
Abstract
This study confirmed that the Flow State Scale for Rehabilitation Tasks questionnaire is reliable and valid for measuring the flow experience of patients after (sub)acute stroke.
Flow can be described as a subjective state that people report when they are completely involved in an activity, feeling pleasure, happiness, satisfaction, and enjoyment (Abuhamdeh, 2020; Csikszentmihalyi, 1975, 2014; Nakamura & Csikszentmihalyi, 2009). The concept of flow became a key element for the theory of optimal experience (Biasutti, 2011), and it is defined by nine characteristics: challenge–skill balance (i.e., balance between the challenge represented by the activity and personal skills), action–awareness merging (i.e., involvement in the task), clear goals (i.e., clear idea of what needs to be accomplished), unambiguous feedback (i.e., clear and immediate feedback), concentration on the task at hand (i.e., complete focus on the task), sense of control (i.e., clear feeling of being in control), loss of self-consciousness (i.e., not being concerned about something, focus only on the activity), distorted sense of time (i.e., altered perception of time, either sped up or slowed down), and autotelic experience (i.e., perception of the activity as intrinsically rewarding; Csikszentmihalyi, 1975).
Flow experience has increasingly been measured in the physical and cognitive rehabilitation settings in patients with neurological disorders (Baker et al., 2015; Galna et al., 2014; Robinson et al., 2015; Shin et al., 2014; van der Kuil et al., 2018; I. Yoshida et al., 2018, 2019). By measuring flow experience, one can determine the extent to which patients engage with therapy interventions. It has been shown that being in a flow state during rehabilitation interventions may have a considerable positive impact on functional outcome (K. Yoshida et al., 2014, 2018). For instance, in patients with traumatic brain injury, attentional performance showed a greater improvement when attentional training was performed under a flow state compared with when it was not (I. Yoshida et al., 2014, 2018). Flow has also been shown to positively influence performance in settings other than therapy, such as in sports and during learning. For example, flow experience during competition predicted better performance in elite athletes (Jackson et al., 2001; Sklett et al., 2018; Stavrou et al., 2007), and students who experienced a flow state during learning performed significantly better in exams than those who did not (Engeser & Rheinberg, 2008).
A recent systematic review provided a summary of several flow questionnaires that have been used in therapeutic settings (Ottiger et al., 2021). However, although the measurement of flow states has been recommended (Baur et al., 2018), the review showed that none of the existing questionnaires has been specifically validated in patients with stroke. Indeed, the existing questionnaires seem to be validated only in healthy people, such as athletes and high school students (Jackson & Marsh, 1996; Martin & Jackson, 2008; Webster et al., 1993; K. Yoshida et al., 2013). In contrast to healthy people, patients with stroke are often confronted with different motor and cognitive impairments. Motor impairments are often related to hemiplegia (one-sided loss of strength), whereas cognitive impairments are mostly related to attentional deficits, reduced working memory, language impairments (aphasia), and unilateral neglect (Patel et al., 2003). Patients with cognitive impairments may experience difficulties in understanding the questions of the aforementioned questionnaires (e.g., the latter are too long and too complex), consequently affecting the validity of self-reported answers. Thus, a reliable, valid, and comprehensible questionnaire to measure flow state in stroke patients is still lacking. This tool is necessary and instrumental for evaluating the effects of flow on functional outcome and also for adapting the therapy program accordingly.
Our aim was to develop a new flow questionnaire that can be validly applied to stroke patients when they perform exercises (e.g., upper limb training) in a rehabilitative setting.
