
Abstract
This pilot study highlights how the Comprehensive Operating Room Ergonomics program can effectively address a projected surgeon shortage by 2025 due to work-related musculoskeletal disorders, which affect surgeons’ health and job continuity.
Life-altering diagnoses of significant work-related musculoskeletal disorders (WMSDs) among procedural-based physicians, such as surgeons and those in interventional medical specialties, have risen dramatically over the past decade (Voss et al., 2017). The Occupational Safety and Health Administration (OSHA; 2020) defines WMSDs as overexposure to manual materials handling, such as pushing, pulling, lifting, and twisting, while performing a task in an unfavorable body posture. More than 80% of surgeons experience work-related musculoskeletal pain, strain, and fatigue during and after surgeries, and 30% report multisite occupational injuries that include the shoulder, neck, and upper and lower back (Alleblas et al., 2017; Dalager, Søgaard, et al., 2019; Epstein et al., 2018; Sergesketter et al., 2019; Voss et al., 2017). According to Coleman Wood et al. (2018), this rising trend of WMSDs and work-related risk factors among surgeons, specifically in the area of minimally invasive surgery, is expected to continue.
Risk Factors
During an operation, surgeons often place their bodies in biomechanically disadvantaged positions while performing repetitive motions for a sustained period, putting their neck, back, and upper extremities at risk for both acute and chronic injuries (Auerbach et al., 2011; Janki et al., 2017; Voss et al., 2017). In their systematic review, Alleblas et al. (2017) found that risk factors such as case load, length of surgery time, sustained awkward postures, repetitive motions for long periods of time, chronic pain, and fatigue contributed to the increase in WMSDs. These risk factors have been shown to affect dexterity, range of motion, proprioception, grip strength, and decision-making among surgeons (Epstein et al., 2019). Sergesketter et al. (2019) performed a retrospective review using Bureau of Labor Statistics Survey of Injuries and Illness data from 1992 to 2016, reporting that 10,078 physicians had nonfatal occupational injuries. Women ages 35 to 55 yr reported most of these injuries. Back pain and strain injuries were among the highest reported (Sergesketter et al., 2019). According to Voss et al. (2017), female surgeons are more likely to report acute neck and shoulder pain immediately, whereas male surgeons often delay reporting such injuries, possibly because of work and cultural stigma and a lack of awareness of acute symptoms. This results in a higher incidence of chronic WMSDs among male surgeons. The observed gender differences suggest that variations in pain perception and self-awareness, as well as the influence of workplace culture, exist between male and female surgeons.
Most surgeons lack ergonomic knowledge and problem-solving strategies to reduce their occupational demands (Dalager, Højmark, et al., 2019). The Centers for Disease Control and Prevention have noted that WMSDs have a higher economic impact than any other physical ailment, directly and indirectly costing $45 to 54 billion in the United States alone. WMSDs are the number one health care employment disability claim compared with other disease groups (Epstein et al., 2018; Park et al., 2017). These claims are associated with increasing absentee rates and loss of overall productivity among health care workers, including surgeons (Epstein et al., 2018), of whom at least 80% report a WMSD during their career (Alleblas et al., 2017; Dalager, Søgaard, et al., 2019; Epstein et al., 2018; Sergesketter et al., 2019; Voss et al., 2017). The rising trend of WMSD diagnoses and work-related risk factors among surgeons, specifically among those performing laparoscopic surgery, is expected to continue (Coleman Wood et al., 2018).
Surgeons may knowingly or unknowingly adopt awkward and biomechanically disadvantaged postures while performing repetitive surgical tasks for extended periods. Holding surgical instruments in static poses, excessive neck extension and flexion to look at monitors or into the surgical field, and prolonged standing with trunk flexion and rotation all contribute to increased physical demands on the surgeon. These physical demands include muscle strain and fatigue, increasing the surgeon’s risk for WMSD (Auerbach et al., 2011 ; Janki et al., 2017; Voss et al., 2017). Chrouser et al. (2018, 2024) have indicated that physical, emotional, and environmental stressors directly affect surgeons’ attention and decision-making, which raises concerns about their cognitive function and performance outcomes, with potential implications for patient care and medical errors. A lack of ergonomic knowledge, awareness, and problem-solving strategies adversely affects surgeons’ occupational performance and quality of life (Dalager, Højmark, et al., 2019).
Identifying Gaps in the Research
There are no evidence-based, comprehensive holistic ergonomic intervention protocols using preventive strategies to help reduce WMSD and risk factors among surgeons (Dalager et al., 2020; Epstein et al., 2018; Franasiak, 2013; Voss et al., 2017). Numerous studies have shown a strong demand for ergonomic interventions to address surgeons’ physical and cognitive well-being, evolving surgical technology, natural aging of the population, and high burnout rates (Epstein et al., 2018; Jackson et al., 2018 ; Sergesketter et al., 2019). Unfortunately, this issue is not limited to trained surgeons because there is no standardized formal ergonomics education at the surgical trainee level, which is when ergonomics habits during surgery are formed (Epstein et al., 2018). Currently, the Surgical Council on Resident Education (n.d.) provides recommended surgical ergonomics guidelines for residency programs.
Current Surgical Ergonomic Intervention Strategies
The most promising interventions in the literature are intraoperative “microbreaks,” proven to increase overall physical and cognitive performance without affecting the intraoperative surgical flow among surgeons (Abdelall et al., 2018; Coleman Wood et al., 2018; Park et al., 2017). Other researched interventions include guidelines for operating room (OR) equipment setup (monitors, tables, foot pedals, stools, lighting), ergonomic devices (floor mats, support stockings, and supportive furniture), ergonomically designed medical technology equipment (exoskeleton), education (online workshops), and cognitive and behavioral modification strategies (body awareness; Dalager, Højmark, et al., 2019; Epstein et al., 2018). Although interventions to improve surgical ergonomics show promise, research on their long-term benefits and sustainability is limited (Sweeney et al., 2021).
