
Abstract
The study findings can help occupational therapy practitioners identify what state funding sources are available to help their clients with intellectual and developmental disabilities access environmental modifications to support community integration, self-determination, and independence.
When home environments are inaccessible, people with intellectual and developmental disabilities (IDDs) have an increased risk of falls, injuries, limitations in activities of daily living, and institutionalization (Greiman et al., 2022). A lack of fit between the person and their environment can make functioning unsafe and physically difficult; it can also increase cognitive demands when performing routine activities in a setting filled with barriers. The Occupational Therapy Practice Framework (4th ed.; American Occupational Therapy Association [AOTA], 2020) details how environmental modifications are a key intervention to explore to support a client’s ability to engage in meaningful occupations. When the physical, social, and sensory environments people with IDDs inhabit are not adequately matched with their needs, people may exhibit behaviors that challenge (BTC; Roos et al., 2022). BTC is used to describe a direct relationship between the context of an environment and the behavior a person is exhibiting (National Institute for Health Care and Excellence, 2015). Historically, “challenging” behaviors frame these as individual characteristics, so interventions have focused on the person (Bradley & Korossy, 2016). However, the term BTC is increasingly being used to acknowledge that behaviors may result from environments that are restrictive and inaccessible, creating frustration for a person with an IDD when performing activities they want or need to do (Roos et al., 2022). In contrast, Tanner et al. (2008) found that older adults reported feeling a greater sense of personal control, self-efficacy, and mastery over routines and daily activities after the implementation of tailored home modifications; importantly, older adults also described positive effects on caregivers, with reduced worry and stress strengthening the quality of their social relationships with caregivers.
The Centers for Medicare & Medicaid Services (CMS) breaks environmental modifications into two categories: (1) home modifications and (2) vehicular modifications. CMS (2019) defines home modifications as those physical adaptations to the private residence of the participant or the participant’s family . . . that are necessary to ensure the health, welfare and safety of the participant or that enable the participant to function with greater independence in the home. (p. 174)
Vehicle modifications are “adaptations or alterations to an automobile or van that is the waiver participant’s primary means of transportation in order to accommodate the special needs of the participant” (p. 174).
Assessing and implementing home and vehicular modifications are clearly within occupational therapy’s scope of practice (AOTA, 2020). Examples of environmental modifications that might be recommended by an occupational therapist could include such things as adaptive equipment, ramps, bathroom modifications, modifications to a vehicle to ensure wheelchair access, adapting the lighting or desk height of a workstation, and many more. Environmental modifications can be transformational for the daily living experiences and quality of life of people with IDDs and their caregivers (Carnemolla & Bridge, 2016). In fact, adults with IDDs, similar to other adults, prefer home environments that support independent functioning and access to social networks and community participation (Friedman, 2020; McConkey et al., 2004). Moreover, research with people with disabilities has found that after the implementation of environmental modifications, both informal and formal care provision decreases, supporting a model of self-determination and autonomy (Carnemolla & Bridge, 2019).
Occupational therapy models of practice provide a conceptual lens through which occupational therapists can examine the relationship between environment and person to understand its impact on occupational performance (Christiansen et al., 2005; Law et al., 1996). In fact, research highlights the need to assess the person–environment fit, rather than just environmental barriers, when making recommendations for environmental modifications, to ensure that the modifications are based on the person’s individualized needs (Iwarsson et al., 2009; Stark et al., 2015). Comprehensive assessments of the safety and accessibility of a person’s home environment are frequently performed by occupational therapists; these are followed by tailored recommendations that involve changes to the usability, physical structure, and layout of the home (Wellecke et al., 2022).
A review of the literature identified strong evidence for the efficacy of community-based occupational therapy interventions, including environmental modifications, for supporting the aging in place of older adults (Brown et al., 2020). In addition, occupational therapists have developed targeted assessments that measure the person–environment fit of a client’s home (Stark et al., 2010), as well as clinical reasoning guidelines to prioritize home modification interventions (Stark et al., 2015). Research examining the need for and impact of environmental modifications to support aging at home for people with IDDs has identified that ongoing assessment of the degree of fit between the person and their physical environment has a positive impact on that person’s safety, autonomy, and independence (Hutchings et al., 2008). Research supports comprehensive environmental modification interventions, including assessing the person’s abilities, establishing occupational goals, developing plans to achieve those goals, and training the person with an IDD and caregiver in how to use environmental supports, are more effective than modification recommendations alone (Stark et al., 2017). These comprehensive assessment and intervention approaches include examining the need for external home environmental modifications, such as automatic doors, accessible parking, and lifts and adaptations to vehicles, to promote social and community participation as well as access to medical care and employment and increased school attendance (Batson et al., 2022; Chandola & Rouxel, 2022).
