
Abstract
This systematic review explains how virtual reality (VR) as an intervention has been used with children with cerebral palsy. The findings include a recommended minimum frequency for VR to be used in occupational therapy to yield noticeable improvements in upper extremity function and motor performance.
Active participation in occupations can promote, facilitate, support, and maintain people’s health and participation (American Occupational Therapy Association [AOTA], 2020). To support a client’s engagement in occupation, an occupational therapy practitioner designs and develops an occupation-based intervention plan (AOTA, 2020). A multitude of occupational therapy interventions allow occupational therapy practitioners to use evidence-based practice while exercising clinical reasoning to make advanced decisions that will enable clients to achieve their goals. Intervention services can address rehabilitation or restoration needs; provide support for, maintenance of, or modifications to aspects of promotion of health and wellness; and are intended for clients with both disability-related and non–disability-related needs (AOTA, 2020).
Cerebral palsy (CP), which has many etiologies, is a disorder that occurs during brain development or infancy and mainly affects movement, balance, tone, and posture (Bax et al., 2005; Vitrikas et al., 2020). This disorder is one of the most common physical disabilities seen among children, and although it is nonprogressive, secondary problems such as pain and dysfunction can arise (Vitrikas et al., 2020). Comorbidities such as intellectual disabilities, the inability to walk or speak, and behavioral or sleep disorders, as well as movement disorders such as ataxia, spasticity, or dyskinesia, may also be present (Vitrikas et al., 2020). A wide range of functional abilities are associated with clinical presentations of CP. Physical mobility and functional abilities range from being able to ambulate and handle objects independently to having severe mobility limitations and significantly reduced manual abilities (Almasri et al., 2018). Occupational therapy plays an important role with this population by providing interventions to enhance functional performance and promote independence in daily occupations (Steultjens et al., 2004). Additionally, occupational therapy practitioners use various evidence-based approaches and therapeutic interventions to encourage functional independence and enhance clients’ overall quality of life (Steultjens et al., 2004).
According to AOTA’s (2020) Occupational Therapy Practice Framework: Domain and Process (4th ed.), virtual interventions are defined as the “use of simulated, real-time, and near-time technologies for service delivery” (p. 62). In addition, virtual reality (VR) is defined as “synthetic environments consisting solely of computer-generated virtual objects” (Ferguson & Blackstock, 2019, p. 6). In occupational therapy, VR interventions typically tend to be focused on the functioning of the upper extremity (UE) and hand, cognitive rehabilitation, and mental disorders (Aran et al., 2017). VR has been used as an intervention method with both pediatric and adult populations to promote functional skills and encourage engagement in occupations (Aran et al., 2017).
Background Literature
Occupational therapy practitioners analyze clients’ motor performance when examining the ability to participate in meaningful occupations. Deficits in motor performance and UE functioning are commonly seen among children diagnosed with CP, and previous research has used VR to support the achievement of functional tasks and motor skills in rehabilitation (dePaula et al., 2017). VR interventions use both VR and virtual environments and are defined as simulation of real-world environments through a computer and experienced through a “human–machine interface” (Holden, 2005, p. 188). Currently, VR is used as an intervention by occupational therapy practitioners and other professionals for a variety of disorders, including but not limited to cerebrovascular accidents, Parkinson’s disease, musculoskeletal disorders, limb loss, burn care, psychological and cognitive disorders, and CP (Ferguson & Blackstock, 2019). Additionally, in terms of motor functioning, Holden (2005) described VR for rehabilitation as being provided clinically for orthopedic rehabilitation, mobility, and functional activities of daily living (ADLs).
Because of its ever-increasing technological advances and increasing accessibility, VR is a rapidly progressing method of intervention. This means that many types of VR exist and can be used for therapeutic intervention. Virtual environments exist on a reality–virtuality continuum (Figure 1) and include different immersion levels, such as nonimmersive, mixed, and immersive (Ferguson & Blackstock, 2019). Nonimmersive VR includes the use of mobile-sized or larger screens and incorporates video games, internet computer games, Wii games, Xbox Kinect, robotics, and exoskeletons. Mixed VR, also known as semi- immersive VR, includes both augmented reality and augmented virtuality. Augmented reality is defined as a “real environment viewed with a portion of VR added” (Ferguson & Blackstock, 2019, p. 7), with an example being Pokémon Go. Augmented virtuality is defined as “VR viewed with a portion of the real environment added” (Ferguson & Blackstock, 2019, p. 7), and an example is the PlayStation EyeToy. Immersive VR can include a head-mounted display with or without body tracking, Oculus, or a PlayStation 4 VR system. A variety of VR interventions are used in clinical rehabilitation settings to treat children diagnosed with CP (Ferguson & Blackstock, 2019). The specific types of VR included in this review are defined according to their respective study and VR classification and are listed in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
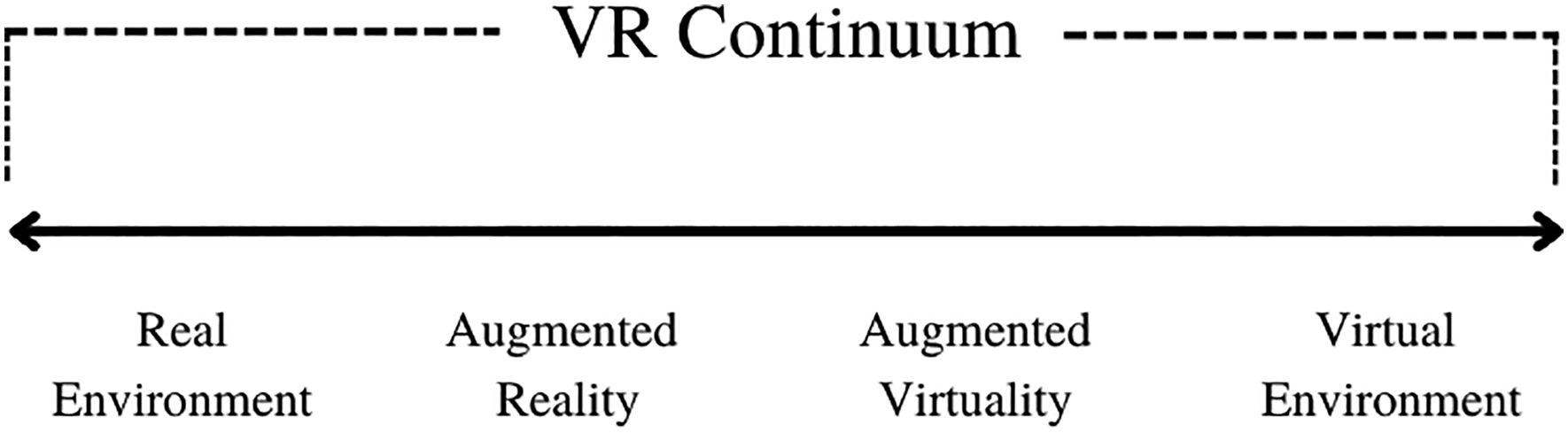
VR continuum.