Method
Development of the Flow State Scale for Rehabilitation Tasks
In developing the new questionnaire, we searched for existing flow questionnaires and came across two interesting ones. On the one hand, we found the Flow Kurz Skala (FKS; Engeser & Rheinberg, 2008), which was originally validated with German university students and has been used in various activities of daily life to capture people’s experience of flow. The FKS consists of 10 items measured on a 7-point Likert scale ranging from 1 (disagree) to 7 (agree). On the other hand, a good candidate for the application in stroke patients appeared to be the Flow State Scale of Occupational Tasks (FSSOT; K. Yoshida et al., 2013). The FSSOT consists of 14 items, measured on the same Likert scale as the FKS. An advantage of the FSSOT is that it was primarily developed to measure patients’ flow states in a therapeutic setting such as occupational therapy. However, the validity of the FSSOT was evaluated so far only in students who were engaged in computer games that could elicit three psychological states: flow, anxiety, or boredom. In this population, the FSSOT showed good psychometric properties (K. Yoshida et al., 2013). However, in reviewing these two questionnaires more in depth, we found that the questions might be too complex for poststroke patients. Because the FSSOT was primarily designed for occupational therapy, we decided to use the FSSOT as a basis for the development of the new flow questionnaire.
The original authors of the FSSOT (K. Yoshida et al., 2013) translated the original Japanese version into English. With their permission, we translated the English version into German according to the recommendations for cross-cultural validation and adaptation of self-report questionnaires and following the guidelines of the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN; de Vet et al., 2011 ; Terwee et al., 2018). Two translators independently translated the FSSOT (including instructions, item contents, and response options) from the English version into a German version. This forward translation was performed by one occupational therapist who has knowledge about flow theory and by one linguistics expert in German and English who was naïve with respect to the topic. The two translators and the first author (Beatrice Ottiger) combined the results of both translations into an integrated, common version of the forward translation. This common forward translation version was translated back into the original language (English) by a bilingual language teacher whose mother tongue is English and who was naïve with respect to the topic. For reconciliation and harmonization, this back-translation was compared with the original version by all involved translators to find a consensus. No further adjustments were necessary at this stage.
This translated version was tested on 10 stroke patients (5 women and 5 men; median age = 69 yr; Quartile 1 = 66; Quartile 3 = 79) to verify the comprehensibility of the translation. We selected patients who understood the German language, and their cognitive ability was tested using the Montreal Cognitive Assessment (MoCA; Chiti & Pantoni, 2014; Nasreddine et al., 2005; median = 23.5 points; Quartile 1 = 22; Quartile 2 = 26; range = 17–30). After an occupational intervention (in this case, upper limb training), they were given the flow questionnaire to complete and were then asked immediately if they understood the questions and whether they had any further comments on the questionnaire. As feedback, the patients reported that the questions were posed in a way that was too general. Additionally, they advised to keep the questions simple and clear. More specifically, they would have preferred the questions to refer to a specific task. Therefore, for easier understanding, we reformulated the questions with simpler morphosyntactic constructions and in direct form. Moreover, all questions were reformulated in a simpler language and made explicit reference to the exercises they were doing (i.e., Question 1 in original form, “I had a meaningful time,” was reformulated as “The exercises were meaningful”; Question 14 in original form, “I wanted to do it again,” was reformulated as “I want to repeat the exercises”). Question 2 (in original form, “I knew clearly what I wanted to do or what I should do at every moment”) was interpreted ambiguously. It was not clear to the patients whether they had to judge what they wanted to do or what they should do. Thus, this question was generally difficult for the patients to understand. For this reason, we simplified the sentence and formulated the question with explicit reference to the exercises: “I knew what I had to do during the exercises.”
Furthermore, we decided to remove three items for different reasons. First, the reversed Question 9 (in original form, “The task was really boring”) repeatedly caused confusion, because the patients were not sure as to whether they filled it out correctly. Moreover, Question 5 (in original form, “I felt that I could deal with whatever might happen next”) was not understood by the patients in relation to upper limb training, and they had the impression that the question concerned life in general. For this reason, we removed this question. In addition, we checked which of the questions had similar content to avoid redundancies. Question 6 (in original form, “It felt like time passed quickly”) and Question 11 (in original form, “I lost track of time while doing the task”) both have the same content; that is, they aim to assess altered time perception. Question 6, however, has the disadvantage of explicitly asking about a sped-up perception of time; that is, if a patient had a slowed-down perception of time, this would not be detected by the question. Therefore, we decided to keep Question 11, which more generally captures altered time perception, and to remove Question 6. Moreover, Question 11 was also formulated in relation to the exercises. The final feedback by the patients was that the extension of the scale for the possible answers (i.e., from 1 to 7) was too broad and that a narrower scale would have been preferred. Thus, we adopted a 5-point Likert scale for the adapted version, which proved to be much easier for patients.