Despite the evidence for occupational therapy’s role in environmental modifications (Brown et al., 2020) and a growing understanding of the value of establishing a home that environmentally supports and fits a person with an IDD and achieves the goal of long-term, stable community living (Freedman et al., 2014), less is known about how environmental modifications are provided to people with IDDs in Medicaid home- and community-based services (HCBS) waiver–funded programs. Medicaid HCBS-funded programs are service programs for people with IDDs to help them live in their own homes and communities. Unlike acute care, Medicaid HCBS-funded programs include a wide range of wrap-around services, such as personal care and in-home supports; residential habilitation (e.g., group homes); day and employment services; health and professional services; transportation; and specialized medical equipment and assistive technology, including environmental modifications (Friedman, 2023). Because of deinstitutionalization, the preferences of people with IDDs, and the benefits of community living, Medicaid HCBS waivers have become the largest funding source for long-term services and supports (LTSSs) for people with IDDs (Braddock et al., 2017). In fact, 79% of LTSSs for people with IDDs in fiscal year (FY) 2018 was funded by HCBS waivers (CMS, 2020). In FY 2021, $43.2 billion in funding was projected for HCBS for 860,000 people with IDDs (Friedman, 2023).
Although Medicaid HCBS is a critical funding mechanism for people with IDDs, each state in the country has the ability to customize their Medicaid HCBS-funded programs—deciding who will receive services, what services people will receive, and the scope and extent of those services. Decisions regarding HCBS funding often leads to large differences across states and programs as well as disparities in who can access services (Friedman, 2023). Moreover, little is currently known about environmental modification services in the HCBS programs for people with IDDs.
An increased understanding of HCBS funding mechanisms for environmental modifications could assist occupational therapists in making recommendations to clients to support community living. In addition, identifying state programs that have disparate funding for HCBS environmental modification can inform the need for professional advocacy. For example, despite the fact that occupational therapy services are offered within many HCBS programs, many state programs devote limited funding to these services (Friedman & VanPuymbrouck, 2018). This may be due in part to a lack of knowledge about HCBS programs among occupational therapists, resulting in limited professional advocacy for the funding of occupational therapy services within HCBS waivers (Zaffos, 2019). In fact, Zaffos (2019) found that the majority of occupational therapists were lacking in knowledge of HCBS waivers and wanting education on waivers as a funding source for occupational therapy services, as well as information to support legislation and advocacy for occupational therapy funding within these waivers. However, only a limited amount of literature has examined occupational therapy services within HCBS waivers (Friedman & VanPuymbrouck, 2018), and no research exists that is specific to HCBS waivers and environmental modifications. For these reasons, our aim in this study was to examine how environmental modifications are provided in HCBS waivers for people with IDDs. To do this, we examined, using a mixed-methods analysis, FY 2021 Medicaid HCBS 1915(c) waivers from across the United States.
Method
We obtained the Medicaid HCBS 1915(c) waivers from https://www.medicaid.gov/medicaid/section- 1115-demo/demonstration-and-waiver-list/index.html in January 2022. To be included in this study, HCBS waivers needed to be classified as 1915(c), exclusively serve people with any type of IDD (i.e., intellectual disabilities, developmental disabilities, autism), and include FY 2021. Although some states used the state FY (July 1, 2020–June 30, 2021), others used the 2021 calendar year (January 1, 2021–December 31, 2021), or the federal FY (October 1, 2020–September 30, 2021); we use the term FY for consistency. Through this process, we collected 107 HCBS 1915(c) waivers for people with IDDs from 44 states and the District of Columbia (some states have more than one HCBS 1915[c] program for people with IDDs, and some do not have any).
