
Abstract
This systematic review shows the value of upper extremity task-oriented training as an effective intervention in stroke rehabilitation.
Stroke is one of the leading causes of long-term disability worldwide. Every year, more than 795,000 people in the United States have a stroke (Centers for Disease Control and Prevention, 2023), and around half of stroke survivors experience chronic disability (Tsao et al., 2022). Given that most daily activities, such as feeding, grooming, and dressing, involve the use of the upper extremity (UE), UE disability can undermine a person’s capacity to perform daily activities, consequently decreasing quality of life and self-efficacy (Alsubiheen et al., 2022; Thant et al., 2019). Today, interventions for improving UE function have become a priority in stroke rehabilitation (Almhdawi et al., 2016; Thant et al., 2019).
Task-oriented training (TOT), proposed by Carr and Shepherd (2003), is one therapeutic intervention used in stroke rehabilitation to improve UE motor skills and performance of daily activities in adults with stroke. TOT refers to programs that focus on the massive practice of functional tasks and active participation. However, the definition of functional tasks used in TOT is inconsistent among published studies. Some TOT studies have defined functional tasks as preparatory activities, such as reaching or grasping (Cunningham et al., 2016; Michaelsen et al., 2006), and others have defined it as comprising meaningful real-life activities (i.e., feeding, dressing, handwriting, and using objects with the hand; Israely et al., 2017; Schaefer et al., 2013; B. Simpson et al., 2016). Although the literature supports the general effectiveness of TOT in improving UE recovery (Bosch et al., 2014; Hussain et al., 2022; Timmermans et al., 2010), it also highlights certain limitations. Thus far, no TOT systematic review has focused on one consistent definition of functional tasks to examine the specific effectiveness of TOT, leading to limited implications for TOT in the context of clinical practice.
Meaningful real-life activities are a major intervention tool used in the occupational therapy profession. Based on motor leaning theory (Carr & Shepherd, 2003), the concept of directly practicing an activity that is related to a person’s daily life can not only facilitate long-term retention of a new skill but also help the person transfer the learned skill to daily life, optimizing functional recovery. We believe that understanding the effectiveness of using meaningful real-life activities in TOT approaches will increase their use in therapeutic interventions and help the occupational therapy profession engage in evidence-based practice. Therefore, a systematic review that focuses on TOT using meaningful real-life activities as training tasks is needed.
In this review, the term activity-based TOT refers to TOT that uses meaningful real-life activities as functional tasks; specifically, activity-based TOT is defined as a client-centered, activity-based intervention that focuses on the practice of goal-directed, real-world, context-specific tasks that are meaningful to patients (Almhdawi et al., 2016; Valkenborghs et al., 2017). Our aim was to conduct a systematic review to investigate the effectiveness of activity-based TOT in improving the UE recovery of adults with stroke, including motor function, motor performance, and performance of activities of daily living (ADLs) as outcome measures.
Method
This systematic review was underpinned by the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Moher et al., 2009) to increase methodological rigor and reduce bias. We found no existing review protocol after conducting a preliminary search of the Joanna Briggs Institute Database of Systematic Reviews and Implementation Reports (https://library.sfsu.edu/joanna-briggs-institute-database-systematic-reviews-implementation-reports-2012-2019).
Search Strategy
The strategy and database searches were developed and carried out with the assistance of a health science librarian at New York University, where this research was conducted. A systematic search of three databases (CINAHL Plus, MEDLINE, and PubMed) was conducted to identify for inclusion studies published from June 2012 to December 2022. The search strategy combined the keywords with the U.S. National Library of Medicine’s (2024) Medical Subject Headings (MeSH), and the search was performed using the Boolean operators “AND” and “OR” to combine the search terms and structure the delimitation in the database. Search terms were developed on the basis of the population, intervention, and outcome measures: stroke, task-oriented, task-related, task-specific, upper limb, and upper extremity. The search terms were used first individually and then in combination. Manual searches of the reference list from the included articles were conducted to locate additional articles that may have been missed in the keyword search.
