
Abstract
This study identifies what helps and hinders pediatric occupational therapists in addressing the sleep health concerns of their clients as well as actionable steps that can be developed to promote the role of occupational therapy in supporting sleep.
A child’s sleep health critically affects academic learning, mental health, immune health, and physical growth (Chaput et al., 2016; Chien et al., 2019; Spruyt, 2019). Considerable sleep problems have been reported in 40% to 80% of neurodiverse children (Blackmer & Feinstein, 2016; Cortesi et al., 2010; Langberg et al., 2020; Romeo et al., 2021), a rate that is at least twice as high as the general population’s prevalence of 20% to 30% (Maski & Owens, 2016; Owens, 2008). Considering that neurodiverse children often seek occupational therapy services, sleep assessment and intervention should be common in occupational therapy treatment.
Promoting good sleep health is considered foun dational in health care therapies that promote development, such as occupational therapy (American Occupational Therapy Association [AOTA], 2020). However, despite the inclusion of sleep in many rehabilitation providers’ frameworks, sleep has historically been overlooked in typical rehabilitation care (Fung et al., 2013; Valenza et al., 2011; Verschuren et al., 2017). In recent years, occupational therapy clinicians and scientists have highlighted the need for occupational therapists to address sleep concerns within routine care (Fan & Drumheller, 2021; Faulkner, 2022; Ho & Siu, 2018; Iwama et al., 2015; Tester & Foss, 2018). In recent surveys, researchers have noted that occupational therapists frequently do not evaluate or address sleep in routine therapy, yet they report a desire to be better prepared to evaluate and treat sleep in their practice (Ludwig et al., 2022; Piller et al., 2021). In this study, we built on these findings by using qualitative methods to identify why sleep continues to be overlooked. The long-term goal is to create clear, actionable steps to improve service delivery to occupational therapy clients.
The purpose of this qualitative descriptive study was to thoroughly examine (1) pediatric occupational therapists’ experiences addressing sleep health during typical care, (2) the role sleep plays in rehabilitation goals, (3) pediatric occupational therapists’ confidence in addressing sleep concerns, and (4) the supports and barriers they encounter related to addressing sleep health concerns for their pediatric clients. Our research question was “What are the experiences and perspectives of pediatric occupational therapists in the United States with regard to addressing sleep concerns within therapy?”
Method
We used a qualitative descriptive methodology (Sandelowski, 2000) with a constructivist paradigm to explore pediatric occupational therapists’ perspectives on sleep health in their practice. A constructivist paradigm allows for each individual perspective to be seen as one construct of reality, thereby allowing each participant to contribute to an overall understanding in a unique way (Hatch, 2002). This paradigm also allows for the researcher and study participants to work as cobuilders of the construction of the findings. This concept aligns well with this study because we are pediatric occupational therapists with our own experiences. We chose this methodology and paradigm so we could develop a rich description of occupational therapists’ perceptions of sleep health that allows for personal experiences to inform the end model or framework. All procedures, consent forms, and measures were approved by the University of Pittsburgh’s institutional review board (STUDY20090057).
Researcher Characteristics and Reflexivity
The three researchers who were involved directly in data collection and interpretation are female pediatric occupational therapists: Amy G. Hartman, Roxanna Bendixen, and Kaitlyn Caspero. Hartman, the study’s principal investigator, conducted all interviews and has 10 yr of clinical experience in inpatient and outpatient pediatric occupational therapy. She received qualitative training through her doctoral education and was mentored in the qualitative process by Bendixen. Bendixen has been a pediatric occupational therapy researcher for 16 yr and a clinical occupational therapist for 5 yr. Caspero assisted with coding and data analysis and is a pediatric occupational therapist with 7 yr of clinical experience, primarily in outpatient occupational therapy settings. She also has experience in assisting with qualitative coding and interviewing.
In the development of this project, Hartman assumed that sleep was underaddressed because of her own experiences as a clinician and prior research in the area. She did not want to bias the direction of the study; therefore, she ensured that the beginning questions in the interview guide offered opportunities for participants to share times when they had discussed sleep and their views on the importance of sleep for their clients. She also kept a reflection journal during data collection and analysis to identify times when personal bias or interest might be influencing the direction of the study.