CMS (2019) requires that state Medicaid waivers document the following: CMS assurances and requirements, levels of care, waiver administration and operation, participant access and eligibility, participant services, service planning and delivery, participant direction of services, participant rights, participant safeguards, quality improvement strategies, financial accountability, and cost-neutrality demonstrations. We used the information provided in the Participant Services (Appendix C) and Cost-Neutrality Demonstrations (Appendix J) sections of HCBS waivers for this study.
In the Participant Services section, states list which services they will provide (Appendix C, Subsection C-1: Summary of Services Covered) and include definitions for each of those services (Appendix C, Subsection C-1/C-3: Service Specifications). First, we used these data to determine which waivers provided any type of environmental modification services. (Eight services combined environmental modifications with other forms of assistive technology services; they were excluded from this study because the services could not be differentiated.) Carli Friedman then analyzed the definitions of the environmental modification services using content analysis (Hsieh & Shannon, 2005; Merriam, 2009; Patton, 2002; Zhang & Wildemuth, 2009). Patton (2002) described content analysis as a “qualitative data reduction and sense-making effort that takes a volume of qualitative material and attempts to identify core consistencies and meanings” (p. 453). To do this, Friedman assigned codes to each environmental modification service definition while creating an emerging inductive coding scheme using the constant-comparison method (Glaser, 1992). After all definitions were coded, Friedman returned to the data to confirm alignment of the coding scheme and consistent coding.
After the definitions were coded, we analyzed the cost-neutrality demonstrations data. In the cost- neutrality demonstrations section of waivers (Appendix J, Subsection J-2: Derivation of Estimates), states document how their programs will be cost-neutral compared with institutions; they do this by documenting for each service the total unduplicated participants, total projected spending, projected spending per participant, reimbursement rates, and annual service provision per participant. We used descriptive statistics to examine environmental modification service allocation. While doing so, we also analyzed the fiscal effort dedicated to environmental modifications. Fiscal effort is also one way to control for some state contextual differences to make comparisons across states, specifically, those related to state wealth. Fiscal effort was calculated by dividing the state’s total projected spending on environmental modification services by the state’s personal income in millions.
Results
In FY 2021, 75 waivers (70.09%) from 35 states (77.78%) provided 127 environmental modification services to people with IDDs (some waivers included multiple environmental modification services; see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot). Among the services, 53.54% of environmental modifications (n = 68) were for the home, 29.92% (n = 38) were for vehicles, 14.96% (n = 19) were for both home and vehicles, and 1.57% (n = 2) were for work settings.
Service Definitions
In the service definitions, the most common examples of environmental modifications included in the definitions are presented in Table 1. In addition, 11.02% of environmental modification services (14 of 127 services) mentioned including training for people with IDDs about how to use the modifications.
Service Definitions: Common Examples of Environmental Modifications
The purpose of environmental modifications was most often described as to promote the health, welfare, and safety of people with IDDs (82.68%, n = 105) and to promote the independence of people with IDDs (69.29%, n = 88). Although less common, other purposes of environmental modifications included preventing institutionalization (30.71%, n = 39), promoting community integration (24.41%, n = 31), and decreasing the need of people with IDDs for paid supports (11.02%, n = 14).
In terms of additional requirements, 61.42% of environmental modification services (n = 78) required the need for modifications be documented in a person’s service plan to justify their use, 18.90% (n = 24) required an evaluation first, and 28.35% (n = 36) required prior approval before anything could be purchased. In addition to noting that environmental modification services should be cost-effective (18.90%, n = 24), it was also common for service definitions to note that an HCBS waiver should be the payer of last resort and that funding from Medicaid state plans, or early and periodic screening, diagnoses, and treatment, should be used first (44.88%, n = 57).
The majority of environmental modification services also specified that general improvements to homes or cars, such as cosmetic changes or routine maintenance, were excluded (82.68%, n = 105). Sixty-eight services (53.54%) also excluded modifications that increased the square footage of homes; however, 39 of those services allowed exceptions if the increased square footage was specifically required for a modification (e.g., enlarging a bathroom). In addition, 38 services (29.92%) did not allow modifications to be conducted in homes and vehicles that were not owned by the person with an IDD or their family, although four of those services allowed exceptions with approval of the home’s landlord. Finally, slightly fewer than one-third of environmental modification services (29.13%, n = 37) explicitly mentioned excluding the purchase or lease of new vehicles as part of the service.