Statement of Problem
Currently, research on the functional and motor performance impact of VR as an intervention tool for children with CP is limited. This review addressed the impact of VR on UE function and motor performance of children diagnosed with CP by summarizing the results of studies that implemented VR as an intervention for children with CP. A critical investigation of the findings provides the potential for occupational therapy practitioners to gain increased evidence-based knowledge in this specialty area. Additionally, continued research on VR is necessary to understand and apply the use of evidence-based practice in occupational therapy rehabilitation and to further the use of VR as an intervention method. This systematic review looked at the impact of VR in terms of noticeable improvements that occurred in UE function and motor performance among children diagnosed with CP.
Method
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and followed the Cochrane Collaboration methodology throughout the entirety of this review (Higgins et al., 2019; Moher et al., 2009). Each author independently conducted an extensive literature search to identify appropriate articles for the review. The inclusion criteria for the literature search were as follows: (1) children ages 0 to 21 yr with any type of CP diagnosis, (2) use of VR as an intervention method, and (3) outcomes that included measures of UE function and motor performance. Studies were excluded if they were published in a language other than English or if they did not include UE function and motor performance as outcomes.
Seven databases were searched: EBSCOhost, One Search, PubMed, Cloud Source, CINAHL, SPORTDiscus, and Google Scholar. Studies published since 2006 that had full-text availability were included. Key search terms used during the literature search were VR, video games, cerebral palsy, occupational therapy, motor performance, motor development, and randomized controlled trial. The search identified a total of 7,408 studies. During the screening process, studies were excluded if they did not have a results section, did not have an experimental design, or were published before 2006 (see Figure 2 for the flow of articles through the review process).
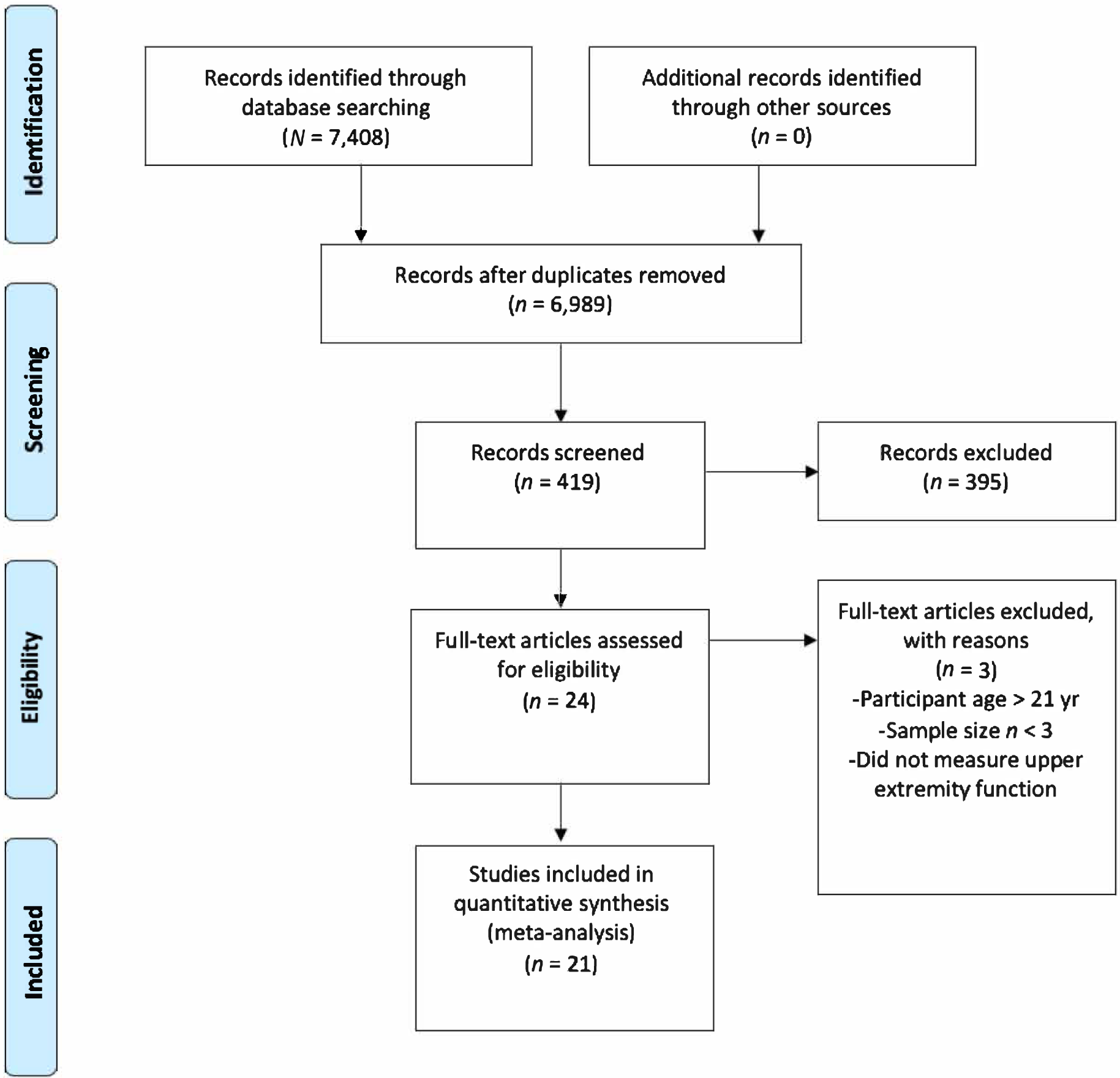
Flow of articles through the systematic review process.