To address a gap in the surgical literature and the need for ergonomic improvements in surgery, the Comprehensive Operating Room Ergonomics (CORE) program tailored to surgeons was developed. This program addresses a variety of factors that affect surgeons’ professional and personal lives, including habits, roles, routines, and performance patterns and skills, both inside and outside the OR. With consultation from an occupational therapist with more than 40 years experience (Penelope Moyers Cleveland), and an occupational therapist (Pamela Hess) designed this multimodal, client-centered educational program. The development and study of this program will be used to support future grant proposals focusing on ergonomic risk factors among laparoscopic surgeons (see the “Method” section). Our study aimed to evaluate the CORE program’s design, implementation, and effectiveness as an evidence-based ergonomic intervention. The central research question was, “Does the CORE program designed to reduce perceived symptoms of WMSDs and the physical and mental demands of surgeons’ work have potential for improving their work performance and quality of life?”
Method
This was a 14-wk pilot study that used a mixed-methods embedded design in which the quantitative strand was embedded within the qualitative strand to examine the potential of the CORE program as an ergonomic intervention for laparoscopic surgeons to prevent WMSDs. The pilot study was designed with oversight from a research team (Dimitrios Athanasiadis, Nicole Kissane Lee, Sara Monfared, Dimitrios Stefanidis), who plan to use data from the pilot study as information for future grant proposals. The second author (Athanasiadis) guided and reviewed the quantitative data from the pilot study and ran the statistical analyses. The third and sixth authors (Lee and Stefanidis) facilitated and reviewed the OR observations. The fourth and fifth authors (Monfared and Cleveland) provided input into the development of the CORE program. Cleveland specifically provided oversight of the program’s development to reflect the principles of occupational therapy and also provided consultation on collecting and interpreting the qualitative strand and the mixing or triangulation of the qualitative and quantitative data.
Participants
Surgeon participation was voluntary, and informed consent was obtained according to institutional review board approval. Six participants were recruited to form a convenience sample; the small sample size reflects that the primary purpose of the pilot study was not hypothesis testing but to determine the themes regarding the participants’ experience with the CORE program and its potential as an intervention. The quantitative data provided additional evidence to support the themes emerging from the qualitative data.
The participants were board-certified general surgeons specializing in minimally invasive surgery. Surgeons who performed only open surgery were not included because their practice could have introduced confounding factors in assessing the impact of minimally invasive techniques on the surgeons themselves. Because of the small sample size, group demographics were not reported so as to not identify participants.
Data Collection
Qualitative Data
Semistructured interview.
The questions in the semistructured interview were modeled after the Canadian Occupational Performance Measure as a framework to help facilitate conversation and gain insight into the surgeon’s lifestyle, occupational performance patterns, roles, routines, and other meaningful activities (Law et al., 2014). Before the interview questions, participants were educated on the role of occupational therapy in applying ergonomic principles to all their daily occupations, including their surgery occupation. Qualitative data documented in field notes from the semistructured interviews helped to establish participants’ long- and short-term goals for the CORE program.
Field notes.
The purpose of the field notes was to document the surgeons’ interactions and responses to all components of the CORE program. These field notes were taken during program interactions and were then expanded after the interaction was completed (Phillippi & Lauderdale, 2018).
OR observations.
OR observations were conducted before and after the ergonomics intervention for each participant. Intraoperative observations consisted of gathering data about table heights in relation to the lead surgeon and other OR staff; monitoring the surgeon’s positions; noting surgery start and end times; observing the layout of surgical instrument; determining room lighting; discerning the number of microbreaks taken; observing potential safety hazards; and noting adaptive equipment, such as step stools, platforms, and OR standing mats. There were 12 baseline observations (two observations for each of the 6 participants), and 20 postimplementation observations (at least two for each participant), all involving laparoscopic procedures. Robotic operations were also observed (one during baseline observations and two during postimplementation observations). These observations were documented with field notes and photographs that provided insight into the surgeons’ occupational demands and their ability to transfer newfound ergonomics knowledge to their working environment.
Quantitative Data
The occupational therapist (Hess) assessed the WMSD risk factors for each surgeon using a postural assessment (Hough & Nel, 2019a, 2019b); the Physical Discomfort Survey and Wellness Questionnaire, which was developed for this pilot study; and the Rapid Upper Limb Assessment (RULA; Kiger & Varpio, 2020).
Postural assessment.
This assessment was chosen because according to Hough and Nel (2019a, 2019b), good posture is the foundation of effective and efficient biomechanics when engaging in daily activities. Surgeons consistently position their bodies at awkward angles, putting them at a biomechanical disadvantage during the surgical experience. Postural deficits could contribute to a surgeon’s physical pain and discomfort, potentially affecting their occupational performance. The assessment involved photographing the surgeon in the coronal (front and back) and sagittal (right and left) standing positions with the Posture Screen Mobile® application (Szucs & Brown, 2018). According to Szucs and Brown (2018), this application is a reliable method of assessing posture across raters.
Using the posture photographs, the occupational therapist performed a visual analysis of the photos of each surgeon using the Anatomy Trains body reading method to identify structural asymmetries and patterns that may affect the surgeon’s functional performance (Myers, 2014). The results of the postural assessment inspired the design of the surgeon’s ergonomics intervention. Unaddressed postural deficits put surgeons at higher risk of WMSDs and burnout, ultimately affecting patient care and safety (Hough & Nel, 2019a, 2019b; Wells et al., 2019). The information gained was shared with each participant at an individual follow-up consultation session to increase body awareness, identify common asymmetries, and give credibility to the recommended individualized corrective therapeutic exercise program and ergonomic adaptations in the OR.
Physical Discomfort Survey and Wellness Questionnaire.