Participants
In FY 2021, HCBS waivers projected providing a total of 12,671 people with IDDs with environmental modification services out of 861,000 people with IDDs receiving HCBS support (1.47%; Table 2). This ranged per service line from 1 participant (seven different services) to 2,015 (Minnesota Developmental Disabilities Waiver’s [MN.0061.R07.19] Consumer Directed Community Supports: Environmental Modifications and Provisions service), with the average service line projecting to serve 99.77 participants (SD = 257.43). The states that provided environmental modification services to the most people with IDDs were Minnesota (n = 2,532), New Mexico (n = 2,194), and Ohio (n = 1,605; Table 3). The states that provided environmental modification services to the greatest proportion of their IDD HCBS waiver participants were New Mexico (24.20%), Minnesota (10.57%), and New Jersey (8.33%).
Environmental Modifications
Environmental Modification Services by State
Note. H = home modifications; HCBS = home- and community-based services; NS = not specified; V = vehicle modifications; W = work modifications.
Exceptions allowed. bSee https://www.medicaid.gov/medicaid/section-1115-demo/demonstration-and-waiver-list/index.html for specific waiver descriptions.
Of the 12,671 people with IDDs projected to receive environmental modifications, 70.86% (n = 8,979) were eligible to receive services that provided only home modifications, 20.67% (n = 2,619) were eligible to receive services that provided only vehicle modifications, 8.41% (n = 1,066) were eligible to receive services that provided both home and vehicle modifications, and 0.06% (n = 7) were eligible to receive services that provided only work modifications.
Total Projected Spending
In FY 2021, $68.83 million was projected for environmental modification services (0.16% of all FY 2021 projected spending). On average, waivers projected spending $0.54 million per service line (SD = $1.19 million), ranging from $18.72 per service line (Indiana Community Integration and Habilitation Waiver’s [IN.0378.R04.02] Environmental Modifications– Equipment/Assessment/Inspection service) to $5.92 million per service line (MN.0061.R07.19’s Consumer Directed Community Supports: Environmental Modifications and Provisions service). New Mexico ($10.97 million), Minnesota ($9.21 million), and New Jersey ($7.68 million) projected spending the most on environmental modification services. The states that allocated the largest portion of their IDD HCBS spending on environmental modification services were New Jersey (2.65%), New Hampshire (0.57%), and Minnesota (0.52%).
Of the $68.83 million projected for environmental modifications, 67.66% ($46.57 million) was directed toward services that provided only home modifications, 23.88% ($16.43 million) for services that provided only vehicle modifications, 8.44% ($5.81 million) for services that provided both home and vehicle modifications, and 0.02% ($14,811) for services that provided work modifications.
In FY 2021, the national fiscal effort for environmental modification services was $3.77/$1 million of personal income. The states with the highest fiscal efforts were New Jersey ($112.42), Minnesota ($26.25), and New Hampshire ($17.39).
Average Spending Per Participant
The average annual spending per participant on environmental modification services in FY 2021 was $6,297 (SD = $5,040; Figure 1). Average annual spending per participant on environmental modification services ranged from $13.50 (Pennsylvania Consolidated Waiver’s [PA.0147.R06.11] Home Accessibility Adaptations service) to $35,925 (Hawaii HCB Services for People With IDD Waiver’s [HI.0013.R08.00] Vehicle Modifications service). The states with the highest average spending per participant were New York ($16,605), Maine ($11,600), and North Dakota ($9,686).