Participants
Currently practicing pediatric occupational therapists across the United States were invited to participate. Before the start of this study, a target sample size was set for 20 participants with the flexibility to continue sampling if thematic saturation had not been met. Using a convenience sampling method, we recruited therapists using emails to clinics and individuals across the United States. Email addresses were obtained through internet searches and the authors’ professional networks. Four of the participants were former colleagues of Hartman. To increase the variety of experiences, recruitment was capped at 5 participants from the same metroplex and 1 person from a clinic. Therapists who indicated interest in the study were contacted by Hartman via telephone to enroll in the study.
Data Collection
During the months of January and February 2021, Hartman conducted hour-long semistructured interviews with participants using Zoom videoconferencing software. Interviews were recorded, except for instances when technology faltered (n = 3); in those cases, interviews were completed over the phone. To build rapport and develop a relationship before the interview, Hartman shared with each participant the aim of the study and the fact that she was also a pediatric occupational therapist. Participants completed the interview in a setting and at a time that was convenient to them. All but 1 participant was alone in their setting, with 1 participant caring for their own child toward the end of the interview. Throughout the interview, Hartman facilitated the discussion using a semistructured interview guide with questions of interest to focus the conversation on the aims of this study (see the Appendix).
The semistructured interview guide was developed by Hartman and pilot tested with Caspero before initiating the study. This guide was used to provide some initial structure for the interview and was based on the study’s aims. During the interview, participants were free to share additional information, and Hartman used probing questions to explore topics in more detail.
Hartman took notes on the discussions and wrote down any thoughts or personal bias that became apparent. For the first 8 to 10 interviews, she wrote an overall impression and general themes at the end of the interview in a reflection journal to clarify broad themes and ensure the interview guide questions were still appropriate.
Upon completion of the interview, participants completed an online demographics questionnaire using REDCap software (Clinical and Translational Sciences Institute at the University of Pittsburgh Grant UL1-TR-001857). This questionnaire included questions about basic demographic characteristics; their experience level as a clinician; current practice setting and location; and the age, race, and ethnicity of the children they serve.
Data Analysis
The transcripts of the interviews, interview notes, reflection journal, and demographic questionnaires were all used during data analysis. Interviews were transcribed using Zoom software (Otter.ai) and then cleaned by Hartman using the audio recording of the interview. Interview transcripts were transferred to Microsoft Excel documents for analysis. We took a qualitative thematic analysis approach to analyze the data (Braun & Clarke, 2006). This analysis method was chosen to provide a rich and detailed account of the perspectives of the participants without imposing a priori frameworks or hypotheses onto the data.
Two researchers (Hartman and Caspero) read each interview, applied structural codes to identify sections of text that surrounded each question of the interview, and added any additional concepts that were discussed. In the second round of coding, descriptive and in vivo coding methods were used to summarize emerging themes within each structural code. The researchers met twice monthly to review themes and ensure agreement. Concepts that were difficult or required more thorough discussion were brought to larger laboratory meetings with Bendixen.
As interviews were coded, we moved the codes into a large descriptive matrix within Microsoft Excel with each structural code as its own tab, preliminary categories across the x-axis at the top and each participant placed along the y-axis. Descriptive codes and in vivo text were placed into the individual cells. Matrix analysis (Averill, 2002) allows for data to be presented in such a way that overarching themes can be discovered and interactions can be explored. As new categories were discovered, already-coded interviews were reviewed to ensure any new category was not missed. To explore unique themes by specific setting, we grouped participants by the primary setting in which they worked. Unique themes that were setting specific were identified.
All participants were sent an overview of major themes that emerged from the data as a member-checking opportunity. Participants were asked to confirm that their thoughts had been accurately captured within these themes. Sixteen of the 20 participants responded to this member checking, and all reported that their experience had been appropriately captured.
Results
Twenty-four pediatric occupational therapists indicated interest in this study, and 20 completed interviews. Participants’ demographic information can be found in Table 1. Four interested individuals were unable to be contacted after their original email of interest and therefore never provided consent and did not participate. No data were collected on them to understand whether their nonparticipation was correlated with a particular characteristic. After 18 interviews were conducted, data saturation was becoming evident. To ensure data saturation was met, two more interviews with targeted participants (known to Hartman) with unique experiences were conducted. One interview was with a female travel occupational therapist who served Alaskan Native children, and the other was with a male occupational therapist with 19 yr of experience as a clinician and a current position with administrative as well as clinical responsibilities in a hospital system.