This measurement tool was created by adapting several sources, such as the Self-reporting Pain and Discomfort Survey (Beurskens et al., 2000; Huang et al., 2000; Trejo et al., 2006); the Mindful Attention Awareness Scale (Brown & Ryan, 2003), which measures one’s perceived mindfulness and situational awareness; and the Five Facets Mindfulness Questionnaire (Baer et al., 2006), which assesses the conceptualization of mindfulness. The Physical Discomfort Survey and Wellness Questionnaire was used with each surgeon before and after observed surgical procedures to measure perceived bodily pain and discomfort, physical and mental fatigue, and ergonomic strategies used. The two-part questionnaire includes 22 presurgical procedure items and 28 postsurgical procedure item measuring specific bodily pain and discomfort areas, self-perceived behaviors, attention, focus, fatigue, ergonomic strategies, and surgical case workload, using a combination of Likert-scale, dichotomous scale (yes–no), and open-ended questions. It was administered longitudinally over 4 wk before and after each OR case to capture any physical and behavioral changes of the surgeon, such as everyday life activities, roles, habits, and routines. Pain and discomfort for each body region were rated on a Likert-type scale ranging from 0 (no discomfort at all) to 10 (worst imaginable discomfort), and perceived behaviors (irritability), executive cognitive function (wandering thoughts, attention), other bodily discomfort (stiffness, numbness, heart rate, tremors, headache), and fatigue were scored using a scale of no, slight, and substantial. A postsurgical assessment measured the surgeon’s ability to translate and incorporate ergonomics strategies and techniques into the OR using a yes–no scoring scale. The total score for each surgeon was calculated by summing the responses.
RULA.
The RULA was used to measured the pre- to postintervention change in the participant’s working posture during tasks (McAtamney & Corlett, 1993) and to quantify each participating surgeon’s WMSD risk acuity level during their surgical experiences. The RULA assesses workload and force of the upper limbs and trunk and involves the neck, shoulders, elbows, forearms, wrists, and upper and lower body (Shin & Park, 2019). A score is given for each body region, based on the observed and photographed postures, and musculoskeletal risk factors are then determined using the grand score, which ranges from no risk (1–2), indicating that no environmental change is needed, to very high risk (≥7), indicating that immediate change is needed (Craven et al., 2013). The final RULA score is relative and indicates WMSD risk at the level of high-risk tasks that require further analysis and potential ergonomic intervention. It is not an absolute score.
Intervention Design
The development and implementation of the CORE program was based on several theoretical models, the Person–Environment–Occupation–Performance (PEOP) model (Christiansen et al., 2011), intervention mapping (Dalager, Højmark, et al., 2019), and The Six Disciplines of Breakthrough Learning (Pollock et al., 2015). The PEOP model is a dynamic client-centered model focusing on the influences and transactions among the person, their occupation, the environment, and their performance (Christiansen et al., 2011). The reciprocal interaction between the person and the environment influences their occupational performance outcomes, roles, and routines.
Intervention mapping is a practical approach to health promotion in various occupational settings to predict any change in the process to drive implementation (Dalager, Højmark, et al., 2019). Pollock et al. (2015) developed a learning model to drive behavioral change to achieve performance outcomes related to an individual’s capabilities, environmental influences, and ability to transfer and apply the information learned. This learning model includes the following steps: (1) Define the problem, (2) design the complete experience, (3) deliver for application, (4) drive learning transfer, (5) deploy performance support, and (6) document results.
Blending these theoretical models, we used a unique six-step model to support the design and implementation of a novel ergonomics intervention for surgeons. As show in Figure 1, the CORE Intervention Framework model includes six steps with supporting subtasks to effectively deliver the CORE program’s overarching goals for desired outcomes. The occupational therapists (Hess and Cleveland) designed the model, and Hess then used the resulting CORE Intervention Framework model to address ergonomic and wellness deficits in the OR and enhance the surgeons’ occupational engagement and participation in daily life in the least restrictive environment. The CORE Intervention Framework model involves four components: education, physical well-being, context and environment, and mindfulness.
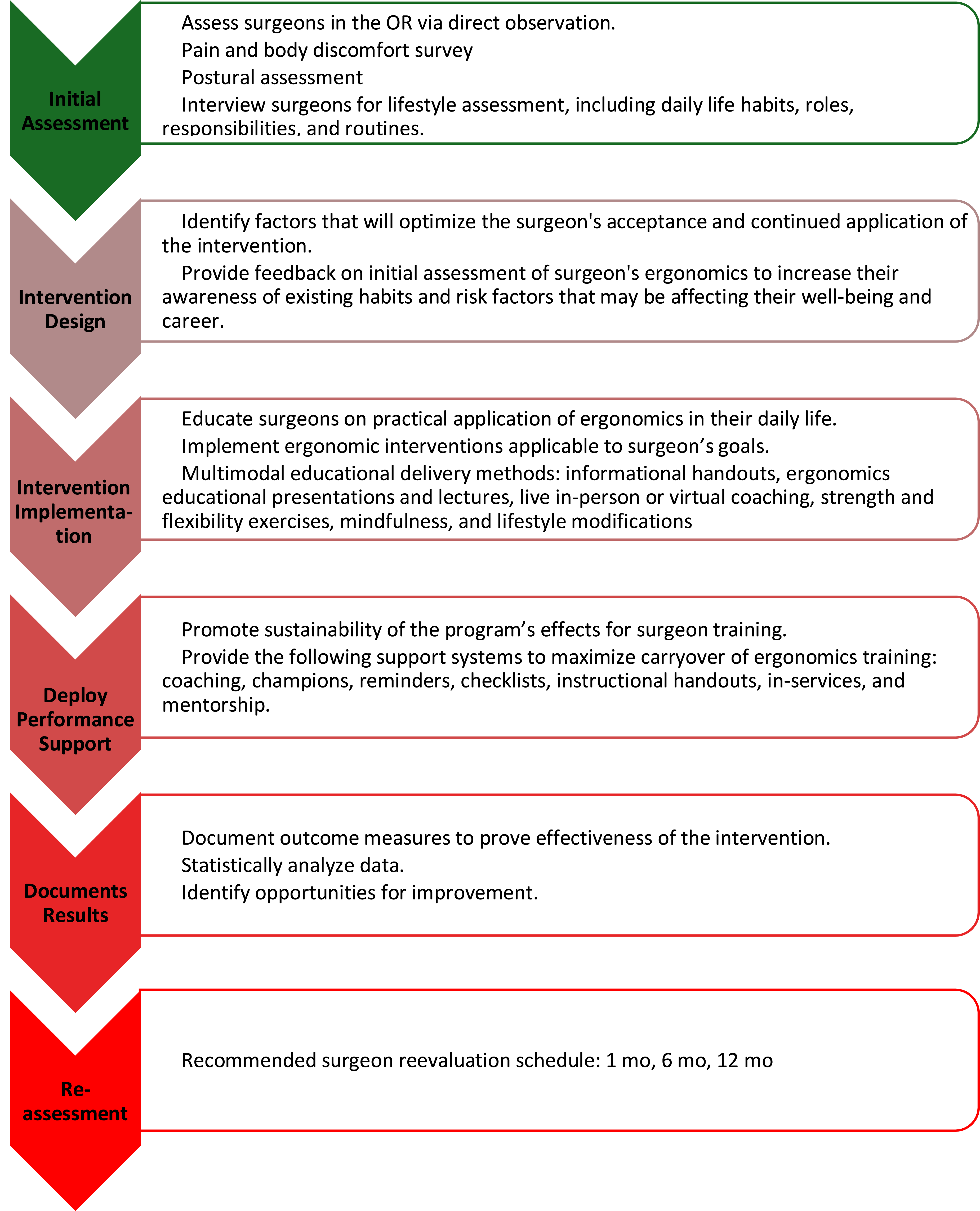
CORE for surgeons; an intervention mapping model.