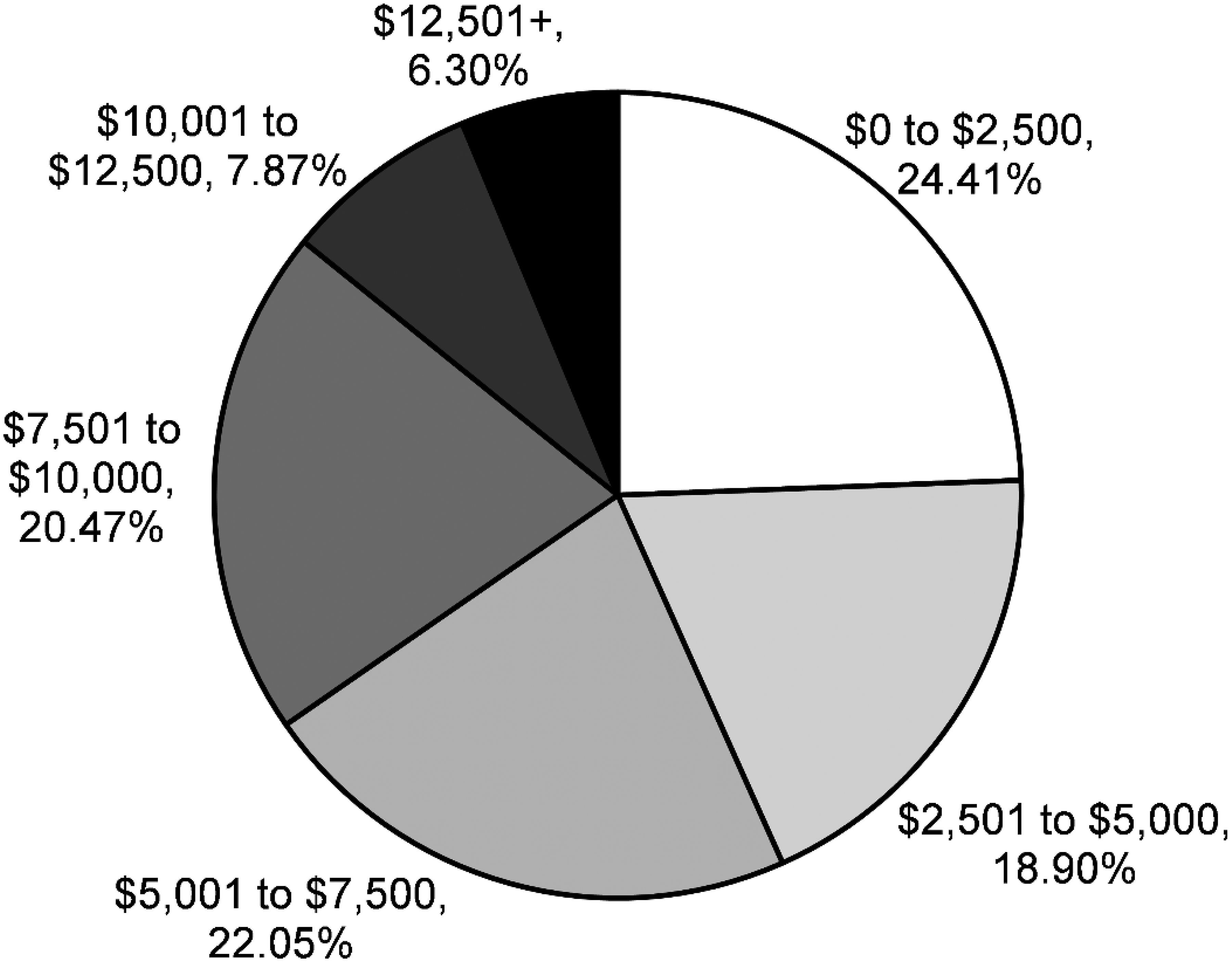
Average spending per participant on environmental modifications.
The average spending per person for home- modification–only services was $6,411 (SD = $5,276), $7,021 (SD = $5,290) for vehicle-modification—only services, $4,744 (SD = $3,316) for services that offered both home and vehicle modifications, and $3,459 (SD = $4,432) for work modification services.