Study Selection
Articles were included according to the following criteria: (1) quantitative studies that reported TOT interventions that incorporated functional activities, real-world daily activities, or both, as the training tasks (i.e., feeding, dressing, or handwriting); (2) studies with participants age ≥18 yr, with a diagnosis of stroke in all phases; (3) studies that focused on evaluating the effects of the TOT interventions in an effort to improve UE motor recovery; (4) at least one outcome measure that included assessments of motor function (e.g., Fugl-Meyer Assessment [FMA] and grip strength), motor performance (e.g., Wolf Motor Function Test [WMFT] and Box and Block Test), or ADL performance (e.g., FIMTM and Modified Barthel Index [MBI]); 1 (5) peer-reviewed journal articles published in English between June 2012 and December 2022; and (6) a study design with an evidence level of 1 to 4 (Oxford Centre for Evidence-Based Medicine, 2009). Studies were excluded on the basis of the following criteria: (1) The study’s interventions provided additional assistance in performing the tasks, such as robotics or functional electric stimulation; (2) interventions were conducted in tandem with other therapies, such as mirror or robotic therapy; and (3) interventions used movement- based exercise in certain joint movements as the training tasks (i.e., reaching and grasping).
Article screening and inclusion determination were managed through Covidence (https://www.covidence.org/), a web-based software platform that enables each reviewer to independently determine inclusion or exclusion at the screening and full article review stages. The abstracts and titles were first screened for relevance according to the inclusion and exclusion criteria. A full-text review was then conducted. Articles were independently screened for inclusion at each stage. In the event of conflicting perspectives with regard to inclusion or exclusion, we reviewed the inclusion and exclusion criteria and arrived at a consensus.
Data Extraction and Appraisal
Research design, population, setting, intervention, outcome measures, and results of the selected studies were extracted from each of the selected articles and listed on a data extraction form (see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot). Data were extracted by the first author (Cheng-Yu Lee) and checked by the second author (Tsu-Hsin Howe). We independently assessed the quality and risk of bias of each selected article. Risk of bias was evaluated using the Cochrane tool for controlled trials (Higgins et al., 2011) and, for single-group studies, a tool developed by the National Heart, Lung, and Blood Institute (2014). The levels of evidence were evaluated using criteria proposed by the Oxford Centre for Evidence-Based Medicine (2009). The criteria were based on the methodological quality of the study design, ranging from Levels 1 to 5. Level 1 is the highest level of evidence, such as randomized controlled trials (RCTs), and 5 is the lowest level, such as an expert opinion without critical appraisal. We reached agreement on the level of evidence and risk of bias.
Strength of Evidence
The strength of evidence was determined on the basis of guidelines created by the U.S. Preventive Services Task Force (2018) and the American Occupational Therapy Association’s (2020) guidelines for systematic reviews. Strong strength of evidence includes ≥2 Level 1b studies (i.e., well designed, well constructed) with consistent results. Moderate strength of evidence includes ≥1 Level 1a or Level 1b study or multiple Level 2a/b or 3a/b studies. Low strength of evidence includes a small number of low-level studies with insufficient evidence to assess effects on outcomes because of a variety of factors, such as a small sample size or poor study design.
Data Synthesis
The studies were organized by intervention setting. Two themes emerged from the literature, and studies were divided accordingly: hospital-based and home-based settings. In each setting, a narrative analysis was used to summarize the data. The results are reported in the following order: study design and evidence level, participant characteristics, intervention characteristics, outcome measures, and effectiveness.
Results
The literature search using the three databases yielded 583 studies. After eliminating duplicates, 326 studies remained. Of those studies, 48 met the criteria for a full-text review. After the full-text review, 32 of these 48 studies were excluded. The excluded studies were those in which TOT was provided in tandem with other interventions (14 studies), studies that provided additional assistance in performing the tasks (13 studies), and studies that used movement-based exercise as the intervention tasks (5 studies). The screening process and results are shown in Figure 1, and the overall risk of bias for each study is reported in Supplemental Table A.2 or A.3.