Therapist Demographic Characteristics
After overarching themes were developed, we then separated interviews according to the therapist’s primary setting(s) and explored unique setting-specific themes. Primary settings included outpatient (n = 14), early intervention (n = 6), school systems (n = 4), and inpatient hospital (n = 2). Within this analysis, setting-specific supports and barriers became apparent, along with novel themes about how sleep is viewed.
Therapists voiced interest in discussing the role of sleep in routine care for their clients. They used words such as important, complex, individualized, and fluid to characterize sleep in a therapeutic setting. They talked about how sleep affects a person’s occupations and overall development, using phrases such as “biggest life skill” and “kids look really different once they’re sleeping” (Participant 118). Therapists also viewed sleep as a concept that is intricately woven throughout each member of the family unit and therefore an intimate part of the lives of the children with whom they worked.
Despite its importance, more than half of the therapists interviewed report that, before this study, they did not regularly inquire about a child’s sleep health as part of their practice. A variety of themes describing the supports and barriers to addressing sleep emerged. These themes fell into four broad categories: (1) personal factors, (2) client/family factors, (3) setting-specific factors, and (4) external factors (Table 2, Figure 1).
Factors That Affect Pediatric Occupational Therapists When Addressing Sleep
Note. Numbers in parentheses are participant identifiers. OT = occupational therapist/therapy.
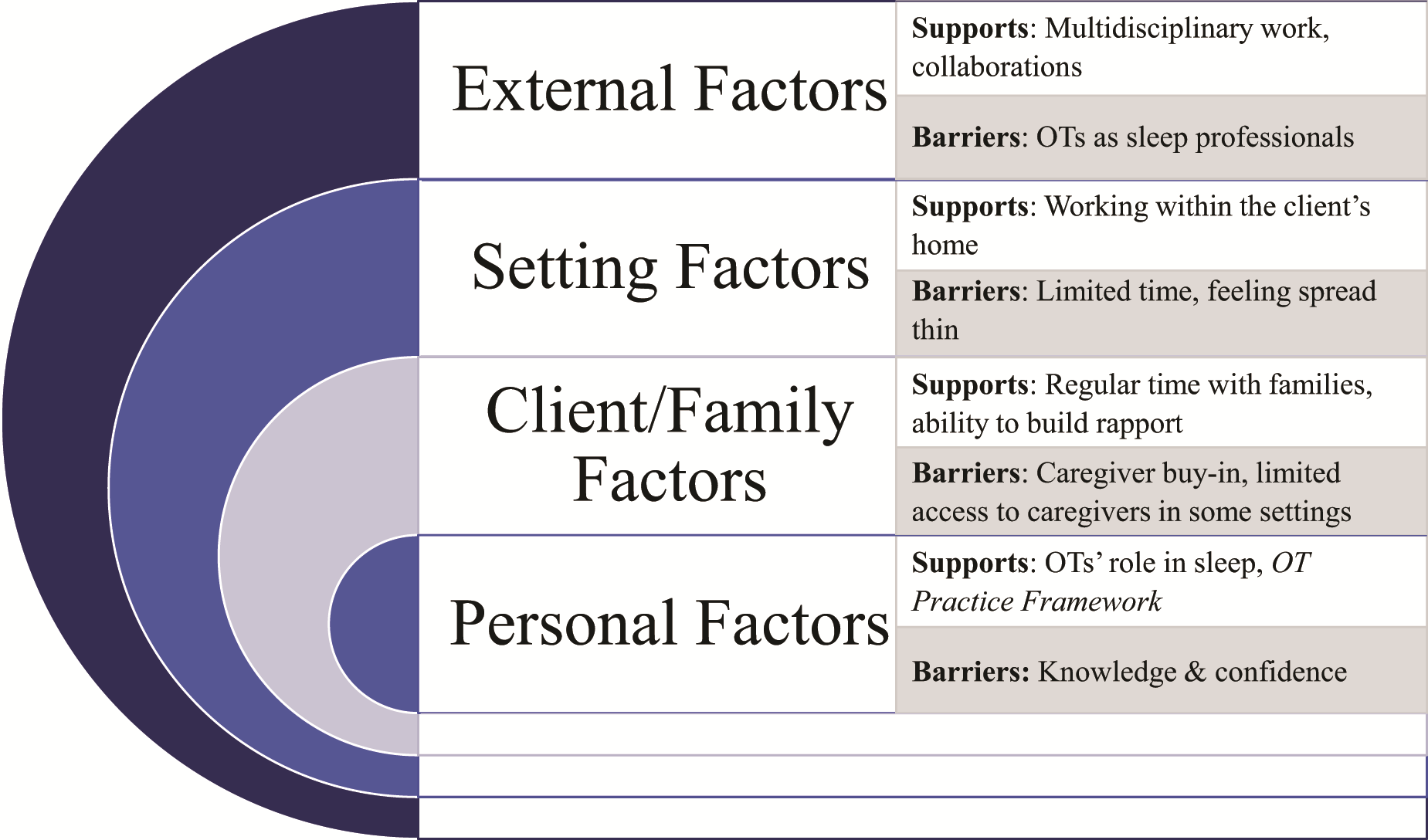
Major themes of qualitative interviews.