Reimbursement Rates
Environmental modification services were reimbursed by item/unit (n = 121, 95.28%), hour (n = 2, 1.57%), and year (n = 3, 2.36%). Of those environmental modification service lines provided by item/unit, the average reimbursement rate for these services was $5,116 per item/unit (SD = $4,180), ranging from $1.00 per item/unit (five services) to $20,945 an item/unit (Pennsylvania OBRA Waiver’s [PA.0235.R05.09] Vehicle Accessibility Adaptations service). The average hourly rate was $3.00 (SD = $2.83), ranging from $1.00/hr (Illinois Support Waiver for Children and Young Adults with Developmental Disabilities’ [IL.0464.R02.09] Home Accessibility Modifications service) to $5.00/hr (Ohio Self Empowered Life Funding Waiver’s [OH.0877.R02.06] Worksite Accessibility service). The average yearly rate was $5,573 (SD = $4,026), ranging from $1,718/yr (Louisiana New Opportunities Waiver’s [LA.0401.R03.12] Environmental Accessibility Adaptation Services) to $9,750/yr (New Jersey Community Care Waiver’s [NJ.0031.R06.00] Environmental Modifications service).
Annual Service Provision
The item/unit services provided an average of 529.66 items/units (SD = 3,480.57) of environmental modification services per participant per year, on average, ranging from 1 item/unit a year (84 services) to 35,925 items/units a year (HI.0013.R08.00’s Vehicle Modifications service). The services that reimbursed hourly provided an average of 3.50 hr (SD = 3.54) of environmental modification services per participant per year, ranging from 1 hr/yr (IL.0464.R02.09’s Home Accessibility Modifications service) to 6 hr/year (OH.0877.R02.06’s Worksite Accessibility service). Yearly rate services provided an average of environmental modification services 1.67×/yr (SD = 1.15) per person, ranging from 1×/yr (two services) to 3×/yr (LA.0401.R03.12’s Environmental Accessibility Adaptation Services).
Discussion
Most people with IDDs want to live in their own home (Friedman, 2020); however, only 1% of the current housing stock in the United States has even the most basic accessibility features: no-step entry, single-floor living, wide halls and doorways, electric controls and switches, and lever-style door and faucet handles versus knobs (Joint Center for Housing Studies of Harvard University, 2018; Keglovits & Stark, 2020). Most states have HCBS 1915(c) waivers that provide an opportunity for a person with an IDD who requires an institutional level of long-term care to instead live in a home in the community. However, in this study we found that not all HCBS programs for people with IDDs provide environmental modification services (70%); in addition, only 1.5% of the 860,000 people with IDDs receiving HCBS waivers in FY 2021 were projected to receive environmental modification services (Friedman, 2023). This is troubling given the lack of accessible housing, the preference on the part of people with IDDs for community living, a growing preference for aging in place, and concerns stemming from coronavirus disease 2019 (COVID-19) about the real health risks of institutional living and congregate living (Chidambaram, 2022; Friedman, 2020; Joint Center for Housing Studies of Harvard University, 2018; Landes et al., 2020; Szanton et al., 2014). In fact, a recent scoping review (Washington et al., 2021) highlighted the growing need for attending to the concerns of adults with IDDs and specifically called for “occupational therapy to move forward as a profession” (p. 8) to address the many environmental barriers that exist to support aging in place for adults with IDDs.
Although only a small proportion of people with IDDs are projected to receive environmental modification services, those who do may be able to benefit immensely given that evidence from other populations indicates that environmental modifications can support staying in a home, improving quality of life, and reducing caregiver burden (Hutchings et al., 2008; Stark et al., 2010). Research has noted that when occupational therapists provide environmental modifications to the homes of older adults with disabilities, considerable improvements occur in outcomes related to occupational performance as well as satisfaction with that performance (Stark, 2004). In fact, the most frequent modifications described in HCBS waivers in this study—changes to the physical features of the home, including building ramps or lifts, widening doorways, and bathroom modifications—align with evidence that changes like these increase independence while simultaneously decrease reliance on support services for people with mobility disabilities (Greiman et al., 2022). Moreover, these results appear to have a sustained impact: A study of older adult recipients of occupational therapy home modification services reported their daily activity performance to be significantly improved even 2 yr postmodification (Stark et al., 2009). Importantly, environmental modifications support aging in place for older adults and support discharge to the community, rather than an institution, for people with disabilities when hospitalizations occur (Wellecke et al., 2022). In fact, the average projected cost per person for environmental modifications in our study in FY 2021 ($6,297) was just a fraction of the average cost of institutional living for people with IDDs ($140,210 in 2019; Residential Information Services Project, University of Minnesota, 2022), suggesting that environmental modifications can contribute to the cost-effectiveness of HCBS waivers.