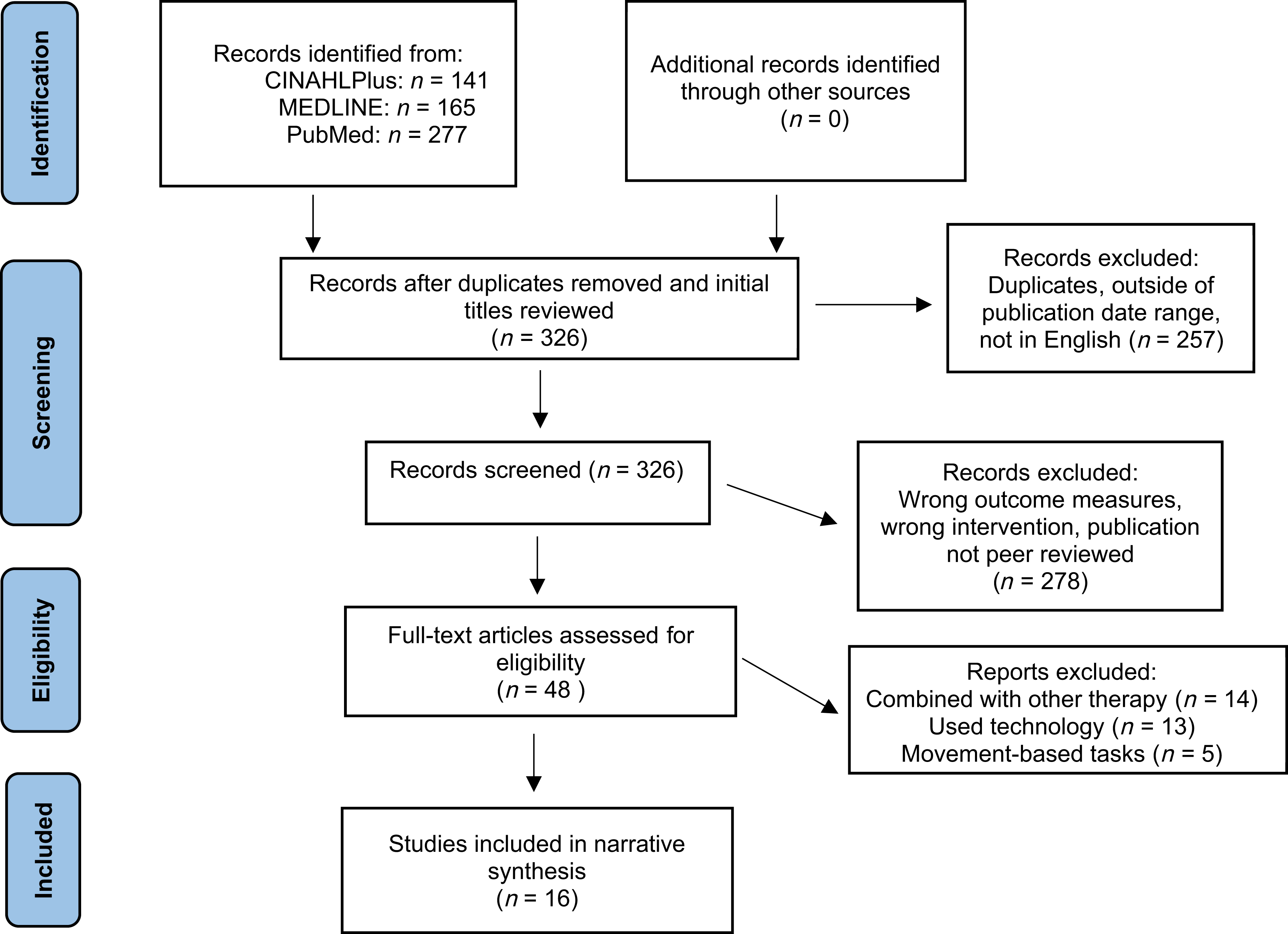
Flow of articles through the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) systematic review process.