The first author (Beatrice Ottiger) and an occupational therapist with strong expertise in the conceptualizing flow theory (see previous work; Ottiger et al., 2021) evaluated and discussed all the aforementioned suggestions made by the patients. Subsequently, all the aforementioned changes were incorporated in a final version of the questionnaire. The final version was presented to the occupational therapists and physical therapists at the Neurocenter of the Luzerner Kantonsspital during an interdisciplinary workshop. Because the newly developed 11-item flow questionnaire significantly differed from the FSSOT in terms of questions, number of questions, and scoring, we named the new version the Flow State Scale for Rehabilitation Tasks (FSSRT; see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Determination of the FSSRT's Psychometric Properties
Design
In the next step, the FSSRT was evaluated in a new sample of patients with stroke. For this purpose, a single-center prospective cohort study was conducted at the neurorehabilitation unit of the Neurocenter of the Luzerner Kantonsspital in Lucerne, Switzerland.
Participants
A sample of 50 inpatients with a diagnosis of stroke was consecutively recruited between May 2018 and October 2019.
Inclusion and Exclusion Criteria
Inclusion criteria were a diagnosis of stroke of any type according to the International Classification of Diseases (10th rev.; World Health Association, 1993), as confirmed by brain computed tomography or magnetic resonance imaging; a score of less than 54 points on the Action Research Arm Test (Lyle, 1981); and a score of more than 14 points on the MoCA (Chiti & Pantoni, 2014; Nasreddine et al., 2005). Patients who could neither read nor understand the German language were excluded.
Ethical Considerations
Before study participation, written informed consent was obtained from all patients. The study was conducted according to the latest version of the Declaration of Helsinki. Ethical approval was provided by the Cantonal Ethics Committee Northwest and Central Switzerland (EKNZ 2018–00645), Lucerne, Switzerland. The work adhered to the World Medical Association Declaration of Helsinki (World Medical Association, 2013), and reporting adhered to the Strengthening the Reporting of Observational Studies in Epidemiology statement (von Elm et al., 2014).
Procedure
The patients included in the study received intensive upper limb training (five sessions per week, each lasting 30 min) during their neurorehabilitation stay. Depending on the severity of arm paresis, patients performed either mirror therapy with motor imagery, modified constraint-induced movement therapy (Kwakkel et al., 2015), or arm skills training from the impairment-oriented therapy concept (Platz, 2004). The occupational therapist in charge was following the international best practice application for arm recovery after stroke (Wolf et al., 2016) and decided which of the mentioned upper limb trainings was the most appropriate for each patient. Therapy assistants accompanied the patients during the arm training sessions. They also handed over the FSSRT and gave them instructions on how to complete it. The FSSRT was filled out at two time points: immediately after the training session at the end of the first week and immediately after the training session at the end of the second week. In addition to the FSSRT, patients completed the FKS (Engeser & Rheinberg, 2008) for the assessment of construct validity in the validation procedure. The properties of the FKS are described in more detail in the following section, Data Collection and Outcome Measures. The therapy assistants instructed the patients on how to complete both questionnaires: “Please recall the exercises you have just performed and answer the following questions with specific reference to these exercises. There are no right or wrong answers. Please rate the statements intuitively. For each question, circle the number from 1 (strongly disagree) to 5 (strongly agree) for the FSSRT and from 1 (strongly disagree) to 7 (strongly agree) for the FKS that best matches your experience.” If there were any uncertainties in filling out the questionnaires, the patients could ask for help from the therapy assistants.
Data Collection and Outcome Measures
Medical and Sociodemographic Data
Medical and sociodemographic data such as age, gender, stroke type (ischemic or hemorrhagic), time after stroke, and length of stay in neurorehabilitation were collected from the patients’ record.
FSSRT
The FSSRT consists of 11 items that are measured on a 5-point Likert scale ranging from 1 (disagree) to 5 (agree); see Table A.2 in the Supplemental Material. The FSSRT total score ranges from a minimum of 11 points to a maximum of 55 points; higher scores indicate higher levels of flow. The time needed to complete the FSSRT was measured and presented as mean, range, and standard deviation (SD) and presented in Table 1.