The focus of the CORE program involved educating surgeons about ergonomics and the role of occupational therapy. Physical well-being aspects of the CORE program included postural assessment, regular vision screening by an optometrist or ophthalmologist, and involvement in a pre–, intra–, and post–surgical procedure exercise program. The context and environment intervention of the CORE program focused on the surgeons’ working and everyday life environments, such as office setup; driving positions; holding a child, for those surgeons who were new parents; and standing at the OR table or performing other daily tasks. Last, a mindfulness component was included because of the increased level of stress surgeons experience daily. Mindfulness interventions included diaphragmatic breathing exercises, sleep hygiene, and self-efficacy activities, such as performing a body scan and recognizing when the body needs to take short breaks during busy workdays.
The CORE program used a holistic and client- centered approach to reflect best-practice strategies that optimize the fit of the task to the surgeon. Skilled occupational therapy services, such as activity analysis, goal setting, and environmental modifications, were provided to address various physical and cognitive performance challenges that were potentially affecting the surgeons’ overall occupational performance. In addition to the individualized intervention sessions, the occupational therapist offered the participants supplemental ergonomics education. For example, Hess provided an ergonomics training session at a monthly medical conference attended by all study participants.
For the CORE program, a presurgical procedure ergonomics time-out checklist rooted in surgical ergonomics principles was used before each surgical experience (Miller et al., 2012; OSHA, 2020; van Det et al., 2009). Athanasiadis, Lee, and Stefanidis reviewed and validated this checklist through quality improvement plan–do–study–act cycles with Hess before their surgical cases (Institute for Healthcare Improvement, n.d.). The purpose of the checklist was to ensure OR safety and a reduction in WMSD risk factors. The ergonomics time-out includes a five-item checklist designed to be completed by the surgeon or OR staff (see Table 1).
Preprocedure Ergonomic Time-Out Checklist
Note. OR = operating room.
Procedures
The procedures for implementing the CORE program involved the occupational therapist preparing in advance for each surgeon’s experience in the program, identifying learning goals for each surgeon, and noting any foreseeable barriers that would affect knowledge transfer, such as lack of insight into and awareness of their operative and everyday postures. The surgeons met with the occupational therapist weekly at various times because of the surgeon’s OR and clinic schedules. Individual meetings were held in either the OR or an office setting, and the surgeon received education and training on postural corrective exercises, OR environment design, adaptive strategies to support optimal posture both in and out of the OR, and identification and establishment of new routines and habits for their daily lives to maximize the carryover of learned ergonomic and wellness information.
Data Analysis
Data analysis involved a mixed-methods triangulation approach in which the quantitative data supported the themes inductively derived from the qualitative data (Creswell & Plano Clark, 2017).
Qualitative Analysis
Qualitative analysis involved thematic analysis according to Boyatzis (1998) and Braun and Clarke (2013) and consisted of six recursive steps: (1) familiarizing ourselves with the data, (2) generating initial inductive codes (basic segment or element of the raw data), (3) searching for themes (noting the codes frequently mentioned), (4) reviewing themes (incorporating additional codes into themes and subthemes), (5) defining and naming themes (finalizing names and definitions of the themes that are brief and descriptive), and (6) producing the report (substantiating themes with data extracts).
Determining the rigor or trustworthiness of the qualitative analysis included enhancement of credibility through both member checking with the surgeons regarding the themes and peer examination of the analysis process by Cleveland regarding coding, reviewing themes, and naming and defining themes. Transferability was enhanced by collecting data at a variety of times for each surgeon to capture their total experience with the CORE program. Cleveland also conducted dependability and confirmability audits during meetings initiated by Hess throughout the data analysis process. Dependability was determined when Cleveland examined the consistency of the codes and the development of themes according to Hess’s decisions. The data were coded and recorded, and themes were revised. Confirmability was determined when Cleveland followed the audit trail of the data and the decisions made about the data analysis to arrive at similar conclusions regarding the meaning of the data. Triangulation of field notes and OR observations strengthened both the confirmability and dependability of the data.
