intervention.
Our evaluation of the program revealed essential considerations in providing a group intervention for people with progressed MS. Participant fatigue, inconsistent center attendance, and the perceived burden of research participation proved particularly important in implementing a group intervention with this population. Fatigue has been identified as a factor underlying poor quality of life in people with MS (McGuire et al., 2015). Although the center-based context of this intervention consolidated the need for multiple appointments and travel, it also entailed sequential programs, and end-of-the-day fatigue was noted. Although the time of day and presence of fatigue were problematic, they were not insurmountable, and the facilitator used strategies, including stretching and brief movement breaks, to manage their effect. Further research addressing fatigue in the group structure would be beneficial.
Transportation issues and illness were the most frequently cited reasons for inconsistent center attendance. The intervention occurred during a pandemic health crisis and late winter, necessitating transitions to the virtual environment. Altering the group’s timing for improved attendance could be important for future assessments of demand and interest.
Despite attempts to keep data collection for this population as abbreviated as possible, logistics necessitated program evaluation data collection in the form of the written output of short-answer questions that the facilitator and observers felt were burdensome to participants. An established intervention without program evaluation will entail markedly less data collection. Using participant focus groups in future research could maximize responses while respecting energy levels. Previous research has found that the burden of research participation may be stressful for some people (Lawson et al., 2022). It is possible that the perceived burden of providing program evaluation data affected the study’s outcomes.
This program evaluation also identified important group structure and format factors. The sample size was too small to draw firm conclusions regarding the impact of group size; the qualitative data suggest that a group size of 4 to 8 participants results in good engagement and ease of implementation. Qualitative data indicated the need for an extension of the time frame for each group. Forty-five minutes was not sufficient to consistently allow for relaxed participation and inclusion of movement in each session. One group intervention for wellness with this population reported good outcomes with a group structure of 90-min sessions for 10 wk (McGuire et al., 2015). The next step with this intervention might be expanding the time to 75-min sessions while incorporating strategies to manage fatigue.
Qualitative results indicated that the Making Meaning intervention met participants’ expectations for providing opportunities for peer connection and support. Participants were often engaged and expressed gratitude despite fatigue or frustration with the online environment. The qualitative data indicated the importance of spirituality in participants’ lives and their willingness to share with and support each other. This desire for and readiness to participate in a spiritual intervention support the ongoing need to create a space and opportunity for addressing spirituality with this population. Previous research has called for creativity in providing spiritual interventions for persons with neurodegenerative disease (Sytsma et al., 2020). The spiritual well-being outcomes of the FACIT–Sp–12 in this program evaluation were consistent with those achieved by an individual life review intervention led by chaplains (Sytsma et al., 2020). Occupational therapy practitioners have identified spirituality as a client factor within their domain of practice and have a strong history and tradition of addressing the individual holistically, making them well suited to provide spiritual care (American Occupational Therapy Association, 2020; Pham et al., 2020). The use of the MOW in this group intervention provides a promising framework for guiding practice in the area of spiritual care.
Strengths and Limitations
The main strength of our program evaluation is its focus on the quality and value of the intervention in the naturalistic environment without controls, allowing claims to be made about the program’s merit (Adams & Neville, 2020). Limitations of this program evaluation include the lack of an administrative perspective on the feasibility of the intervention, an inability to member-check qualitative data because of the retrospective nature of the evaluation, potentially burdensome data collection measures, and a limited sample size.
Future research could include a prospective mixed-methods design with multiple sites, using focus groups to increase the breadth and depth of participant feedback, expansion of data sources to include administrators, a closed group structure, and consideration of timing to support attendance. Another possibility for future study is an exploration of whether and how the length of the sessions affects participant satisfaction and outcomes.
Implications for Occupational Therapy Practice
We developed the Making Meaning group intervention for spiritual well-being, on the basis of the MOW, to meet a need for group-based spiritual interventions among people with progressed MS. The present study has the following implications for occupational therapy practice: ▪ Occupational therapy practitioners have a unique perspective on and opportunity to improve spiritual well-being in persons with MS by using the MOW as a framework to address spiritual occupations. ▪ There is an opportunity to build on this intervention in occupational therapy clinical research. The intervention has been shown to be feasible, and further study using prospective designs to determine efficacy is warranted. ▪ There is also a need to educate occupational therapy practitioners about increasing students’ working knowledge of spirituality and health to facilitate improved clinical reasoning for occupational therapy’s role in addressing clients’ spiritual well-being.
Conclusion
This program evaluation demonstrates the feasibility of the Making Meaning group spiritual intervention in a community-based setting. Most participants were satisfied with the intervention, and adaptations necessitated by environmental demands were successfully incorporated. The evaluators gained valuable information from this program evaluation to refine the Making Meaning protocol. This intervention holds promise for meeting the need for spiritual care for persons with MS, and future studies should include prospective designs to assess its efficacy.
Footnotes
Group Facilitator and Student Observer Observation Guide
| Group Facilitator | Student Observers |
|---|---|
| Were elements of protocol addressed? | What were the discussion questions addressed? |
| Were substantive additions necessary? What? Results? | |
| What were the strengths of the session? | |
| What were the weaknesses of the session? | |
| What portion of the intervention went well? Why? | |
| What portion of the intervention could have been improved? How? | |
| What is your perception of how group members received the session? | |
| Was there any portion of the protocol that was especially helpful? | Quotes/observations |
| Was there any portion of the protocol that was a hindrance to the session? | |