Study Sample Demographics and Characteristics
Note. N = 50. FKS = Flow Kurz Skala; FSSRT = 11-item Flow State Scale of Rehabilitation Tasks; HADS = Hospital Anxiety and Depression Scale; LIMOS = Lucerne ICF-Based Multidisciplinary Observation Scale; MoCA = Montreal Cognitive Assessment.
Values in parentheses indicate skewness and kurtosis.
FKS
To verify that the FSSRT score effectively measures the construct of flow (i.e., criterion validity), we correlated the FSSRT total score with the FKS total score (Engeser & Rheinberg, 2008). The FKS consists of 10 items that are measured on a 7-point Likert scale ranging from 1 (disagree) to 7 (agree). The FKS score thus ranges from a minimum of 10 points to a maximum of 70 points; higher scores indicate higher levels of flow.
HADS
The Hospital Anxiety and Depression Scale (HADS), a self-report questionnaire measuring the state of mood, was chosen to assess divergent validity. Anxiety and depression are known opponents of the flow experience (Csikszentmihalyi, 2014; Nakamura & Csikszentmihalyi, 2009; K. Yoshida et al., 2013). The HADS, a well-known, validated scale that is commonly used with hospitalized patients, is composed of an anxiety subscale (HADS–A) and a depression subscale (HADS–D), each consisting of seven items and measured on a 4-point Likert scale ranging from 0 (absence) to 3 (extreme presence). The total score can thus range from 0 to 42 points (i.e., 21 per subscale; higher scores indicate higher levels of depression and/or anxiety; Aben et al., 2002). The HADS total score can be used as a global measure of psychological distress (Johnston et al., 2000; Roberts et al., 2001) and has been shown to exhibit adequate to excellent psychometric properties in stroke patients (Aben et al., 2002).
Montreal Cognitive Assessment
We investigated the potentially confounding effect of cognitive impairments on flow experience. Therefore, we used the MoCA (Chiti & Pantoni, 2014; Nasreddine et al., 2005), which is a cognitive screening tool that helps health professionals identify mild cognitive impairment. The total maximum possible score of the MoCA is 30 points, with higher scores indicating better cognitive abilities. Physicians assessed patients’ general cognitive ability with the MoCA on admission to the neurorehabilitation unit.
Lucerne ICF-Based Multidisciplinary Observation Scale
Furthermore, we investigated whether restrictions in the performance of ADLs could have an influence on the flow experience. The Lucerne ICF-Based Multidisciplinary Observation Scale (LIMOS; Ottiger et al., 2015) was completed to assess the patient’s ability to perform ADLs on admission to neurorehabilitation. The LIMOS is a reliable and valid observation scale for stroke patients and is based on the International Classification of Functioning, Disability and Health (ICF; Ottiger et al., 2015; Vanbellingen et al., 2016). On patient admission to neurorehabilitation, the LIMOS was routinely completed by trained health professionals such as nurses, therapists, and physicians in charge of the patient.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 25.0). Descriptive statistics for qualitative data were expressed as number of cases and percentages. In case of normal distribution, descriptive statistics for quantitative data included the mean, SD, and range. In case of nonnormal distribution, descriptive statistics included the median as well as first and third quartiles. For all analyses, a two-tailed p value, with a critical value of .05, was used as the threshold for ascertaining statistical significance.
Reliability Analyses
Internal Consistency
Cronbach’s α was calculated for testing the degree of interrelatedness among items (i.e., internal consistency) of the FSSRT. A value more than .70 was considered to reflect an acceptable homogeneity of the items within the total scale (Bland & Altman, 1997; Mokkink et al., 2010).
Test–Retest Reliability
Test–retest reliability was defined as “the extent to which scores for patients who have not changed are the same for repeated measurement under several conditions” (Mokkink et al., 2010, p. 473). To determine the test–retest reliability, the patients were asked to complete the FSSRT 1 wk later. For this comparison, the intraclass correlation coefficient (ICC; a two-way mixed model with an effect of absolute agreement; Shrout & Fleiss, 1979) was computed. An ICC value more than .70 was considered acceptable (Lance et al., 2006).