Quantitative Analysis
Age and years of experience as a surgeon, number of cases for each surgeon, and RULA score were treated as continuous variables. A mixed-effects analysis of the RULA scores was undertaken before and after the ergonomic intervention while accounting for the fixed effects of age, gender, and surgeons’ years of experience. A p < .05 was considered significant. Data analysis was performed with IBM SPSS Statistics (Version 26).
Wiley and Rapp (2019) described the procedure for a linear mixed-effects model for small-n designs with repeated measures. These researchers applied the mixed-effects model to a sample size of 5 with six fixed effects. According to Pinelis et al. (2018), sample sizes of 10 and fewer can attain sufficient power when the minimum effect worth detecting is large and when greater risk for a Type 1 error is acceptable, such as in a pilot study. Caution is needed, however, when there are fewer observations, such as the two data points for the RULA, and when there is more than one fixed effect. Consequently, the quantitative data were treated as additional support for the qualitative themes.
Mixing the Data
Mixing of the qualitative and quantitative components occurred at multiple stages of the pilot study, starting with the design decisions based on the study’s previously described frameworks (Creswell & Plano Clark, 2017). Mixing also occurred during data collection when both the quantitative and the qualitative strands led to the collection of additional qualitative data (Creswell & Plano Clark, 2017). Finally, the interpretation of the results was mixed, with the qualitative themes supported by the quantitative data.
Results
Six surgeons (three women and three men) ranging in age from 32 to 46 yr participated in this pilot study. Surgeons who performed robotic surgeries had an average 5 yr experience. Laparoscopic surgery experience ranged from 6 to 17 yr. Three of the participants performed both robotic and laparoscopic surgeries; the other 3 performed only laparoscopic surgeries. On average, each surgeon spent 2 days per week in the OR (M = 3 cases/day and 17–20 hr/wk operative time). Each surgeon spent approximately 2 days per week in the clinic. For male and female participants, respectively, average height was 180.3 cm and 166.7 cm; average weight, 81.5 kg and 64.8 kg; average body mass index, 25.2 and 23.6; and average years of surgical experience, 10.0 yr and 11.7 yr.
The research team used a triangulation approach in which five themes were extrapolated from the qualitative and quantitative data analyses to support the design and potential for implementation of an ergonomics program for surgeons. Not every theme had both quantitative and qualitative data. Some themes were qualitative in nature. Triangulation enhanced the credibility of the pilot study, integrating all data from multiple sources and using constant comparison of inductively derived coding and themes (Krefting, 1991). Careful examination of the quantitative data further supported the qualitative themes. The themes identified were postural alignment, areas of commonly reported physical pain or discomfort, setup of the OR environment, surgical ergonomics training, and ergonomics in everyday life (see Table 2).
Themes and Subthemes of the Pilot Study’s Qualitative and Quantitative Data Analysis
Theme 1: Postural Alignment
Each surgeon participated in a postural assessment that determined asymmetries from the individual’s plumb line. These asymmetries are reported in Table 3. Postural photographs of the participants in the sagittal plane were compared, demonstrating that all but one surgeon presented with a swayback posture. Similar postural patterns were revealed despite the surgeons’ different years of surgical experience. The participant with the fewest years of surgical experience (6 yr) showed mild asymmetries in the sagittal and frontal planes compared with the participant with 17 yr of experience, who demonstrated more severe asymmetries (see Figures A.1 and A.2 in the Appendix). The relative flexibility principle posits that when one link in the body’s kinetic chain weakens or destabilizes, another area compensates with altered movement patterns to achieve the task, especially when the original movement is suboptimal or imprecise (Blanch, 2004; Sahrmann, 1998). Therefore, when a surgeon deviates from their optimal posture, bodily stress, tension, and pain are produced within the body that may affect their ability to perform functional tasks related to their job or activities of daily living (ADLs; see Figures 2 and 3).
Posture Asymmetries
The RULA was used intraoperatively, both pre- and postintervention, to measure changes in WMSD risks associated with the participants’ working postures and the physical demands of the surgical tasks (McAtamney & Corlett, 1993). The baseline RULA scores were analyzed using a mixed-effects data analysis model and demonstrated a mean value of 5.0 (SD = 1.1, 95% confidence interval [CI] [4.378, 5.622]). Postintervention, RULA scores revealed a decreased mean value of 4.0 (SD = 1.3, 95% CI [3.430, 4.570]). This change indicates a significant effect of the intervention, as evidenced by a statistically significant (F[1, 6] = 8.517, p = .03).
Furthermore, there was a median effect size of .408, which indicates a moderate effect. The effect size augments the p value by providing a more comprehensive understanding of the intervention’s potential impact, extending beyond statistical significance, strengthening the practical implications, and reinforcing the relevance of the study’s hypothesis and the efficacy of the CORE program.