The levels of evidence were classified and determined in accordance with the Oxford Centre for Evidence-Based Medicine (OCEBM; 2009) and the U.S. Preventive Services Task Force (2018). According to OCEBM (2009), Level 1b studies are well-designed randomized controlled trials (RCTs); Level 2b studies are prospective cohort studies, ecological studies, low-quality RCTs, and nonrandomized studies; and Level 3b studies are individual case–control; one-group, nonrandomized pretest–posttest; or cohort studies. According to the U.S. Preventive Services Task Force (2018), strong evidence results from 2 or more Level 1a or 1b studies, and moderate evidence results from at least 1 Level 1a or 1b or multiple Level 2a or 2b or Level 3a or 3b studies. Low evidence stems from a small number of low-level studies. Studies included in this review were identified as Level 1b, 2b, or 3b.
Results
A total of 21 studies were included. Relevant evidence pertaining to each study was synthesized, and an in-depth summary relating to each study’s participant criteria, VR intervention methods, and outcomes can be found in Table A.2 in the Supplemental Material. According to the OCEBM (2009), 9 studies were Level 1b, 8 were Level 2b, and 6 were Level 3b. Of the 21 studies, 15 were classified as RCTs, and 6 were classified as one-group pretest– posttest. Risk of bias was determined using the Cochrane tool (Higgins et al., 2016) and can be found in Tables A.3 and A.4 for RCTs and non-RCTs and pretest–posttest study designs, respectively. The results have been categorized here by common themes found during the review.
Participant Eligibility
Of the studies that specified the type of CP, the majority of children included were diagnosed with spastic hemiplegia (Arnoni et al., 2018; Chiu et al., 2014; Şahin et al., 2020; Sevick et al., 2016; Urgen et al., 2016). Three additional studies included children with hemiplegic CP, but the degree of muscle tone was not indicated (Fluet et al., 2010; Luna-Oliva et al., 2013; Tarakci et al., 2016). Two studies also included children with diplegic involvement (Luna-Oliva et al., 2013; Tarakci et al., 2016). Additionally, 1 study included children with dyskinesia (Tarakci et al., 2016). Eight studies specified the type of CP diagnosis (Arnoni et al., 2018; Chiu et al., 2014; Fluet et al., 2010; Jha et al., 2021; Luna-Oliva et al., 2013; Şahin et al., 2020; Sevick et al., 2016; Tarakci et al., 2016), and the others did not.
Functional Classification
Functional classification can be used to describe the wide range of functional abilities among children with CP. The Manual Ability Classification System (MACS) and Gross Motor Function Classification System (GMFCS) provide distinctive information related to the manual abilities of children diagnosed with CP (Almasri et al., 2018). The MACS was developed to classify the manual abilities of children with CP (Eliasson et al., 2006). Eight studies included children if their MACS scores were Levels I to IV (Choi et al., 2021; Gilliaux et al., 2015; James et al., 2015; Jha et al., 2021; Piovesana et al., 2017; Preston et al., 2016; Şahin et al., 2020; Sevick et al., 2016). The GMFCS classifies children with CP on the basis of their gross motor function by measuring functional activities (Palisano et al., 1997). Eight studies included children if they scored at Levels I to IV on the GMFCS (Arnoni et al., 2018; James et al., 2015; Jha et al., 2021; Piovesana et al., 2017; Sevick et al., 2016; Tarakci et al., 2016; Urgen et al., 2016; Zoccolillo et al., 2015). This criterion ensured that all children had similar baseline abilities before participation in the respective study.
More than half of the studies (n = 13) required children to have a normal cognitive level, demonstrated by the child’s ability to comprehend and follow verbal instructions (Arnoni et al., 2018; Chiu et al., 2014; Choi et al., 2021; Gilliaux et al., 2015; Jha et al., 2021; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Piovesana et al., 2017; Preston et al., 2016; Reid & Campbell, 2006; Sajan et al., 2017; Tarakci et al., 2016; Urgen et al., 2016). Eight studies required children to have normal corrected vision and hearing (Chiu et al., 2014; Choi et al., 2021; Jha et al., 2021; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Preston et al., 2016; Urgen et al., 2016; Winkels et al., 2013). Six studies excluded children who received botulinum injections (Choi et al., 2021; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Şahin et al., 2020; Tarakci et al., 2016; Urgen et al., 2016).
Age of Children in the Studies
Children’s age range was 4 to 20 yr. Most studies (n = 17) had a mean age range of 5 to 11 yr (Chiu et al., 2014; Choi et al., 2021; Fluet et al., 2010; Gilliaux et al., 2015; James et al., 2015; Jha et al., 2021; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Piovesana et al., 2017; Reid & Campbell, 2006; Şahin et al., 2020; Sajan et al., 2017; Sevick et al., 2016; Sharan et al., 2012; Urgen et al., 2016, Weightman et al., 2011., Zoccolillo et al., 2015). Four studies included children with a mean age of 8 yr or younger (Choi et al., 2021; Luna-Oliva et al., 2013; Weightman et al., 2011; Zoccolillo et al., 2015).