Measurement Error
The measurement error was determined by calculating the standard error of measurement (SEM), which was defined as “the systematic and random error of a patient’s score that is not attributed to true changes in the construct to be measured” (Mokkink et al., 2010, p. 473). The SEM was calculated by dividing the SD of the difference between test (baseline) and retest scores (1 wk later), respectively, by the square root of 2 (de Vet et al., 2011; Harvill, 1991).
Validity Analyses
Structural Validity
Structural validity refers to “the degree to which the scores of a health-related patient reported instrument are an adequate reflection of the dimensionality of the construct to be measured” (Mokkink et al., 2010, p. 743). For this purpose, we conducted a principal component analysis (PCA) to explore the underlying dimensions of the FSSRT. A PCA defines the degree to which items of the FSSRT are correlated with each other, therefore building a common dimension within the total questionnaires. A minimum eigenvalue of 1 was specified as the extraction criterion. The criterion for factor loading was set at .40 (Fleiss, 1986; Mokkink et al., 2010).
Hypothesis Testing for Construct Validity
Hypothesis testing in the context of construct validity was defined as “the degree to which the scores of another outcome measurement instrument are consistent with hypotheses” (e.g., with regard to internal relationships, relationships to scores of other instruments, or differences between relevant groups) on the basis of the assumption that the health-related patient-report instrument validly assesses the construct to be measured (Mokkink et al., 2010, p. 473). To support construct validity, we calculated a Pearson’s correlation between the FSSRT sum score and the FKS sum score. We expected a high correlation (r > .60; Mokkink et al., 2010) between the scores of these two flow questionnaires.
Hypothesis Testing for Divergent Validity
Hypothesis testing in the context of divergent validity was defined as “the degree to which the scores help to establish construct validity by demonstrating that the construct you are interested in (e.g., anger) is different from other constructs that might be present in your study (e.g., depression)” (Mokkink et al., 2010, p. 473). We hypothesized that the HADS would show a moderate, negative correlation (r between −.30 and −.59) with the overall FSSRT score. Similarly, we expected moderate, negative correlations between the overall FSSRT score and the HADS–A and HADS–D. Furthermore, to exclude confounding factors, we hypothesized low correlations (rs < .30) between, on the one hand, the FSSRT sum score and cognitive impairment (as measured by the MoCA score) and, on the other hand, the FSSRT sum score and restrictions in ADL performance (as measured by the LIMOS score; Fleiss, 1986; Mokkink et al., 2010).
Responsiveness
On the basis of the SEM, the distribution-based responsiveness was determined by calculating the minimum detectable change with 90% certainty, or the MDC90
Floor and Ceiling Effects
The floor and ceiling effects reflect the extent to which scores cluster at the bottom and at the top of the scale range, respectively. To ascertain the presence of floor or ceiling effects, we checked whether 15% of respondents scored the lowest or highest total sum score on a scale, respectively (McHorney & Tarlov, 1995).
Results
Patient Characteristics
Fifty patients with (sub)acute stroke were included in the validation study (see flowchart in Figure 1). The demographics and the baseline characteristics of the patients at admission to neurorehabilitation are presented in Table 1.