Among the 16 selected studies, 8 were rated as yielding Level 1b evidence (Almhdawi et al., 2016; Alsubiheen et al., 2022, Arya et al., 2012; da Silva et al., 2015; Song, 2015; Thant et al., 2019; Winstein et al., 2016; Zaman et al., 2022), 1 was rated as providing Level 2b evidence (Choi, 2022), 5 were rated as providing Level 3b evidence (Rowe & Neville, 2018 ; Schaefer et al., 2013; B. Simpson et al., 2016; L. A. Simpson et al., 2017; Waddell et al., 2014), and the remaining 2 were rated as providing Level 4 evidence (Israely et al., 2017; Park & Yoo, 2015).
TOT as a Hospital-Based Intervention
Study Design and Evidence Level
Twelve studies reported TOT being used as a hospital-based intervention. Six studies were conducted in inpatient settings (Arya et al., 2012; Choi, 2022; Israely et al., 2017; Park & Yoo, 2015; Waddell et al., 2014; Winstein et al., 2016), 3 were conducted in outpatient settings (Almhdawi et al., 2016; Schaefer et al., 2013; Song, 2015), and 3 did not mention the setting (Alsubiheen et al., 2022; Thant et al., 2019 ; Zaman et al., 2022). The effectiveness of hospital-based TOT interventions was supported with strong evidence, including 7 Level 1b RCTs (Almhdawi et al., 2016; Alsubiheen et al., 2022; Arya et al., 2012; Song, 2015; Thant et al., 2019; Winstein et al., 2016; Zaman et al., 2022), 1 Level 2b two-group study (Choi, 2022), and 2 Level 3b studies (Schaefer et al., 2013; Waddell et al., 2014). The remaining 2 studies yielded Level 4 evidence: 1 designed as case report (Israely et al., 2017) and the other as a case series (Park & Yoo, 2015).
Participant Characteristics
Six hundred fifty-three participants were included in the hospital-based TOT intervention studies. The length of time since stroke ranged from 0.3 to 62.1 mo. Participants’ ages ranged from 46 to 77 yr, and sample sizes ranged from 1 to 361. The phases of stroke recovery included subacute (Arya et al., 2012; Choi, 2022; Israely et al., 2017; Thant et al., 2019; Waddell et al., 2014; Winstein et al., 2016) and chronic (Almhdawi et al., 2016; Alsubiheen et al., 2022; Park & Yoo, 2015; Schaefer et al., 2013; Song, 2015). The phases of stroke recovery were categorized on the basis of time since the occurrence of the stroke. The acute phase referred to the initial 7 days after stroke, the subacute phase encompassed the period from 7 days to 6 mo poststroke, and the chronic phase described the period beyond 6 mo after stroke. All the reviewed articles required participants to have a minimal amount of active movement in their affected arm and basic cognitive ability. Two descriptions were used to characterize the minimal amount of active movement in their affected arm: (1) demonstrate an active movement range of 10° to 15° in either the shoulder–elbow or wrist–finger joints, depending on the design of each study’s intervention, and (2) exhibit mild to moderate motor impairment in the UE, as evaluated by movement-based assessments such as the FMA, the Brunnstrom stages of stroke recovery, or the National Institutes of Health Stroke Scale. All included participants showed the cognitive ability to follow directions or a score ≥24 on the Mini-Mental State Examination (MMSE).
Intervention Characteristics
All hospital-based TOT interventions implemented daily activities, such as feeding, dressing, and drinking water, set up with different levels of collaboration between clinicians and participants. Six studies collaborated on goals with the participants and implemented personalized intervention tasks (Almhdawi et al., 2016; Arya et al., 2012; Israely et al., 2017; Thant et al., 2019; Waddell et al., 2014; Winstein et al., 2016), and the remaining 6 studies implemented predetermined tasks (Alsubiheen et al., 2022; Choi, 2022; Park & Yoo, 2015; Schaefer et al., 2013; Song, 2015; Zaman et al., 2022). The intervention intensity varied widely. One study conducted 50 trials/day for 5 days (Schaefer et al., 2013). In most of the studies, the duration of the intervention sessions ranged from 30 min to 1 hr, and the frequency varied from 2×/wk to 5×/wk. The overall duration of the interventions lasted anywhere from 1 to 12 wk. The common shared characteristics among the 12 selected studies were 30 min as the minimum length of a single session and 1 hr as the minimum length of weekly intervention.