In their waivers, states noted that the primary reason for environmental modifications was to promote the health, welfare, and safety of people with IDDs. Although less attention was drawn to the need to decrease paid supports in definitions of environmental modification services, it is important to note that for decades there has been a shortage of direct support professionals (DSPs) that has resulted in unmet needs and has reduced the quality of life of people with IDDs (Friedman, 2018, 2021; Winters et al., 2021). For example, people with IDDs who experience DSP turnover are two times less likely to have maximum access to their physical environments at home, at work, and in the community (Friedman, 2018). The COVID-19 pandemic has further increased DSP shortages (ANCOR Foundation & United Cerebral Palsy, 2021); so too will the aging of caregivers, given that most people with IDDs live with unpaid caregivers who are older (Braddock et al., 2017). Reducing the demand for care providers through environmental modifications can simultaneously address many of the other reasons for these modifications, including a reduction in the likelihood that institutionalization may occur because of a lack of service providers, as well as promote the independence of people with IDD. As such, proactively incorporating home modifications now may achieve many intersecting long-term goals of HCBS waivers to allow people to live and thrive in their homes and communities.
Despite research identifying how critical transportation is in the lives of people with IDD (Batson et al., 2022), this study found that environmental modifications specifically for vehicles were less common than those for homes. Having the ability to use a family vehicle to travel to and from home, school, work, and medical care is an integral part of daily living for people with IDDs, especially those with complex medical needs (Batson et al., 2022). One of the most common challenges reported by families to access even basic health care needs, such as an eye exam for their family member with an IDD, is difficulty with transportation (Li et al., 2015). Moreover, transportation is one of the largest barriers to community integration for people with IDDs (Stock et al., 2013). In fact, the Bureau of Transportation Statistics (2003) estimated that more than 500,000 people with disabilities do not leave their homes as a result of a lack of available, accessible public transportation. As such, vehicle modifications that allow people with IDDs to get out of the home, interact with social connections, and manage health are extremely beneficial. Attending to both home and vehicular modifications allows a higher quality of life through engagement and participation in society for people with IDDs and their families (Hutchinson et al., 2020).
Only two services provided workplace accessibility adaptations. This may be due to people with IDDs receiving workplace accommodations through other means, such as supported employment services through HCBS waivers, vocational rehabilitation funding, and adaptations provided by their employers as required by the Americans with Disabilities Act of 1990 (Pub. L. 101-336). People with IDDs want to work, and are capable of working, in integrated employment settings. There is an Employment First movement (https://www.dol.gov/agencies/odep/initiatives/employment-first) that aims to prioritize integrated employment for people with IDDs, and the HCBS Settings Rule (CMS, 2014) encourages integrated, person-centered employment opportunities. However, HCBS programs for people with IDDs still heavily favor funding day habilitation services over supported employment (Butterworth et al., 2015; Friedman, 2023). This may also contribute to the lack of stand-alone workplace modification services we noted in this study.
A critical finding of this study was that only 11% of environmental modification service definitions mentioned training for people with IDDs in how to use the modifications. This finding is troubling because the research is clear that training in the use of environmental modifications is an established best practice approach performed by occupational therapists (Stark et al., 2009). Without training for the people who will be using them, environmental modifications become less effective in changing their everyday use (Stark et al., 2017). Environmental modifications funded by HCBS waivers should require training interventions to ensure that people with IDDs and their caregivers are competent in their use to ensure that the modifications are able to support the goal of long-term, stable community living.
Finally, in this study we also found a wide variance in the projected allocation of environmental modifications across states, HCBS waivers, and services. For example, even among those states that provided environmental modifications, only an estimated 0.1% to 24.2% of the waiver participants with IDDs in that state were projected to receive these services. Average projected per-person spending ranged by state from $602 to $16,605. Fiscal effort ranged from $0.13 to $112.42 per $1 million of personal income. These are just a few of the wide discrepancies we found. Although HCBS waivers have been an important positive development for people with IDDs in the United States, there is considerable variability across programs that can create barriers to access and use of environmental modifications for people with IDDs.