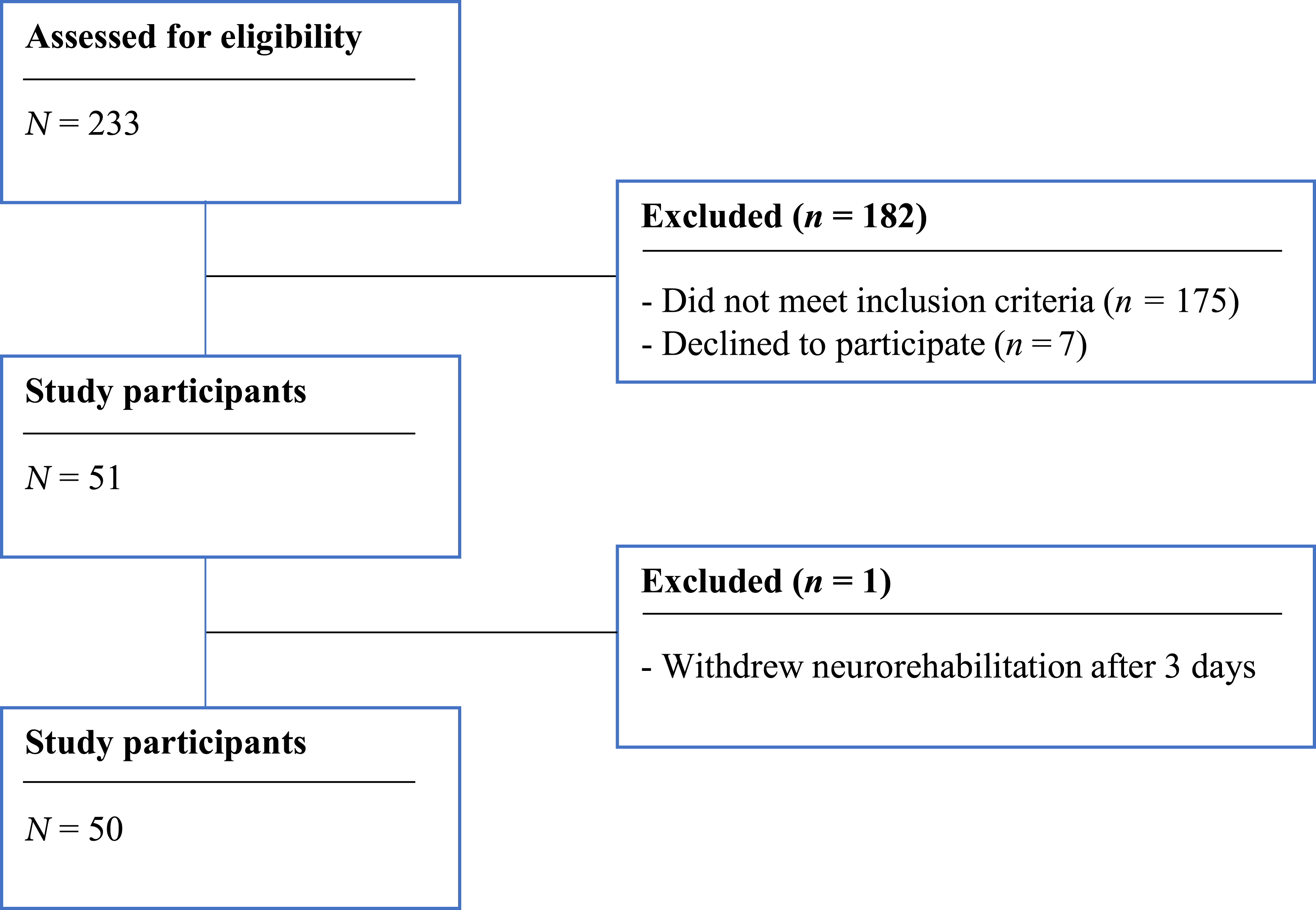
Flowchart of the patient sample.
Reliability
Internal Consistency
For the 11 items of the FSSRT, Cronbach’s α = .714, which reflects an acceptable homogeneity of the scale (Mokkink et al., 2010).
Test–Retest Reliability
The test–retest reliability of the FSSRT within 1 wk (N = 50) was excellent: ICC = 0.81, 95% confidence interval [0.66 – 0.89], p < .001. For the remeasurement within 1 wk, the SEM = 3.31 points.
Validity
Structural Validity
Concerning structural validity, the PCA resulted in four components, each with an eigenvalue of more than 1.0, explaining in total 64.35% of the variance. First, we performed the nonorthogonal rotation method “direct oblimin.” In this analysis, we checked the factor correlation matrix for values more than ±.32 using the criterion explained by Tabachnick and Fidell, (2007, p. 646). No values more than ±.32 were found in this analysis. According to Tabachnick and Fidell (2007), the orthogonal rotation method can be used if the values do not exceed ±.32. Therefore, we performed the orthogonal rotation method varimax. After varimax rotation, all the 11 items presented a loading of more than .40 on at least one of the four components. The eigenvalues of the four components and the rotated factor loadings are presented in Table 2.