Personal Factors
“I do feel like as [occupational therapists] we are a good profession to take kind of a primary role in addressing sleep and asking about it” (117). (Numbers in parentheses are participant identifiers.) Overall, occupational therapists believed they have a distinct role in addressing sleep concerns in the pediatric setting, mentioning that rest and sleep are critical occupations identified in the Occupational Therapy Practice Framework (4th ed.; OTPF–4; AOTA, 2020). They identified specific foundational skills that support their involvement in addressing sleep concerns in the clinic, such as knowledge of environmental adaptations, routines, clinical interviews, and sensory tools to support sensory processing. Therapists who had past experiences addressing sleep shared that they had focused on environmental adaptations (e.g., opening window blinds in a hospital room during the day, using sound machines), bedtime routine building, parent education on good sleep habits, and sensory techniques for regulation before bedtime.
Despite the fact that sleep is addressed by the OTPF–4, all therapists reported that this topic had not been covered in their graduate schooling. Lack of knowledge was a pervasive theme across all interviews. Many felt that sleep topics should be addressed in graduate school as a foundational topic. Continuing education courses on sleep were noted to be difficult to find; however, many therapists shared that they had not thought of looking for courses focused on sleep intervention before participating in this study. Therapists who had sought out sleep education shared that they learned about sleep intervention ideas from conference presentations, training opportunities from different disciplines (e.g., psychology), coworkers within and outside of occupational therapy, books, and internet searches. Therapists felt that they lacked the depth of knowledge they needed to truly address the complex nature of sleep: “I cover sleep very superficially” (106). Therapists specifically felt that, beyond routine changes or sensory techniques at bedtime, they were at a loss as to what to do.
Overall, more than half of the therapists interviewed for this study voiced hesitancy surrounding sleep conversations with their clients and families: “In terms of my competency, no, I don’t feel confident because I don’t have the background knowledge for sleep” (111). Therapists who lacked confidence tended to be less experienced. Some therapists did feel confident in their abilities to address sleep. These therapists were more experienced (range = 6 yr–20+ years) and identified experiences with past clients and discussions with other professionals as key pieces that supported their practice. Many therapists identified their own experience having children as an instigator to consider sleep in their practice. One participant, who had been an occupational therapist for 22 yr, shared the following: I would say my first 10 years of practice, I never even thought about sleep. But after having my own children I think I started thinking more like, this is important. This is definitely the biggest life skill they have because without sleep, everything is off. Eating is off, play is off. It was important. I ask [about sleep] far more now after becoming a mother than I did in the first couple years. (102)
Across all settings, therapists shared that they often felt “spread thin” because of the many areas they address in therapy. They said they do not have the capacity to address sleep concerns in the way they wish they could. The idea of not having enough time—time to uncover sleep problems, time to fully address sleep concerns, time to educate themselves on best practice—was prevalent throughout the interviews: The conversation [on sleep] is not a fast one and you’re not getting the referral for poor sleep. . . . And so I think that’s why a lot of [occupational therapists] use tidbits . . . like weighted blankets. Because the conversation is not a fast one. (116)
Client and Family Factors
Pediatric occupational therapists are focused on the whole child, which often includes that child’s family unit dynamics. In certain settings, occupational therapists have regular access to caregivers and may even engage in therapy in the client’s home. Although the therapists in this study did not expressly identify regular caregiver communication as a support, those who did not have regular contact with caregivers (e.g., school therapists) identified this as a barrier to identifying and addressing sleep concerns.