Types of VR Intervention
Table A.1 compares the different types of VR systems these studies used as well as their respective classification. Fifteen studies used nonimmersive VR. Six of these studies used Nintendo WiiTM Sports Resort and Wii Fit (Chiu et al., 2014; Sajan et al., 2017; Sharan et al., 2012; Tarakci et al., 2016, Urgen et al., 2016; Winkels et al., 2013). An additional 5 studies, also using nonimmersive VR, used the Kinect-based Xbox System (Arnoni et al., 2018; Jha et al., 2021; Luna-Oliva et al., 2013; Şahin et al., 2020; Zoccolillo et al., 2015). Two studies used a Web-based home program called Move it to improve it (Mitii), a type of nonimmersive VR (James et al., 2015; Piovesana et al., 2017). Preston et al. (2016) used a computer-assisted arm VR rehabilitation method, also classified as nonimmersive VR. Metin Ökmen et al. (2019) used PlayStation EyeToy, which is classified as a type of augmented virtuality. Gilliaux et al. (2015) conducted robot-assisted therapy (RAT), a semi-immersive type of VR, and Choi et al. (2021) used RAPAEL Smart Kids for hand function, which is also classified as semi-immersive. Additionally, Sevick et al. (2016) used a semi-immersive individualized UE VR training regimen. One study used a home-based VR rehabilitation system approach that is classified as nonimmersive VR (Weightman et al., 2011).
VR Intervention Frequency and Duration
Seven studies conducted VR sessions for 30 to 45 min. James et al. (2015) and Piovesana et al. (2017) both conducted 20- to 30-min sessions 6 days/wk for 20 wk (3,600 min total). Preston et al. (2016) encouraged 30-min home VR sessions every day for 12 wk (2,520 min total). Choi et al. (2021) conducted 30-min sessions of VR combined with 30 min of conventional occupational therapy 5 days/wk for 4 wk (1,200 min total). Jha et al. (2021) used 30-min VR sessions and 30 min of combined VR and physical therapy 4 days/wk for 6 wk (720 min total of VR, 720 min total of combined VR and PT). Chiu et al. (2014) used VR for 40-min sessions 3×/wk for 6 wk (720 min total). Zoccolillo et al. (2015) conducted 30-min VR sessions and 30 min of conventional therapy 2×/wk for 8 wk (VR, 480 min total; conventional therapy, 480 min total).
Another 7 studies conducted VR sessions for 45 to 60 min. Two studies conducted 45-min sessions 2×/wk for 8 wk (720 min total; Arnoni et al., 2018; Şahin et al., 2020). Sajan et al. (2017) conducted 45-min sessions 6 days/wk for 3 wk (810 min total), and Gilliaux et al. (2015) conducted 45-min sessions of RAT 5×/wk for 8 wk (1,800 min total). Urgen et al. (2016) used 45-min VR sessions 2×/wk for 9 wk (810 min total), and Tarakci et al. (2016) held 50-min sessions 2×/wk for 12 wk (1,200 min total). Fluet et al. (2010) used VR for 60-min sessions 3×/wk for 3 wk (540 min total).
Arnoni et al. (2018) used 45 min of VR intervention 2×/wk for 8 wk (720 min total). Luna-Oliva et al. (2013) used VR for 30-min sessions 2 days/wk for 8 wk (480 min total). Sevick et al. (2016) used VR for 60 min 3×/wk for 12 wk (2,160 min total). Weightman et al. (2011) used VR at home and encouraged the children to use VR as much as they could over 4 wk. Winkels et al. (2013) used VR for 30-min sessions 2×/wk for 6 wk (360 min total). Each of these studies (n = 5) was classified as having a single-group pretest–posttest design.
Overall, the amount of VR intervention ranged from a low of 360 total min (Winkels et al., 2013) to a high of 3,600 total min (James et al., 2015; Piovesana et al., 2017). Ten studies compared VR plus conventional treatment with conventional treatment only (Chiu et al., 2014; Choi et al., 2021; Gilliaux et al., 2015; Jha et al., 2021; Metin Ökmen et al., 2019; Şahin et al., 2020; Sharan et al., 2012; Tarakci et al., 2016; Urgen et al., 2016; Zoccolillo et al., 2015). Five studies compared VR only with conventional treatment (James et al., 2015; Piovesana et al., 2017; Preston et al., 2016; Reid & Campbell, 2006; Sajan et al., 2017). One study used three groups to compare VR in a sitting position with and without support with VR with both support and constraint-induced movement therapy (Fluet et al., 2010). Zoccolillo et al. (2015) was the only crossover trial RCT, in which children in the VR group were compared with children who received conventional treatment. The groups switched after 8 wk so that every child received the other treatment.
UE Function Findings
Twelve studies found statistically significant improvements in upper limb and hand function in children with CP (Chiu et al., 2014; Choi et al., 2021; Fluet et al., 2010; Gilliaux et al., 2015; James et al., 2015; Metin Ökmen et al., 2019; Preston et al., 2016; Sajan et al., 2017; Sevick et al., 2016; Sharan et al., 2012; Winkels et al., 2013; Zoccolillo et al., 2015). These studies ranged from lows of 360 (Winkels et al., 2013) to 540 (Fluet et al., 2010) total minutes of VR intervention to highs of 2,160 (Sevick et al., 2016) to 3,600 (James et al., 2015) min. Interventions occurred for a minimum of 3 wk (Fluet et al., 2010; Sajan et al., 2017; Sharan et al., 2012) and a maximum of 20 wk (James et al., 2015). Five studies conducted VR intervention for 8 to 12 wk (Gilliaux et al., 2015; Metin Ökmen et al., 2019; Preston et al., 2016; Sevick et al., 2016; Zoccolillo et al., 2015).