Principal Components Analysis: Rotated Factor Loadings
First, the PCA revealed that all 11 items of the FSSRT correlated (r ≥ .3) with at least one other item, suggesting reasonable factorability. Second, the Kaiser–Meyer–Olkin measure of sampling adequacy was .665, which is more than the recommended minimal value of .6, and Barlett’s test of sphericity was significant: χ2(55) = 115.56, p < .001. The diagonals of the anti-image correlation matrix had also all values more than .5.
Hypothesis Testing for Construct Validity
Concerning construct validity, we found a significant and strong correlation between the FSSRT and the FKS total scores (Pearson r = .81, p < .001).
Hypothesis Testing for Divergent Validity
The HADS total score correlated significantly and negatively with the FSSRT total sum score (Pearson r = −.525, p < .001). Further significant negative and moderate correlations were found between the FSSRT and the HADS–A (Pearson r = −.486, p < .001) and between the FSSRT and the HADS–D (Pearson r = −.442, p < .001). Neither cognition (MoCA: Pearson r = .120, p > .05) nor ADL performance level (LIMOS sum score: Pearson r = .138, p > .05) resulted in a significant correlation.
Responsiveness
The MDC90 within 1 wk was 7.71 points, which indicates a change of 17.52% on the total scale as a real change in experience flow for a patient (i.e., beyond the measurement error).
Floor and Ceiling Effects
Neither floor nor ceiling effects were observed for the total FSSRT. The percentage of patients who achieved the lowest FSSRT total sum score was 0%; the highest sum score was 3.9%.
Discussion
This study presents the new self-reported flow questionnaire, the FSSRT, for use in stroke rehabilitation wards. It consists of 11 items, which we show to load on four components: concentration, enjoyment, movement control, and absorption. This flow construct showed good construct and criterion validity. Moreover, a high test–retest reliability and responsiveness were found. Because of its short administration time (less than 3 min), as well as short questions formulated in plain language, the FSSRT is suitable for the application in a broad population of stroke patients, even those who suffer from mild to moderate cognitive impairment.
The test–retest reliability of the FSSRT was good within a week. This means that the FSSRT remained stable over repeated measurements for the stroke patients whose flow experience did not clinically change. On the basis of the responsiveness, a change of at least 7.71 points within 1 wk can be interpreted with 90% confidence that the flow experience has changed over time. The absence of floor and ceiling effects suggests that there is room to detect improvement or deterioration in flow experience at both ends of the FSSRT. The internal consistency of the newly developed FSSRT (Cronbach’s α = .714) was lower than that of the original FSSOT (Cronbach’s α = .918; K. Yoshida et al., 2013), but still acceptable. The reasons for this discrepancy can be manifold. First, our sample size was smaller than that of K. Yoshida and colleagues (K. Yoshida et al., 2013). Second, we reduced the number of items from 14 to 11. It is well known that both sample size and items number may affect the internal consistency (Bujang et al., 2018). A third reason might be the heterogeneity of our sample. We validated the FSSRT in stroke patients, who typically show a larger variability in their abilities and disabilities, compared with very homogeneous population of young students who were the target group for the validation of the original FSSOT. The differences in clinical presentation of symptoms across patients might explain more variable responses and, thus, contribute to a somewhat lower internal consistency. However, with an internal consistency value of more than .70, the FSSRT is definitely valid for clinical application (Mokkink et al., 2010).
The removal of three items was necessary, because they led to confusion in stroke patients. This procedure is well justified and in line with the COSMIN guidelines, which particularly emphasize the importance of good content validity of patient-reported outcome measures (PROMs; Mokkink et al., 2010). Indeed, the comprehensibility of a PROM should be high enough to allow the intended users to fully understand what they are asked. Particular attention should be paid to whether the PROM items are appropriately worded (Terwee et al., 2018). The original FSSOT included more complex formulations of the questions and was validated in a population of young students (K. Yoshida et al., 2013). By providing more plainly formulated questions, the newly developed and validated FSSRT can now also be used in stroke patients, who often suffer from reduced cognitive abilities. It is interesting that the nonsignificant correlation between the FSSRT and the MoCA scores further supports this notion.