Outcome Measures
Outcome measures used to assess the effectiveness of the TOT were identified and sorted into three categories: UE motor function, UE motor performance, and ADL performance. The outcome measures used to assess UE motor function were the FMA (Arya et al., 2012; Israely et al., 2017; Thant et al., 2019; Zaman et al., 2022) and strength test (Almhdawi et al., 2016; Alsubiheen et al., 2022; Waddell et al., 2014). The outcome measures used to assess UE motor performance included the WMFT (Almhdawi et al., 2016; Arya et al., 2012; Thant et al., 2019; Winstein et al., 2016; Zaman et al., 2022), the Action Research Arm Test (Arya et al., 2012; Waddell et al., 2014), the Box and Block test (BBT; Alsubiheen et al., 2022; Song, 2015), the Manual Function Test (Alsubiheen et al., 2022; Choi, 2022; Park & Yoo, 2015), and the Jebsen–Taylor Hand Function Test (Song, 2015). Last, the outcome measures used to assess ADL performance included the FIM (Park & Yoo, 2015; Waddell et al., 2014), Barthel Index (Zaman et al., 2022), MBI (Alsubiheen et al., 2022; Choi, 2022; Song, 2015), and the Motor Activity Log (MAL; Almhdawi et al., 2016; Arya et al., 2012).
Effectiveness of TOT as a Hospital-Based Intervention
Strong evidence supporting hospital-based TOT interventions for improving UE recovery was reported in all three outcome measure categories (Supplemental Table A.1). To be specific, strong evidence supporting the effectiveness of UE motor function and ADL performance, respectively, was reported by 3 RCTs (Arya et al., 2012; Thant et al., 2019; Zaman et al., 2022) and 4 RCTs (Almhdawi et al., 2016; Arya et al., 2012; Song, 2015; Zaman et al., 2022), regardless of interventional tasks, that is, whether they were individualized (Almhdawi et al., 2016; Arya et al., 2012) or predetermined (Song, 2015; Thant et al., 2019; Zaman et al., 2022). Strong evidence showing considerable improvement in UE motor performance was provided by 5 RCTs that compared TOT with traditional rehabilitation therapy (e.g., Bobath neurodevelopmental technique, repetitive movements of certain joints and stretching; Alsubiheen et al., 2022; Arya et al., 2012; Song, 2015; Thant et al., 2019; Zaman et al., 2022). However, Winstein et al. (2016) reported no notable changes in the measure of UE motor performance in their comparisons of TOT with conventional occupational therapy interventions.
TOT as a Home-Based Intervention
Study Design and Evidence Level
Four studies reported TOT interventions in the home setting (da Silva et al., 2015; Rowe & Neville, 2018; B. Simpson et al., 2016; L. A. Simpson et al., 2017). Moderate strength of evidence supported the effectiveness of home-based TOT interventions based on the reports of 1 Level 1b RCT (da Silva et al., 2015) and 3 Level 3b studies that had a pre–post single-group design (Rowe & Neville, 2018; B. Simpson et al., 2016; L. A. Simpson et al., 2017).
Participant Characteristics
Thirty-nine participants were included in the home-based TOT intervention studies. The length of time since stroke ranged from 4.7 mo to 41 mo. Ages ranged from 64.5 to 70.4 yr, and sample sizes ranged from 4 to 20 (da Silva et al., 2015; Rowe & Neville, 2018; B. Simpson et al., 2016; L. A. Simpson et al., 2017). The participants were recruited at the subacute (Rowe & Neville, 2018) and chronic (da Silva et al., 2015; B. Simpson et al., 2016; L. A. Simpson et al., 2017) phases of stroke recovery. Similar to the studies reported in the hospital-based intervention section, all studies conducted in home-based settings required participants to have a minimal amount of active movement and the ability to follow instructions. Two studies further required their participants to be able to identify their intervention goals (Rowe & Neville, 2018; B. Simpson et al., 2016).