UE Function Measures
Measures used to assess upper limb and hand function include the Melbourne Assessment of Unilateral Upper Limb Function Test (MAUULF; Fluet et al., 2010), Quality of Upper Extremity Skills Test (QUEST; Gilliaux et al., 2015; Sajan et al., 2017; Zoccolillo et al., 2015), ABILHAND–Kids (Gilliaux et al., 2015; Preston et al., 2016; Winkels et al., 2013; Zoccolillo et al., 2015), Box and Block Test (BBT; Gilliaux et al., 2015; Sajan et al., 2017), Bimanual Fine Motor Function (Metin Ökmen et al., 2019), Modified Functional Reach Test (Sevick et al., 2016), active range of motion (AROM; Sevick et al., 2016), Melbourne Assessment 2 (MA2; Choi et al., 2021; Winkels et al., 2013), MACS (James et al., 2015; Sharan et al., 2012), and the Upper Limb Physician’s Rating Scale (ULPRS; Choi et al., 2021).
Choi et al. (2021) found significant improvements in forearm supination AROM in the intervention group compared with the control group. The MA2 subscales, including ROM, accuracy, dexterity, and fluency, improved for both groups, as did segmental movements in the affected limb using the ULPRS (Choi et al., 2021). Participants in all three study groups of Fluet et al. (2010) showed statistically significant improvements in MAUULF scores, including forward reach times, reach sideways time, hand-to-mouth, composite time, shoulder flexion, and grip. Winkels et al. (2013) found significant differences in two-handed daily activity performance. Sharan et al. (2012) found significant improvement in manual ability based on the MACS after treatment of both the study and control groups. Choi et al. (2021) found significant improvements among children with more severe motor impairments than among those with less severe impairments, as measured by the MACS. However, 3 studies did not find improvements in any component of arm movement or reach (James et al., 2015; Weightman et al., 2011; Winkels et al., 2013) or unilateral upper limb function (James et al., 2015).
Seven studies found statistically significant improvements in fine motor skills in children with CP (Chiu et al., 2014; Gilliaux et al., 2015; James et al., 2015; Luna-Oliva et al., 2013; Şahin et al., 2020; Sajan et al., 2017; Zoccolillo et al., 2015). These studies ranged from a low of 480 min of VR intervention (Luna-Oliva et al., 2013) to a high of 3,600 min (James et al., 2015). The remaining studies ranged from 720 min to 1,800 min of intervention (Chiu et al., 2014; Gilliaux et al., 2015; Şahin et al., 2020; Sajan et al., 2017; Zoccolillo et al., 2015). The interventions occurred for a minimum of 3 wk (Sajan et al., 2017) and a maximum of 20 wk (James et al., 2015). More than half of the interventions in these 7 studies lasted for 6 to 8 wk (Chiu et al., 2014; Gilliaux et al., 2015; Luna-Oliva et al., 2013; Şahin et al., 2020; Zoccolillo et al., 2015).
Fine Motor Skills Measures
Measures used to assess improvements in fine motor skills included the Jebsen–Taylor Test of Hand Function (JHFT; Chiu et al., 2014; James et al., 2015; Luna-Oliva et al., 2013), Bruininks–Oseretsky Test of Motor Proficiency–Short Form (BOTMP–SF; Şahin et al., 2020), and QUEST (Gilliaux et al., 2015; Sajan et al., 2017; Zoccolillo et al., 2015).
Chiu et al. (2014) found increased grip strength in the intervention group, and Gilliaux et al. (2015) found significant improvements in manual dexterity of the upper limb among children who received RAT compared with those who received conventional therapy. The dissociated movements score on the QUEST increased in both groups (Gilliaux et al., 2015). James et al. (2015) found that the intervention group had significantly higher postintervention JHFT scores for the dominant upper limb compared with the control group. In three administrations of the JHFT, Luna-Oliva et al. (2013) also found significant improvements over time for each item, with the exclusion of lifting large or heavy objects. Şahin et al. (2020) found significantly greater improvements in fine motor functions and daily activities in the intervention group than in the traditional occupational therapy group. Sajan et al. (2017) found significant improvements in upper limb function as indicated by total QUEST scores and in grasp and dissociated movements subtests for the intervention group but not the control group. Manual dexterity significantly improved for both the intervention and the control groups, as seen in BBT scores. Sajan et al. (2017) noted significant improvements in upper limb function in the intervention group compared with the control group. Zoccolillo et al. (2015) found significant increases in the quantity of limb-performed movement after video game–based therapy compared with conventional therapy. They also found significant differences in the amount of movement of the paretic side versus the other side after VGT (Zoccolillo et al., 2015).
UE Function Levels of Evidence
Of the 12 studies focusing on UE function, 4 were classified as Level 1b (Chiu et al., 2014; Choi et al., 2021; Metin Ökmen et al., 2019; Şahin et al., 2020). Six of the 12 studies were classified as Level 2b (Fluet et al., 2010; Gilliaux et al., 2015; Preston et al., 2016; Sajan et al., 2017; Sharan et al., 2012; Zoccolillo et al., 2015), and the remaining 2 studies were classified as Level 3b (Sevick et al., 2016; Winkels et al., 2013).
Of the 7 studies addressing fine motor skills, 3 were classified as Level 1b (Chiu et al., 2014; James et al., 2015; Şahin et al., 2020), 3 were classified as Level 2b (Gilliaux et al., 2015; Sajan et al., 2017; Zoccolillo et al., 2015), and 1 was classified as Level 3b (Luna-Oliva et al., 2013). Although a majority of the studies provided significant results for the JHFT, Chiu et al.’s (2014) results did not show changes in hand function and coordination.
Additional Findings
In addition to including outcome measures of UE function and fine motor performance, many studies focused on other skills or abilities that affect UE function, such as functional mobility, gross motor performance, occupational performance, intrinsic factors, caregiver perceptions, and visual–perceptual motor skills. Although not the primary purpose of this review, these findings are reported in addition to the primary findings and are discussed individually.