Theme 2: Commonly Reported Areas of Physical Pain or Discomfort
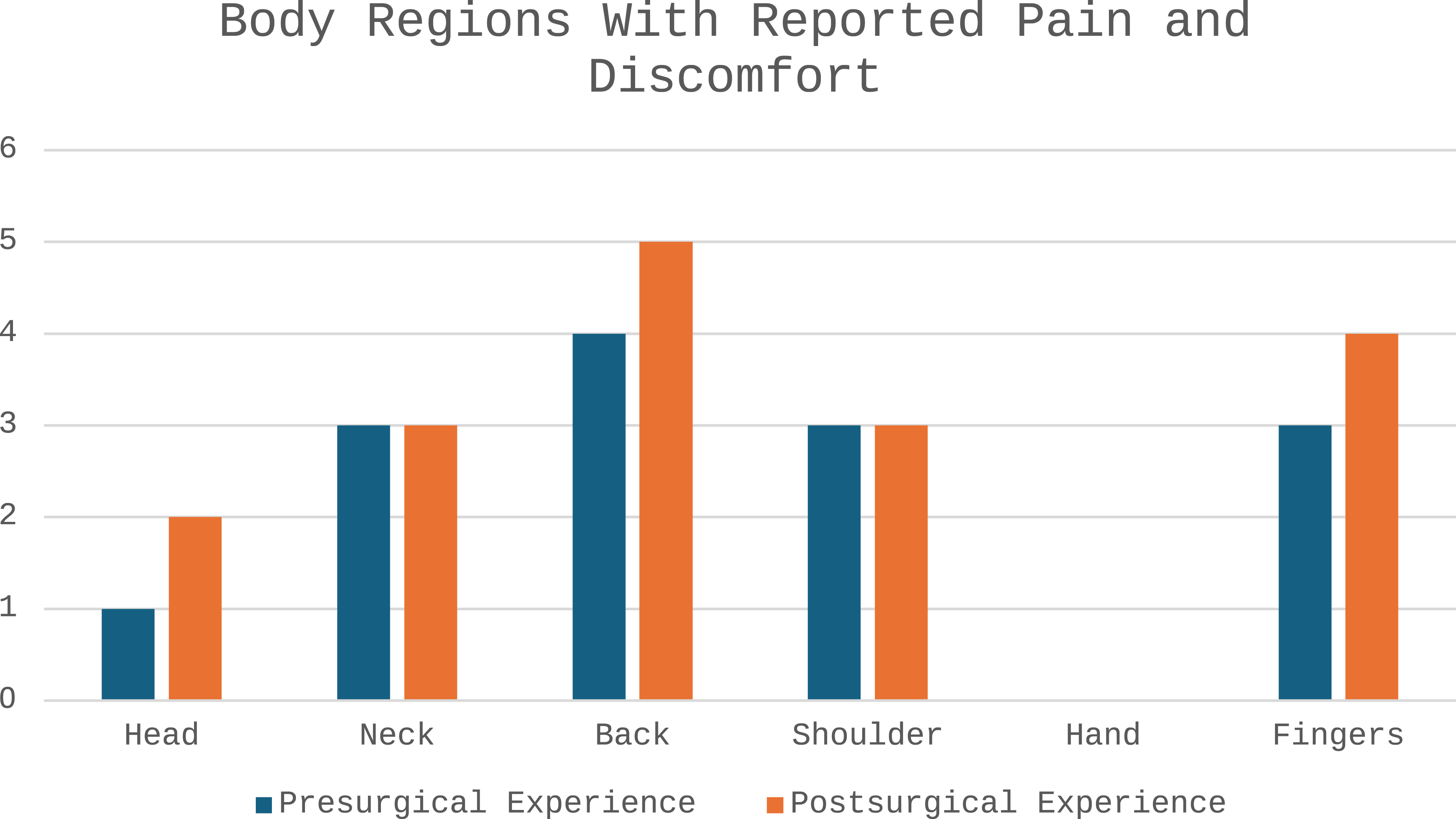
Participants completed a pre- and postsurgical experience Physical Discomfort Survey and Wellness Questionnaire after each OR observation. On the basis of the 12 observed minimally invasive surgeries, the neck, back, shoulders, and fingers were the body areas in which surgeons reported most experiencing pain and discomfort either before or after surgery (see Figure 2). These body regions, as reflected in the literature, are the most common areas in which surgeons experience discomfort and pain (Athanasiadis et al., 2021; Dalager et al., 2020; Stucky et al., 2018).
Participants’ reported pain and discomfort from the surgical experience
Participants reported experiencing various musculoskeletal issues, such as pain in the upper back and neck during prolonged operations; constant tightness and pain in the upper trapezius muscles; discomfort in the right shoulder, elbow, and wrist; discomfort in the left upper extremity when holding the laparoscopic camera for extended periods; and slight numbness and tingling in the fingers and thumb. Data gathered from the participants’ self-reported responses to the Physical Discomfort Survey and Wellness Questionnaire indicate no change for the neck and shoulder region pre- and postsurgical experience; however, results for head, back, and fingers did change, indicating increased pain and discomfort. Although participants felt bodily discomfort while performing surgery, they still pushed through the pain because of the perceived cultural norm and contextual demands.
Theme 3: Setup of the OR Environment
The setup of an OR ideally needs to promote workflow and safety so that the surgeon and other health care staff can perform their tasks and responsibilities efficiently. The OR is a challenging environment because of the equipment and instruments required, multiple cables and lines, and the number of staff working in a confined space while maintaining patient access (Shultz et al., 2019). Before the ergonomics intervention, Hess observed that most participants did not take the time to adjust OR tables or monitors, scan the environment for any safety hazards, or set up other related equipment and instruments for work efficiency. The following examples are derived from Hess’s field notes during intraoperative observations: Surgeon requested table height adjustment during the case; monitors were not adjusted properly, creating neck extension in the surgeon; and safety concerns were observed in the OR, for example, a cord wrapped around a surgeon’s leg. After the ergonomics intervention sessions, surgeons began to demonstrate increased awareness of the OR environment setup before and during the surgical experience. After the CORE intervention and education, Hess observed participants self-initiating the ergonomics time-out preprocedure protocol. Observations included surgeons adjusting bed height and monitors before surgery; adjusting monitors during surgery with minimal verbal cuing from Hess; one surgeon asking for a step stool to accommodate height differences; and surgeons educating residents on proper monitor height before starting the case.