Intervention Characteristics
All home-based TOT interventions implemented daily activities. Two studies implemented personalized intervention tasks (Rowe & Neville, 2018; B. Simpson et al., 2016), and the remaining 2 studies implemented predetermined daily activities tasks (da Silva et al., 2015; L. A. Simpson et al., 2017).
Despite the variations in intervention frequency and dosage, several common denominators among the studies were identified. Similar to the hospital-based TOT interventions, the length of a single intervention session for home-based TOT was 30 min at a minimum, the length of weekly intervention was at least 1 hr, and the range of duration was 6 to 8 wk (da Silva et al., 2015; Rowe & Neville, 2018 ; B. Simpson et al., 2016; L. A. Simpson et al., 2017). One study assigned an additional 3-hr self-practice for every week during the home-based TOT intervention (B. Simpson et al., 2016).
Outcome Measures
Three categories of outcomes used to demonstrate the effectiveness of the home-based TOT were identified. In the category of UE motor function, the outcome measures included the FMA (da Silva et al., 2015), shoulder active range of motion (da Silva et al., 2015), accelerometry (Rowe & Neville, 2018), and shoulder and grip strength tests (da Silva et al., 2015; L. A. Simpson et al., 2017). In the category of UE motor performance, the outcome measure was the Test d’Évaluatión des Membres Supérieurs des Personnes Âgées (da Silva et al., 2015). Last, in the ADL performance category, the outcome measures included the Chedoke Arm and Hand Inventory–9 (L. A. Simpson et al., 2017); the MAL (L. A. Simpson et al., 2017); and handwriting performance, including sentence legibility, handwriting speed, and pen control (B. Simpson et al., 2016).
Effectiveness of TOT as a Home-Based Intervention
There was moderate evidence supporting the effectiveness of home-based TOT interventions in improving UE recovery in the categories of UE motor function and UE motor performance (Supplemental Table A.1); specifically, moderate evidence supporting the effectiveness of UE motor function was reported by 1 RCT (da Silva et al., 2015) and 2 Level 3 studies (Rowe & Neville, 2018; L. A. Simpson et al., 2017). These 2 Level 3 studies further supported the sustainability of motor function at the follow-ups (Rowe & Neville, 2018; L. A. Simpson et al., 2017). Moderate evidence supporting the effectiveness of UE motor performance was reported by 1 RCT (da Silva et al., 2015). Inconsistent results were reported with regard to improvements in ADL performance. L. A. Simpson et al. (2017) reported significant improvement in daily activities in their Level 3 study, whereas B. Simpson et al. (2016) reported no change in daily activity outcomes.
Discussion
The aim of this systematic review was to survey and appraise the literature reporting the effectiveness of UE TOT interventions that use meaningful real-life activities as training tasks to improve the UE motor recovery of adults with stroke. On the one hand, we found strong to moderate levels of evidence supporting the effectiveness of activity-based UE TOT interventions; specifically, strong evidence supported the positive effects of activity-based TOT interventions conducted in hospital settings. On the other hand, moderate evidence supported the positive effects of activity-based TOT interventions conducted in home settings. The results of this review not only align with previous studies’ findings that UE TOT can be effective for adults with stroke (Hubbard et al., 2009) but also demonstrate that using meaningful real-life activities as functional tasks can be effective for adults with stroke in different phases.
In this review, we have identified optimal characteristics of participants and TOT doses that were shared by studies that reported the success of TOT interventions regardless of the setting. To be specific, the participants in the activity-based TOT studies with positive outcomes all demonstrated a minimum 10° to 15° active range of motion and had either the basic cognitive ability to follow instructions or an MMSE score ≥24. In terms of the TOT dose, all activity-based TOT interventions with positive outcomes were delivered with a minimum of 30 min for a single TOT session and with at least 1 hr of weekly intervention.