The therapists who did regularly connect with caregivers reported that the caregivers are often “at the end of their rope” (102) and come into therapy with a list of pressing goal areas, often not involving sleep concerns. One quote from an occupational therapist who worked as an outpatient and early interventionalist in a rural area speaks to this point: While it would be wonderful to give [the parents], like, a sleep diary or, you know, all of these tools or these, like, long interventions, you know, elaborate, addressing exactly the thing . . . they just don’t have the capacity. And you as a therapist don’t have the capacity to do that either, because you’ve got so many different things. And I think that’s going to be a really important piece to kind of unpack is—how do we, like, figure out how to deliver this really important thing [sleep intervention]—sleep is so important[; it] impacts everything—in a way that parents are ready to receive it and therapists can give it? (116)
Identifying sleep as an area for intervention is sometimes difficult for pediatric occupational therapists because of limited access to caregivers (e.g., in a school setting), difficulties building rapport with families, or limited buy-in from families to engage in behavioral changes to improve sleep: “I always make sure that sleep is an important [issue] for the family before I try to intervene” (114). Therapists said that the topic of sleep can feel very personal and that sometimes families are not willing or ready to discuss sleep difficulties: “Sleep is intimate. . . . I’ll mention it, but if they don’t bite, then I drop it” (121). Therapists specifically said that caregivers may feel shame, judgment, or embarrassment about their sleep habits, leading caregivers to avoid bringing up the topic of sleep concerns: “As parents . . . you feel like that should be something that’s easy and it happens, naturally. And when it doesn’t it’s embarrassing, it is it’s hard to admit, and you feel like you failed” (123).
Setting-Specific Factors
The therapy setting was another factor that could either support or limit a therapist’s involvement in sleep assessment and intervention. Some settings, such as early intervention, were predominantly supportive of occupational therapy’s involvement in sleep concerns. Other therapists, in different settings, found considerable barriers to overcome when addressing sleep with their clients.
Outpatient Setting: Independent, Associated With a Hospital, or a Nonprofit Clinic
Outpatient therapists shared a variety of experiences and perspectives related to addressing sleep health with their clients. Half of the outpatient therapists shared that they had specific questions they ask parents to explore sleep in their evaluation or treatment sessions. Despite asking these questions, only 2 therapists reported writing a sleep-related goal in their practice. All therapists shared that they did not use a standardized sleep questionnaire or measurement tool in their practice: “I don’t have any formal sleep questions, but I’ll ask questions. It’s quite hit-and-miss. At the same time I’m trying to talk with the parents, the kid is running around the room” (121). With regard to reasons why they did not use a validated sleep measurement tool, some therapists cited a lack of tools validated for the special populations with whom they work, and others shared that they did not know of any sleep tools to use.
Early Intervention
The early intervention setting allows for occupational therapists to be embedded into the home environment and form relationships with the client (children ages 0–3 yr in most areas) and their caregivers. Early intervention therapists tended to feel more confident in addressing sleep but also reported feeling spread too thin to address sleep completely. They identified the fact that they are often in the home, conduct a routines-based interview during evaluation, have a service coordinator available, and attend regular interdisciplinary meetings that allow for collaboration and mentorship as facilitators of addressing sleep. In addition, some states have specific billing codes that allow therapists to spend time educating families, which is critical to sleep intervention.
School Systems
Occupational therapists who primarily worked in a school system reported that sleep comes up only if the child’s performance in school is affected by daytime fatigue. Half of the school-based therapists shared that they never thought about addressing sleep. School-based therapists who had thought about their client’s sleep reported that sleep is often not a primary focus of therapy because of restrictions placed on goal areas (e.g., goals must be education related) and limitations in access to caregivers for evaluation and education purposes. As such, school-based therapists reported that they focus on educating the child’s teacher: “I think it’s really just educating the teachers. Like when you see these kids come in a certain way [tired], I think we have to give them the grace for the day” (109).
Therapists commented on the impact of poor sleep on common problems seen in middle and high school, such as sloppy handwriting, agitation, anxiety, and overall poor mental health. However, many therapists did not feel comfortable addressing sleep concerns: “I just don’t feel like I have enough knowledge in sleep to really help them dig into it” (109).