Functional Mobility
Four studies found statistically significant improvements in functional mobility (Choi et al., 2021; Metin Ökmen et al., 2019; Tarakci et al., 2016; Urgen et al., 2016). These studies ranged from a low of 720 total minutes of VR intervention (Metin Ökmen et al., 2019) to a high of 1,200 min (Choi et al., 2021; Tarakci et al., 2016). The remaining studies ranged from 720 min (Metin Ökmen et al., 2019) to 810 min (Urgen et al., 2016). Intervention occurred for a minimum of 4 wk (Choi et al., 2021) to a maximum of 12 wk (Metin Ökmen et al., 2019; Tarakci et al., 2016).
Measures used to assess functional mobility included the Pediatric Evaluation of Disability Inventory (PEDI; Urgen et al., 2016), Pediatric Evaluation of Disability Inventory Computer Adaptive Test (PEDI– CAT; Choi et al., 2021), Functional Mobility Scale (FMS; Metin Ökmen et al., 2019), and Functional Forward Reach Test (FFRT; Tarakci et al., 2016). Metin Ökmen et al. (2019) found a significant increase in posttreatment FMS scores for the intervention group. Every FFRT subtest score increased significantly (Tarakci et al., 2016). Tarakci et al. (2016) and Şahin et al. (2020) noted significant improvements in locomotion subtests. Tarakci et al. (2016) found that transfers did not change on the Functional Independence Measure for Children (WeeFIM).
Gross Motor Improvement
Ten studies found statistically significant improvements in gross motor function for children with CP (Arnoni et al., 2018; James et al., 2015; Jha et al., 2021; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Şahin et al., 2020; Sevick et al., 2016; Tarakci et al., 2016; Urgen et al., 2016; Weightman et al., 2011). These studies ranged from a low of 480 min of VR intervention (Luna-Oliva et al., 2013) to a high of 3,600 min (James et al., 2015). Intervention occurred for a minimum of 6 wk (Jha et al., 2021) to a maximum of 20 wk (James et al., 2015). More than half of these studies conducted VR sessions for a duration of 8 to 12 wk (Arnoni et al., 2018; Luna-Oliva et al., 2013; Metin Ökmen et al., 2019; Şahin et al., 2020; Sevick et al., 2016; Tarakci et al., 2016; Urgen et al., 2016).
Measures used to assess gross motor improvement included the Assessment of Motor and Process Skills (AMPS; James et al., 2015; Luna-Oliva et al., 2013), Gross Motor Function Measure (GMFM; Luna-Oliva et al., 2013), Pediatric Reach Test (Luna-Oliva et al., 2013), General Motor Quotient (GMQ; Arnoni et al., 2018), FFRT and Functional Sideways Reach Test (FSRT; Tarakci et al., 2016), Kids-Mini-BESTest (Jha et al., 2021), BOTMP–SF (Şahin et al., 2020), Movement Assessment Battery for Children (M–ABC; Weightman et al., 2011), Bruininks–Oseretsky Test of Motor Proficiency, Second Edition (BOT–2; Sevick et al., 2016), and Gross Motor Performance Measure (GMPM) and GMFM (Urgen et al., 2016).
Arnoni et al. (2018) observed improved GMQ and Motor Developmental Scale (MDS; Motor Quotient 1) scores. Both James et al. (2015) and Luna-Oliva et al. (2013) found significant differences on both the Motor and the Process scales of the AMPS. Jha et al. (2021) found significant improvements in balance assessed with both the Paediatric Balance Scale (PBS) and the Kids-Mini-BESTest. Tarakci et al. (2016) also found significant increases in gross motor components, such as balance, using the sit-to-stand, TUG, FSRT, and FFRT. Şahin et al. (2020) found significant improvements in gross motor scores as measured with the BOTMP–SF. Sevick et al. (2016) noted a significant overall increase in upper limb coordination on the BOT–2. Urgen et al. (2016) found significant between-groups differences in scores on both the GMPM and the GMFM, and significant between-groups differences in balance reactions as assessed with the PBS were noted (Urgen et al., 2016). Weightman et al. (2011) found significant preintervention–postintervention differences in movement time and peak speed but had no significant findings in the quality of reaching movements pre- to postintervention for time to peak speed and movement jerkiness.
Of these 10 studies, 6 were classified as Level 1b (James et al., 2015; Jha et al., 2021; Metin Ökmen et al., 2019; Şahin et al., 2020; Tarakci et al., 2016; Urgen et al., 2016), and 4 were classified as Level 3b (Arnoni et al., 2018; Luna-Oliva et al., 2013; Sevick et al., 2016; Weightman et al., 2011).
Occupational Performance and Functional Independence
Eight studies in this review found a statistically significant increase in independence in daily life and occupational performance after VR intervention (Arnoni et al., 2018; Chiu et al., 2014; Choi et al., 2021; James et al., 2015; Reid & Campbell, 2006; Sevick et al., 2016; Sharan et al., 2012; Winkels et al., 2013). These studies ranged from a low of 360 min total of VR intervention (Winkels et al., 2013) to a high of 3,600 min (James et al., 2015). The intervention lasted for a minimum of 2 wk (Arnoni et al., 2018) to a maximum of 20 wk (James et al., 2015).
Three studies used the Canadian Occupational Performance Measure (COPM) to measure occupational performance (James et al., 2015; Preston et al., 2016; Weightman et al., 2011). Choi et al. (2021) found improvements in ADLs, as demonstrated by the PEDI–CAT, in the intervention group compared with the control group. James et al. (2015) found significantly higher postintervention scores on the COPM for the intervention group compared with the control group. Preston et al. (2016) and Weightman et al. (2011) both found significant improvements in COPM scores from pre- to postintervention.
Two studies used the WeeFIM to assess independence and function (Şahin et al., 2020; Tarakci et al., 2016). Both Tarakci et al. (2016) and Şahin et al. (2020) noted significant improvements in self-care. Şahin et al. (2020) noted significantly greater WeeFIM total scores for independence in the intervention group compared with the control group.