The validity of the flow construct measured with the FSSRT is confirmed by the strong, significant correlation coefficient between the FSSRT and FKS scores. Furthermore, our findings show that the counterparts of flow experience—namely, depression and anxiety (Csikszentmihalyi, 2014; Nakamura & Csikszentmihalyi, 2009), as measured by the HADS—did significantly and negatively correlate with the FSSRT scores. A negative correlation between depression, anxiety, and flow experience could already be observed in young and healthy students (Engeser & Rheinberg, 2008; K. Yoshida et al., 2013). It seems particularly important to understand this relationship further. Indeed, patients are known to be at risk of developing anxiety and depression after suffering a stroke (Stein et al., 2018). If these patients experience little flow, then this could, in turn, indicate that they suffer from depression or anxiety. Therefore, they might be less able to engage in the upper limb training. However, the nonsignificant, weak correlation between LIMOS and flow experience scores indicates that flow experience is not dependent on the ability to perform ADLs in general. This suggests that stroke patients can also experience flow very well, regardless of their level of disability.
Limitations
We focused on measuring flow experience in regular clinical practice; that is, individual patients participated in different training programs that were chosen and adapted to their abilities. Therefore, the use of nonstandardized training protocols could be seen as a limitation. However, the use of standardized training programs may in turn be problematic, i.e., the tasks of the program may be too easy and not challenging for some patients, while being overwhelming difficult for others, depending on their abilities. The use of the FSSRT is limited, because the word exercises was used in the questionnaire. We have shown that the FSSRT is valid for exercise training and with this wording. For the FSSRT to be used in other meaningful therapeutic activities, such as example ADLs, this questionnaire should be retested in a different context and, accordingly, the word exercises in the questionnaire should be replaced with the term therapeutic activities. Furthermore, the study participants were in the (sub)acute phase after stroke. Therefore, we cannot make any statements about the validity of the scale in patients who are in the chronic phase after stroke. Finally, only one center recruited patients for this study. It would be worthwhile to conduct the study in several centers in parallel—ideally, internationally—to compare the results and assess the generalizability of our findings.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: ▪ Flow can be described as a subjective state that people report when they are completely involved in an activity and feel satisfaction and pleasure. This state is increasingly measured in physical and cognitive rehabilitation of patients with neurological disorders. ▪ The FSSRT questionnaire is reliable and valid for measuring the flow experience of patients after a (sub)acute stroke. ▪ The FSSRT can be completed by patients within a short time after a therapy session and provides the treating occupational therapist and physical therapist with important information about the flow experience during training. ▪ On the basis of the information provided by the FSSRT, the therapy program could be adjusted to increase the patient's experience of flow.
Conclusion
The FSSRT is a reliable, valid, and responsive questionnaire for measuring flow experience in patients with (sub)acute stroke. Measuring flow experience with the FSSRT is easy to implement in occupational therapy and physical therapy. Future studies could also validate the FSSRT in patients with other neurological disorders such as Parkinson’s disease, multiple sclerosis, and traumatic brain injury, as well as in patients with chronic stroke. Further studies could also test the FSSRT in the context of occupational therapy or physical therapy with other therapeutic activities, potentially adapting the word exercises with the term therapeutic activities.
Supplemental Material
Supplementary material for The Flow State Scale for Rehabilitation Tasks: A New Flow Experience Questionnaire for Stroke Patients
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050401.pdf for The Flow State Scale for Rehabilitation Tasks: A New Flow Experience Questionnaire for Stroke Patients by Beatrice Ottiger, Janne Marieke Veerbeek, Dario Cazzoli, Thomas Nyffeler and Tim Vanbellingen in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Katja Keller, Brigitte Sigrist, and Barbara Sotiriadis, who worked on the translation and back-translation in the phase of the development of the FSSRT for this study. We also thank all the therapy assistants who accompanied the patients during the arm training.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.