Inpatient Settings: Acute Care and Rehabilitation
Inpatient therapists in this study worked in the pediatric intensive care unit, rehabilitation unit, oncology unit, and neonatal intensive care unit (NICU). They identified the critical role of sleep in the healing, growth, and development that are so important for the health of the children with whom they worked. However, when it comes to sleep intervention, inpatient clinicians noted that sleep was often not the focus of therapy unless they were working in the NICU: I would say there’s just other things that kind of take priority for us in an acute setting. Like their sleep—I think [it] is a given that it’s not going to be as great because they’re in the hospital for all these other reasons. (106)
Participants identified aspects like the hospital bed, client and family stress, pain, and multiple nighttime interruptions due to medical needs as all contributing to poor sleep in the hospital. Most of these are unable to be changed by the therapist or client: “There’s just so many things out of our control in my setting, like medications and pain level [of my clients]” (106).
In the NICU setting specifically, therapists reported that they often discussed sleep concerns with parents primarily because this involved the baby’s feeding routine, which is a common focus of occupational therapy in the NICU: “Sometimes, by asking about sleep, you can get a lot more information [about the child] a lot faster” (110). Despite discussing sleep concerns, NICU clinicians, like other inpatient clinicians, reported they do not write goals addressing sleep health: “I would say my goals are typically focused elsewhere. I don’t do a lot of sleep goals” (110).
External Factors
External factors are those that fall outside of the control of the occupational therapist and their practice setting that affect the occupational therapist’s perceived ability to assess sleep areas and intervene. These themes were centered around how other health care providers or caregivers view occupational therapists.
One dominant supportive external factor was that occupational therapists frequently work as part of a collaborative team and reported learning about sleep across traditional discipline areas. A therapist’s comfort with addressing sleep concerns was related to their view of their role on the team. Therapists who felt that they were seen within their team as the sleep expert spoke confidently about addressing sleep concerns with their clients. Those who mentioned having other clinicians on their team who address sleep (often a developmental specialist or psychologist) tended to speak about sleep not being their area of intervention: No one’s ever really taught [sleep education] to me. . . . I think there are other disciplines that I really appreciated . . . especially some of the behavioral approaches. I’ve appreciated hearing some of those and incorporating some of those strategies because I think that can be an important element sometimes. (115)
Having the confidence to work on the medical team and advocate for occupational therapy’s role in sleep intervention was a barrier noted by a number of participants across multiple settings. In general, therapists perceived that caregivers and other health care professionals did not see sleep as an aspect occupational therapists could address. “A lot of parents are like, ‘What is this [occupational therapy] thing anyway? I don’t understand it.’ I try to do my best to try to explain that [occupational therapists have] their hand[s] in everything” (121). One therapist put into words what it would take to move toward being seen as sleep experts: We could [specialize in sleep], but it’s going to require focus and also it would require a setting’s . . . I don’t want to say “permission,” but it’s kind of permission, to see us in that role. [Other health care professionals] see us as feeding specialists. They’re not looking to us for sleeping. (106)
Discussion
In this qualitative descriptive study, we explored the perspectives of pediatric occupational therapists on the role of sleep health in their practice. Overall, therapists recognized the importance of sleep and believed occupational therapy has a critical role in addressing sleep health. However, many therapists reported that they do not focus on sleep goals or use sleep outcome measures in their routine practice. During thematic exploration, we highlighted personal, client/family, setting-specific, and external factors that affect an occupational therapist’s ability to examine sleep health with their clients.
On the basis of our findings, we can identify some next steps to promote an increased focus on sleep health for pediatric occupational therapists. Building on previous reviews that have identified this gap in practice (Fung et al., 2013; Ho & Siu 2018; Tester & Foss, 2018), our data provide qualitative information about the lived experience of pediatric occupational therapists that influence their abilities to assess and address sleep concerns (e.g., confidence, therapy setting, supports, and barriers).
Consistent with survey findings in the published literature (Ludwig et al., 2022), more than half of the therapists we interviewed shared that they were not confident in their knowledge surrounding the intricacies of sleep. The overwhelming majority reported a lack of education opportunities in their graduate programs and continuing education courses related to sleep. The OTPF–4 identifies sleep as a foundational occupation and, as such, occupational therapy graduate programs could be prime avenues for increasing sleep education for future therapists. Therapists also identified the need for continuing education courses that focus on the more complex aspects of sleep and sleep intervention for therapists who want to specialize in sleep or require deeper knowledge in the area.