Intrinsic Factors
Intrinsic factors, such as self-perception, self-concept, and satisfaction, were measured in 7 studies (Arnoni et al., 2018; Chiu et al., 2014; James et al., 2015; Reid & Campbell, 2006; Sevick et al., 2016; Sharan et al., 2012; Winkels et al., 2013). These studies ranged from a low of 360 total min of VR intervention (Winkels et al., 2013) to a high of 3,600 min (Sevick et al., 2016). Three of the 7 studies included a total of 720 min of VR intervention (Arnoni et al., 2018; Chiu et al., 2014; Reid & Campbell, 2006). The interventions occurred for a minimum of 3 to 6 wk (Chiu et al., 2014; Sharan et al., 2012; Winkels et al., 2013) and a maximum of 20 wk (James et al., 2015).
Reid and Campbell (2006) found significant improvements on the Social Acceptance subscale of the Harter Self Perception Profile for Children for the intervention group receiving VR intervention. Sharan et al. (2012) found significantly higher scores on the Participation Satisfaction Cooperation Motivational Factors (PSCM) for the intervention group compared with the control group in areas such as participation, satisfaction, cooperation, and motivation. Winkels et al. (2013) found high satisfaction with VR training, as determined with a visual analog scale. James et al. (2015) found significantly higher COPM Performance and Satisfaction scores among the intervention group than the comparison group. Sevick et al. (2016) found high levels of motivation among children on the Intrinsic Motivation Inventory. Arnoni et al. (2018) found significant differences in many areas addressed by the Piers–Harris Children’s Self-Concept Scale, including decreased anxiety and improvements in intellectual and school status, popularity, physical appearance, satisfaction, and happiness.
Caregivers’ Perceptions
One study examined caregivers’ perceptions during VR intervention (Chiu et al., 2014). This study had a total of 120 min of VR intervention each week for a duration of 6 wk. Measurements used to assess caregiver perception included the Functional Use Survey (Chiu et al., 2014). Chiu et al. (2014) found a higher use of hands, according to caregivers’ perceptions, among the intervention group compared with the control group, after 6 wk of VR. However, no difference was found in caregivers’ perception of the quality of hand function at any point in time.
Visual–Perceptual and Motor Skills
One study (James et al., 2015) found statistically significant improvements in visual–perceptual skills in children with CP. This study had a total 3,600 min of VR intervention, which took place 6 days/wk for 20 wk. James et al. (2015) used the Test of Visual Perceptual Skill, Third Edition, and found significant improvements in spatial relations and visual closure. However, the findings in visual memory, form constancy, sequential memory, and figure–ground discrimination were nonsignificant (James et al., 2015). Zoccolillo et al.’s (2015) findings for functional visual–motor integration on the Visual–Motor Integration Functional Scale were nonsignificant.
Discussion
Within the past 16 yr, VR-based interventions have been used worldwide as supplemental or primary therapy interventions for children diagnosed with CP. The results of this systematic review provide promising evidence for continued use of VR in occupational therapy interventions. In terms of VR intervention, statistically significant improvements were noted in UE function, fine motor skills, and functional mobility.
To summarize, the evidence appears promising for improvements in UE function when VR-based intervention is provided to children with CP (4 Level 1b, 6 Level 2b, and 2 Level 3b studies). It also appears that fine motor skills may be improved when VR-based intervention is provided to children with various CP diagnoses (4 Level 1b, 2 Level 2b, and 1 Level 3b studies). Four studies classified as Level 1b (Choi et al., 2021; Metin Ökmen et al., 2019; Tarakci et al., 2016; Urgen et al., 2016) found that functional mobility and gross motor performance can improve when VR-based intervention is provided. However, 2 studies found nonsignificant improvements in balance (Sajan et al., 2017; Urgen et al., 2016). Additional findings support the potential for increased independence and overall occupational performance in daily life when VR-based interventions are used (4 Level 1b, 1 Level 2b, and 3 Level 3b studies). However, the studies did not report specific ADLs that improved as a result of VR intervention. The use of VR as an intervention may increase intrinsic factors (2 Level 1b, 2 Level 2b, and 3 Level 3b studies) and improve caregivers’ perceptions (1 Level 1b study). Last, visual–perceptual skills may be improved when VR-based intervention is provided to children with CP (1 Level 1b and 1 Level 2b study), but the results of the studies varied in the area of visual perception that improved.
Studies included in this review varied in the form of VR used, including immersion levels, frequency and duration of VR intervention, and intensity. On the basis of our results, it appears that better UE outcomes are achieved when VR is implemented for at least 360 min, for a minimum of 3 wk or more, with sessions ranging from 30 to 60 min each. The effects of VR on UE function, motor performance, and fine motor skills, when used for less than 3 wk or less than 360 min, is unclear. Similarly, it is unclear how significant the improvements are when VR is used for more than 20 wk and 3,600 min. There is potential for increased improvements in UE function and motor performance with greater use of VR intervention. Occupational therapy practitioners should use their clinical judgment when deciding on the intensity and frequency for their client’s specific needs and goals.
Overall, the evidence supporting the use of VR-based interventions to improve UE function and motor performance of children diagnosed with different types of CP appears to be promising. Although not the focus of this review, evidence suggests that VR can affect functional mobility, gross motor skills, occupational performance, intrinsic factors, caregivers’ perceptions, and visual–perceptual skills. VR-based interventions to support functional improvement and UE function can take place in the child’s home or at the clinic. Although which type of VR intervention provides the most significant overall improvement for children with CP is unclear, VR appears to be effective in improving UE function when used as a primary or supplemental intervention during occupational therapy treatment.