Limitations
Several limitations should be noted when interpreting this study’s findings. Medicaid HCBS 1915(c) waiver data are projections made to the federal government, rather than actual utilization data. However, previous research has found them to be relatively accurate proxies because they are designed on the basis of previous years’ use data (Rizzolo et al., 2013). We excluded eight services from this study—one from Arkansas, one from Kansas, one from Kentucky, and five from Texas—because they combined environmental modifications with other forms of assistive technology, and differentiation could not be determined. Only Friedman coded the service definitions. The aim of this study was to examine how environmental modifications were allocated in HCBS waivers: We did not examine the effectiveness of these services or whether they improved people’s outcomes. We also did not examine whether or how people with IDDs received environmental modifications from other funding sources. For example, millions of people with IDDs do not receive formal services and are instead supported by family caregivers (Braddock et al., 2017), which may influence their experiences with environmental modifications. We believe both areas would be fruitful avenues for future research.
Implications for Occupational Therapy Practice, Advocacy, and Research
In the past 10 yr, there has been a surge in occupational therapy research focusing on supporting aging in place for people with disabilities and older adults that includes attending to environmental modifications and the distinct value of occupational therapy (Stark et al., 2017; Struckmeyer & Pickens, 2016; Washington et al., 2021). Evidence suggests that occupational therapy practitioners are well suited to perform assessments as well as to provide modification recommendations and training in the use of modifications to homeowners as a best practice approach to successful aging in place (Horowitz et al., 2013; Tynan et al., 2023). It may be that a better understanding of Medicaid HCBS waiver data focusing on environmental modifications for people with IDDs can inform areas of practice for occupational therapy practitioners to support people with IDDs with living, as well as aging, in the community rather than in institutions. In addition, this study can be an impetus for occupational therapists to examine their own state’s HCBS waivers to ensure that environmental modifications, both home and vehicular, are a covered service. As this study identified, in many states some HCBS waivers include environmental modifications, whereas others do not. Identifying gaps in coverage can be used by occupational therapists to advocate for their inclusion. More specifically, the findings of this study encourage occupational therapists to do the following: ▪ Determine what funding sources are available in their state to assist individual clients with IDDs in accessing environmental modifications. This could include understanding what services are provided (i.e., home, vehicle, or work), what the current rates are for each service, and identifying and connecting with state-approved providers to prescribe environmental modification recommendations on the basis of individual client needs. ▪ Because of disparities in coverage across states, raise awareness at state and national levels to target advocacy efforts toward state Medicaid agencies, calling for HCBS waivers to increase the availability of and funding for both home and vehicular environmental modifications as well as the use of occupational therapy practitioners in assessments and intervention delivery. ▪ Provide foundational data for needs assessment research on the role of occupational therapy in HCBS environmental modification programing. ▪ Examine the impact of HCBS environmental modifications across states to identify differences in the participation, satisfaction, and quality of life of people with IDDs, to inform best practice approaches for occupational therapy services.
Conclusion
In FY 2021, 70% of HCBS waivers for people with IDDs projected spending $69 million on environmental modifications for 12,700 people. This represents <0.2% of total HCBS program IDD-related projected spending and <1.5% of people with IDDs with HCBS waivers receiving these services. Environmental modifications for people with IDDs align with Medicaid HCBS’s aims to promote the community integration, self-determination, and independence (CMS, 2014). As such, given that in this study very few people with IDDs were projected to receive environmental modifications, we believe advocacy is needed to expand the availability of these services in HCBS waivers. Moreover, an increased understanding and use of HCBS program–funded environmental modifications by occupational therapists may be an “effective solution to facilitate participation in everyday living” and support achieving AOTA’s (2017) Vision 2025 to “maximize health, well-being, and quality of life” for people with IDDs (p. 1). Occupational therapy’s distinct value— facilitating participation and environmental modifications—can and should be used to achieve optimal participation in everyday occupations for the clients we serve.
Supplemental Material
Supplementary material for Environmental Modifications for People With Intellectual and Developmental Disabilities: A Policy Analysis of Medicaid Home- and Community-Based Services
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050393.pdf for Environmental Modifications for People With Intellectual and Developmental Disabilities: A Policy Analysis of Medicaid Home- and Community-Based Services by Carli Friedman and Laura VanPuymbrouck in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.