Pediatric sleep has been well studied, and frameworks to guide measurement and intervention have recently been presented (Allen et al., 2016; Meltzer et al., 2021). In addition, a recent systematic review found a total of five studies that examined occupation- or activity-based interventions in occupational therapy to improve sleep for children and adolescents (Beisbier & Laverdure, 2020). This work is encouraging and reflects the recent shift toward increasing awareness of sleep assessment and intervention. Occupational therapy research can continue to advance sleep research in special populations by merging sleep and occupational therapy frameworks to develop specialized care for children seen in clinics (Ho & Siu, 2018).
Study Strengths and Limitations
Efforts were made to report our findings in a comprehensive way. We used the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007) to ensure that each checklist item was covered in this article. We also took steps to increase the trustworthiness of the results, including recruiting a sample of occupational therapists across the country, capturing interview data through multiple tools (transcripts, interview notes, and a reflexive diary kept by the interviewer), the use of multiple coders, and a final member check to elucidate major themes.
This study represents the perspective of a small sample of pediatric occupational therapists who practice in the United States. Although thematic saturation was achieved with a sample size of 20, we recognize that factors such as geographic location, practice setting, and years of experience could have influenced the therapists’ perspectives. Future studies could explore a broader view of general occupational therapists or a more focused view of the effects of setting, geographic location, and so on, on a therapist’s perspective.
We recruited participants who volunteered for our study, which may have unintentionally resulted in a sample who was more interested in sleep. Our sample was predominantly made up of White, non-Hispanic, cisgender women. We were able to include some participants who identified with underrepresented groups in occupational therapy (e.g., male, non-White, nonbinary); however, a more diverse sample of therapists could offer a more widely representative reflection of perceptions. In addition, although our sample did include therapists who worked with clients of underrepresented populations (e.g., Native Alaskan, African American, located in urban school districts), the majority treated children who were White, non-Hispanic (about 70% of clients across all therapists).
Future Directions and a Call to Action
Our results highlight an opportunity for future education on sleep assessment and intervention for pediatric occupational therapists (Figure 2). Although most of the therapists in our study identified sleep as an important aspect of health for their clients, many said they lacked the education, confidence, tools, and opportunity to incorporate sleep interventions into their regular practice. Educators at universities and in continuing education courses are called to disseminate the existing knowledge surrounding sleep measurement and intervention. Sleep researchers are called to validate sleep measurement and intervention tools in special populations and disseminate findings to clinicians to advance sleep-focused interventions in the clinic. Advocacy for occupational therapy’s role in sleep health interventions within and outside of the field is essential.

Main findings and action items.
Implications for Occupational Therapy Practice
Hearing from the voices of pediatric occupational therapists in the United States allows us to reflect on how sleep health is addressed in our practice. Although a lack of knowledge and confidence were often identified as barriers, occupational therapists felt strongly that sleep is important and within their scope of practice. As such, these findings have the potential to change occupational therapy practice by ▪ bringing sleep to the forefront of the conversation with pediatric occupational therapists and ▪ highlighting the gap in sleep-focused education (continuing education and graduate training) that is available to occupational therapists.
Although it is clear there is an abundance of educational material incorporated into occupational therapy education programs, we believe our findings identify a key occupation that is overlooked in many graduate programs. We did not examine curricula development and organization, and therefore we cannot speak to how and where sleep education should be incorporated. We can, however, highlight that current occupational therapists report a desire to learn more about sleep.
Conclusion
This study highlights a critical opportunity for occupational therapists, occupational therapist educators, and sleep researchers to improve care for children who receive occupational therapy services. Occupational therapists in this study identified specific barriers that limit their ability to address sleep concerns. They also identified a lack of education materials that address sleep in special populations.
Footnotes
Acknowledgments
We thank the occupational therapy practitioners who shared their voices in this project. We also thank the University of Pittsburgh’s Department of Occupational Therapy, School of Health and Rehabilitation Sciences, and Center for Sleep and Circadian Science for supporting this project. Grant funding was given by the School of Health and Rehabilitation Science’s Research Development Fund (Amy G. Hartman). The results of this study were presented in Amy G. Hartman’s dissertation defense to the University of Pittsburgh’s Department of Occupational Therapy before publication.
Appendix: General Interview Questions
What is your experience addressing sleep concerns with your clients? How do you think a child’s sleep impacts their life and the goal areas on which you work? Tell me about how confident you are in talking about sleep with your clients and their caregivers. What are the supports and barriers that impact your ability to address sleep concerns?