Theme 4: Surgical Ergonomics Training
The lack of prior OR ergonomics knowledge was quite evident among participants; 1 participant stated that the only ergonomics advice given during residency was to “keep your nose, navel, and toes lined up when operating.” All participants expressed that they would have benefited from ergonomics education during residency training. Additionally, each participant expressed barriers that affected their ability to make a behavior or habit change in relation to ergonomics and their wellness. These barriers included time, motivation, and height differences. Time was the most common barrier among surgeons because of their unpredictable schedules, both professional and personal. Three participants reported they started off doing the recommended exercise program, but, as 1 noted, “after about a week due to my schedule and feeling fatigued after a long day of work, I failed to continue.” These findings emphasize the importance of establishing realistic routines and habits to support carryover of ergonomic training and knowledge translation among participants. During the semistructured interviews, the participants and Hess explored possible solutions to overcome these barriers. Participants suggested solutions, such as access to asynchronous exercise and educational videos, virtual coaching sessions with an occupational therapist, and an annual workshop or retreat.
Theme 5: Ergonomics in Everyday Life
The research team learned through the semistructured interviews that the participating surgeons were replicating awkward postures from the OR in ADLs outside the OR. For instance, 1 surgeon reported that while cooking, they tend to hold their child on one side of their body, resulting in a lateral shift of their pelvis. This pelvic posture mirrors foot pedal use during surgery, contributing to the bodily pain and discomfort experienced by the surgeon. Hess observed all surgeons using technological devices to perform nonoperative tasks, such as texting on smartphones with excessive cervical flexion and head-forward posture while repeatedly moving the thumbs, similar to when they looked down into the surgical field and manipulated the laparoscopic instruments in the OR with their thumbs and fingers. These data indicate potential interdisciplinary opportunities for occupational therapy practitioners to educate surgeons on practical and adaptive ergonomic strategies that can be integrated into daily activities, potentially improving their quality of life.
The coronavirus pandemic represented a unique outlier in this study. Although the collection of observational and postural data had been completed before the pandemic, the remaining qualitative data collection, such as the surgeon’s final semistructured interview session and an educational webinar on office ergonomics, was redirected to an online format.
Discussion
The CORE program targets the significant musculoskeletal and occupational performance challenges faced by surgeons during laparoscopic surgery, such as prolonged static postures and repetitive movements. A vital CORE program component involves providing individualized ergonomics interventions tailored to each surgeon’s needs during operations and outside of the OR. Our pilot study was designed to develop and assess the potential of this evidence-based ergonomics intervention, leveraging the Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association [AOTA], 2020) to address these risks effectively. Early findings suggest that our approach not only enhances surgical performance but also mitigates the risk of musculoskeletal injuries, demonstrating the viability of our innovative intervention in promoting surgeon health and well-being.
Consistent with existing literature, our preintervention findings highlight a significant imbalance between surgeons’ work and occupational demands and their capacity to perform tasks requiring repetitive movements and static holds for prolonged periods in awkward postures, heightening the risk of WMSDs (Alleblas et al., 2017). The occupational demands of a surgeon often exceed most individuals’ average available work capacity; however, the culture among surgeons is to push through relentlessly, even if it causes harm to their own physical and mental health (Wells et al., 2019). To date, no holistic ergonomic wellness and prevention program that comprehensively addresses this occupational imbalance exists (Coleman Wood et al., 2018; Dalager, Højmark, et al., 2019 ; Dalager, Søgaard, et al., 2019; Franasiak et al., 2013; Park et al., 2017; Voss et al., 2017). We tailored the CORE program specifically to surgeons by drawing parallels from a study on nursing professionals by Marshall et al. (2018), demonstrating the effectiveness of a comprehensive intervention approach in reducing WMSD risk factors through body mechanics training, job shadowing, exercise programs, and primary preventive measures. We aimed to help reduce WMSD risk factors and enhance overall well-being and career longevity by adopting a whole-person approach. Our approach integrates physical, psychosocial, and environmental considerations to optimize surgeons’ engagement in daunting surgical tasks, daily activities, and meaningful roles and responsibilities.
We used qualitative and quantitative data to further support our pilot study’s design and implementation of our ergonomics program for surgeons. Through qualitative analysis, we identified five key themes: (1) postural alignment, (2) areas of commonly reported physical pain or discomfort, (3) setup of the OR environment, (4) surgical ergonomics training, and (5) ergonomics in everyday life. These themes highlight the multifaceted challenges surgeons face in maintaining ergonomic practices in and out of the OR. Our quantitative data identified a significant estimated effect through the change in RULA scores from pre- to postintervention, demonstrating knowledge translation and awareness of ergonomics strategies among the participating surgeons by a decrease in the occupational demands in the OR. Intraoperative constraints presented challenges, such as the contextual confines related to the sterile field, surgical equipment and instrument design, and hospital resources (Abdelall et al., 2018; Cha et al., 2020). Hess provided surgical ergonomics education and training, emphasizing practical intraoperative adaptations and strategies, ergonomic recommendations (i.e., stepstools, supportive shoes and socks, standing mats), and modifications for daily life activities. These interventions were designed to counteract the surgeons’ occupational deprivations and enhance their overall quality of life.
The preintervention assessments in our pilot study highlight a finding worth mentioning. All the participating surgeons demonstrated a tendency to a swayback posture. The swayback posture, characterized by an anterior shift of the pelvis and flattening of the lumbar spine, creates an imbalance between the musculoskeletal and nervous systems, potentially affecting a surgeon’s occupational performance and engagement in their work tasks and other meaningful activities (Shin et al., 2023). Such deviations place undue stress on the body and contribute to mental and cognitive load, potentially impairing surgical precision and outcomes (Chrouser et al., 2018). This observation warrants future investigation and subsequent research.