After the onset of stroke, rehabilitation is conducted differently at each recovery phase depending on the neurological improvement (Jung, 2017). Recognizing that adults with stroke in the chronic phase typically experience suboptimal motor recovery compared with those in earlier phases, we conducted a further examination and comparison of the effectiveness of TOT intervention for adults with chronic stroke in both hospital- and home-based settings. On the basis of the results from our review, we observed that strong evidence supporting the positive effectiveness of activity-based TOT interventions for adults with chronic stroke was reported only in hospital settings. The TOT interventions administered in hospitals were reported to be effective in enhancing UE motor recovery, and they require a shorter duration of intervention compared with home-based TOT (Almhdawi et al., 2016; Park & Yoo, 2015; Schaefer et al., 2013; Zaman et al., 2022). Conversely, the effectiveness of TOT interventions in a home-based setting was supported by a smaller body of research and a lower level of evidence. The lack of optimal quality and quantity of evidence supporting home-based TOT may be due to methodological challenges, such as clients’ compliance, control over the intervention environment, and participant recruitment challenges that lead to small sample sizes. Further research on home-based TOT interventions is warranted because optimal interventions for adults in the chronic phase of stroke should be conducted in their most natural environments.
Although most of the reviewed studies indicated that TOT interventions enhanced UE motor recovery for people with stroke, 2 studies reported no noteworthy improvements after their TOT interventions (B. Simpson et al., 2016; Winstein et al., 2016). Rowe and Neville (2018) offered explanations for the nonsignificant results reported by Winstein et al. (2016): They hypothesized that Winstein et al.’s (2016) TOT intervention shared the same component as traditional occupational therapy—both focused on client-centered and meaningful activity-based interventions and resulted in nonsignificant outcomes between the TOT group and the traditional occupational therapy control group, even though both groups showed improvement.
On the basis of Winstein et al.’s (2016) study results and Rowe and Neville’s (2018) explanation, we would like to further propose that interventions that emphasize client-centered and meaningful activities in occupational therapy and TOT interventions could both lead to positive outcomes. However, TOT interventions have the advantage of providing structured protocols that help the client not only focus on a certain meaningful task but also practice it intensively to optimize motor learning.
To investigate the pure intervention effects of TOT interventions, we excluded studies that used TOT in tandem with other types of training. There has been an increase in the number of studies reporting the combined effectiveness of TOT and other treatments, such as electrotherapy, robotic training, or mirror therapy (Bondoc et al., 2018; Jung, 2017; Moon et al., 2021; Schweighofer et al., 2012). However, we believe that before analyzing the combination or synergistic effects of interventions, it is essential to understand their individual effectiveness. With the understanding of the effectiveness of activity-based TOT interventions gained from this review, exploring the effectiveness of TOT in tandem with other interventions should be the next step.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for clinical practitioners of occupational therapy: ▪ Positive outcomes of TOT interventions are likely to be observed for adults with stroke who demonstrate at least 10° to 15° of UE active movement and who can follow instructions or have an MMSE score ≥24. ▪ Successful TOT interventions should include high-repetition practice and goal-directed functional tasks preferably related to basic and instrumental ADLs. ▪ Functional tasks used in TOT interventions could either be customized to the individual’s needs or be predetermined, but need to be at appropriate challenge levels. ▪ The recommended intensity of TOT interventions should be a minimum of 30 min each session, with a total of at least 1 hr of interventions every week for a minimum of 4 wk.
Conclusion
This review found moderate to strong evidence supporting activity-based TOT interventions for improving the UE recovery of adults with stroke; specifically, there was strong evidence for hospital-based TOT interventions and moderate evidence for home-based interventions. Because we examined the effectiveness of activity-based UE TOTs, this review not only shows the value of UE TOT as an effective intervention in stroke rehabilitation but also supports the occupational therapy philosophy of using functional and meaningful activities in practice.
Supplemental Material
Supplementary material for Effectiveness of Activity-Based Task-Oriented Training on Upper Extremity Recovery for Adults With Stroke: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050391.pdf for Effectiveness of Activity-Based Task-Oriented Training on Upper Extremity Recovery for Adults With Stroke: A Systematic Review by Cheng-Yu Lee and Tsu-Hsin Howe in The American Journal of Occupational Therapy
Footnotes
1
FIMTM is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
* Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.