Limitations
Variations in the frequency and type of VR intervention and the different assessments that were used proved challenging when comparing the results of different studies. The most common limitation found among the studies was the lack of consistency in the definition of VR. For example, some studies included nonimmersive VR or video game–based therapies such as the Wii and Xbox Kinect (Arnoni et el., 2018; Chiu et al., 2014; Jha et al., 2021; Luna-Oliva et al., 2013; Sajan et al., 2017; Sharan et al., 2012; Tarakci et al., 2016; Urgen et al., 2016; Winkels et al., 2013). Another study, although still classified as nonimmersive, used strictly computer-based and computer-assisted treatment games (Preston et al., 2016). The remaining studies were classified as semi-immersive VR and involved various programming and technologies (Choi et al., 2021; Fluet et al., 2010; Gilliaux et al., 2015; James et al., 2015; Metin Ökmen et al., 2019; Piovesana et al., 2017; Reid & Campbell, 2006; Şahin et al., 2020; Sevick et al., 2016; Weightman et al., 2011; Zoccolillo et al., 2015). Measuring the impact of therapies that vary so greatly in their administration affected our ability to draw conclusions from the results and made it difficult to determine whether one VR intervention method provided greater results than another. Because of the wide variety of VR-based interventions used in the various studies, it is difficult to conclude that one type of VR was better than another in affecting UE motor performance. Additionally, because of the limited availability of RCTs focusing on the treatment setting (home or clinic), it is unclear whether the results and outcomes of VR intervention are better when used in one location or another.
UE motor function outcome measures varied in whether they measured hand function, fine motor skills, or UE function as a whole. Hand function can be measured with the QUEST, JHFT, BBT, and others. However, these same assessments were also used to examine UE functioning and performance. There was little consistency in the studies in measuring UE, hand function, and fine motor abilities. To create consistency, future studies should focus on using similar outcome measures when testing for significant and insignificant improvements in specific areas.
There was also a lack of consistency in children’s baseline impairments; some studies included only children with MACS and GMFCS scores indicating high functioning (Arnoni et al., 2018; Piovesana et al., 2017; Şahin et al., 2020; Sevick et al., 2016; Tarakci et al., 2016; Urgen et al., 2016), and others included a wider variety of abilities (Arnoni et al., 2018; Choi et al., 2021; Gilliaux et al., 2015; Jha et al., 2021; Zoccolillo et al., 2015). Another limitation identified is the variation in the type of CP diagnosis for the children in the studies. Only 8 of the 21 studies identified the specific CP diagnoses of the children included in the study, and these varied among hemiplegia, spastic hemiplegia, diplegia, and dyskinetic CP (Arnoni et al., 2018; Chiu et al., 2014; Fluet et al., 2010; Jha et al., 2021; Luna-Oliva et al., 2013; Şahin et al., 2020; Sevick et al., 2016; Tarakci et al., 2016). Future research should focus on the results of VR intervention in terms of the specific type of CP diagnosis and the child’s functional abilities before using VR. This would potentially allow researchers to determine whether children with one type of CP can reap more benefits from VR-based interventions than those with other types of CP.
Overall, sample sizes in the included studies were relatively small. Three studies included samples consisting of fewer than 10 participants (Arnoni et al., 2018; Fluet et al., 2010; Sevick et al., 2016). None of the studies completed a power analysis to determine an appropriate sample size. However, 2 studies included more than 100 children (James et al., 2015; Piovesana et al., 2017). Four other studies included more than 50 children (Chiu et al., 2014; Choi et al., 2021; Şahin et al., 2020).
In the current literature, the variability in children’s ages and degree and diagnosis of CP, lack of a power analysis, wide variety of outcome measures, and varying definitions of VR limited the conclusiveness of the findings. However, the evidence appears to suggest the potential for improvements in UE function and motor performance with several additional findings that affect a child’s participation in occupations.
Implications for Occupational Therapy Practice
This review has the following implications for occupational therapy practice: ▪ Occupational therapy practitioners should be aware of the benefits VR interventions can provide for children diagnosed with CP, and they should evaluate and assess their clients to determine their needs and goals before implementing VR-based intervention methods. ▪ Because VR technology can be used at home, VR can be implemented as a supplement to traditional therapy interventions. Occupational therapy practitioners should consider recommending home-based VR intervention to enhance the child’s quantity and quality of UE movement outside of the clinic. ▪ Because of inconsistencies in the implementation and administration of the various VR programs and technologies, occupational therapy practitioners might require additional training to be able to appropriately administer VR. Training in the specific VR interventions that meet the needs of the occupational therapist’s specific clientele would likely be beneficial. ▪ To achieve the best potential outcomes, VR should be implemented for at least 360 min over the course of 3 wk or more.
Conclusion
When used as a therapeutic intervention, VR, in its many forms, such as robot- and computer-assisted games, has the potential to improve or maintain functional status and UE performance in children with CP. The results of the 21 studies included in this systematic review suggest the benefits VR can provide when used as an intervention for children with CP. VR has the potential to improve UE function and motor performance and gross motor and functional skills and to influence intrinsic factors, such as motivation and participation in occupations. Although moderate to strong evidence exists, further research is needed to clearly determine which type of VR technology results in the most significant improvements over a period of time in children with CP. Studies with larger sample sizes would improve the generalizability of the results of VR-based interventions. A greater number of RCTs would provide the potential to determine the type of VR most applicable and beneficial for use in occupational therapy practice worldwide.
Supplemental Material
Supplementary material for Effectiveness of Virtual Reality for Upper Extremity Function and Motor Performance of Children With Cerebral Palsy: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050374.pdf for Effectiveness of Virtual Reality for Upper Extremity Function and Motor Performance of Children With Cerebral Palsy: A Systematic Review by Juliana Bell, Bonnie Decker, Alicia Eichmann, Carly Palkovich and Chelsea Reji in The American Journal of Occupational Therapy
Footnotes
* Indicates studies included in the systematic review.
Acknowledgments
All authors participated in the data collection and design of the review. The authors declare no conflicts of interest and no financial interests during the creation of this systematic review. This review did not receive any funding or grants. The authors acknowledge the occupational therapy doctorate faculty for their guidance and mentorship as this review was conducted, synthesized, and finalized.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.