In our pilot study, surgeons consistently reported experiencing upper back, neck, and shoulder pain, a finding that aligns with the existing literature (Stucky et al., 2018). These symptoms emphasize the need for a holistic ergonomics and wellness approach in the surgical environment. Such an approach should account for factors that include the surgeon’s gender, the ergonomics of surgical instruments in terms of size and design, the length and intricacy of surgical procedures, and the physical characteristics of both the patient and the surgeon (Bellini et al., 2022; Hislop et al., 2023; Mesiti & Yeo, 2023; Wong et al., 2022). Additionally, specific attention needs to be given to the importance of the setup of the OR environment (i.e., table and monitor height) and optimal instrumentation use and fit, particularly in minimally invasive surgery. Ideally, surgeons performing minimally invasive surgery should work with shoulders abducted <30°, elbows bent 90–120° with forearms in neutral, a 60° angle between the two laparoscopic instruments, and a table height of 70% to 80% of the surgeon’s elbow height to facilitate a mechanical advantage and reduce musculoskeletal strain (Tetteh et al., 2023). Incorporating the OR ergonomics time-out protocol mentioned in our study’s methods before surgery is one potential means of improving the surgical working environment. Despite the inherent challenges of surgical ergonomics, our study reveals that the CORE program can increase surgeons’ postural awareness in the OR and in their daily life activities, potentially mitigating WMSD risk factors.
Our pilot study is unique in its holistic nature because the CORE program addresses the surgeon’s lifestyle outside the OR as an essential component of the intervention process. We identified a general need for surgeons to increase their awareness of ergonomics in their everyday tasks, roles, and other responsibilities outside the OR walls. It may be that surgeons’ posture and poor biomechanics when performing surgery were subsequently repeated when they engaged in their ADLs, putting them more at risk for WMSDs (Epstein et al., 2018). Examples of postural imbalance from the OR repeated during daily life activities included a surgeon holding a young child on one side of the body (i.e., hip), creating a lateral shift in the pelvis and spine, which is similar to a surgeon shifting weight for a period to manage the foot pedal during an operation. Another example is when a surgeon texts on their smartphone with a forward flexed head and neck position for an extended period using repetitive thumb and digit movement patterns, which is similar to surgical procedures when the table height or monitor is not adjusted correctly and when manipulating laparoscopic instruments (Bharal et al., 2023; Sanders & Morse, 2005).
Our pilot study further supports the need for a formal standardized ergonomics curriculum for surgical trainees and OR staff. The CORE program may help decrease barriers such as lack of knowledge and awareness, cultural and behavioral factors in surgery, OR environment design, resource constraints, physical and cognitive demands, and personal or client factors that limit surgeons’ ability to participate in their meaningful occupations. Ergonomic deficits that go unaddressed will continue to put surgeons at a higher risk for WMSDs and burnout, ultimately affecting patient care and safety (Chrouser et al., 2024).
Because of the promising results of this pilot program, we are currently working on implementing the CORE program with our surgical residents alongside their established introduction to the fundamentals of the laparoscopic surgery program. As presented in this study, novel curricula derived from CORE are being developed to teach surgical interns proper OR ergonomics at the outset of their careers, hoping to instill healthy ergonomic habits. A successful resident-based ergonomics and wellness program could have a significant impact on the health and well-being of the surgical workforce.
Limitations
Like most studies, our study is not without limitations. Hess was primarily responsible for program design, data collection, and analysis, thereby creating researcher bias. Researcher bias was limited by the different roles of the research team members in developing the CORE program and in reviewing and analyzing data, particularly in establishing rigor for the qualitative analysis. Our sample included a small number of surgeons, which is appropriate for a pilot study as well as for a design that emphasized qualitative data. Additionally, we included several observations per surgeon to improve the dependability of the data interpretations through the triangulation of multiple experiences. We also embedded the quantitative data to support the qualitative themes rather than interpreting these results separately.
No residents were included in the convenience sample; thus, our results are not transferable to the residents’ ergonomic risk improvement, even though the literature suggests they share similar ergonomic profiles (Athanasiadis et al., 2021). We focused only on laparoscopic general surgery procedures, but the effect of other surgical procedures on surgeons’ WMSDs should be studied. Finally, because of the COVID-19 pandemic, in-person surgeon intervention modalities were reduced by 4 wk, resulting in the early conclusion of the study. Once COVID-related quarantines were initiated, delivery methods for this program were primarily anchored in online and virtual ergonomics training sessions.
Implications for Occupational Therapy Practice
The CORE program for surgeons directly supports AOTA’s (2017) Vision 2025 as an opportunity to promote population health, well-being, and quality of life. The role of occupational therapy practitioners is to identify performance barriers within person, environment, and task (AOTA, 2020). The role of a surgeon is to perform operative procedures using highly skilled techniques to treat a patient’s medical condition and improve the patient’s quality of life. In Greek, the definition of surgery is “hand work.” Mary Reilly (1962) once said, “Man, through the use of his hands, as they are energized by mind and will, can influence the state of his own health” (p. 2). The irony of this quote is that occupational therapists and surgeons believe that what they do with their hands helps restore and heal others. A surgeon’s role directly affects patient care and outcome measures. The physical and mental demands that influence a surgeon’s life put them more at risk for WMSDs and other health conditions. An occupational therapy–based ergonomics program for surgeons can help decrease or eliminate barriers that inhibit a surgeon’s physical and cognitive occupational performance. This pilot study helped to narrow the research gap by developing and implementing the CORE program for surgeons. Additionally, it creates a platform for the occupational therapy profession to cultivate interdisciplinary relationships among occupational therapists and surgeons in an emerging practice area, ergonomics and population health.
Conclusion
Surgeons’ vulnerability to WMSDs should be targeted with appropriate formal ergonomic interventions to reduce their injury risk profile and elongate their careers. Therefore, given the current ergonomic needs in surgery, an occupational therapy practitioner is qualified to provide skilled therapeutic services to reduce WMSD risk factors and injuries among surgeons. Our findings show that a holistic occupational therapy approach is essential to forming the fundamental and theoretical foundation for how occupational therapists and occupational scientists understand the intricacies of how surgeons engage in meaningful occupations both at work and in their personal lives. Future studies should investigate the retention of these improvements and implement interventions such as the CORE program with a larger sample of surgeons, including residents, from various specialties.