
Abstract
Group yoga may improve behavioral regulation for adults with acquired brain injury.
Acquired brain injury (ABI), or any brain damage occurring after birth, is an umbrella term encompassing both traumatic brain injuries (TBIs) and brain injuries with “nontraumatic” etiologies such as stroke, infections of the brain, and tumors (Teasell et al., 2007). Regardless of etiology, ABI may result in significant difficulties in everyday functioning across physical, cognitive, vocational, emotional, and social domains (Braden et al., 2010; Mozaffarian et al., 2015). Difficulties in cognitive domains after ABI may include deficits in executive function (EF; Chung et al., 2013). EF refers to a set of higher level cognitive processes that affect the ability to effectively engage in purposeful and goal-directed behavior; EFs are effortful and enable control over behavior, thought, and emotions (Cicerone et al., 2000; Miyake & Friedman, 2012; Waid-Ebbs et al., 2012).
Deficits in EF are common after ABI and may persist for years after injury (Chung et al., 2013; Marsh et al., 2016; Riepe et al., 2004). Impairment in EF, or executive dysfunction, is associated with difficulties in everyday decision making (Cicerone et al., 2000). Furthermore, executive dysfunction may lead to functional impairments, restrictions in participation in occupations, and reduced quality of life for people with ABI (Cramm et al., 2013; Pohjasvaara et al., 2002; Yousefzadeh-Chabok et al., 2021). Therefore, addressing EF should be a focus of rehabilitation efforts for people with ABI (Häggström & Lund, 2008).
Yoga is an ancient practice for physical, spiritual, and mental development with the initial aim of fostering the attainment of self-awareness (Field, 2011; Riley, 2004). In Western society, yoga has been clinically adapted and used as a treatment modality or therapeutic intervention for neurological, psychological, and medical conditions (Silveira & Smart, 2020). This style of practice typically aligns with hatha yoga, which involves physical postures (asanas), breathing exercises (pranayama), and meditation (dhyana; Büssing et al., 2012; Field, 2011). Yoga can be included in traditional rehabilitation as an alternative or complementary intervention, because it does not need to be prescribed by a physician or approved by insurance (Schmid et al., 2016). Specifically, yoga may be used in occupational therapy, because the American Occupational Therapy Association (AOTA) supports the use of complementary health approaches and integrative health practices (Bradshaw, 2017). Yoga may be applied in practice as a preparatory method, occupation, or activity to address health outcomes, ultimately enhancing participation in other meaningful occupations and roles (AOTA, 2020; Bradshaw, 2017).
Emerging evidence, although limited in scope, has shown that yoga is a holistic approach that can improve physical and psychological outcomes for people with ABI (Chan et al., 2012; Donnelly et al., 2017; Garrett et al., 2011; Schmid et al., 2012, 2016; Silverthorne et al., 2012; Stephens et al., 2020; Yeates et al., 2015). A growing body of research suggests that yoga, particularly hatha yoga, may improve EF in various populations (Luu & Hall, 2016). However, at this time, yoga for EF in ABI populations has been explored only in people with TBI in a study with 2 participants (Wen et al., 2021). Researchers continue to explore the underlying mechanisms of the yoga–cognition relationship; some researchers have proposed that the attenuation of stress, along with the quieting of the sympathetic nervous system and hypothalamic– pituitary–adrenal (HPA) axis, as induced by yoga, may support improved cognition (Gothe et al., 2016; West et al., 2004). Thus, the purpose of this study is to explore the impact of group yoga on EF for people with ABI.
Method
Design and Setting
This study is a secondary analysis from a parent study of brain imaging, balance, and yoga (Stephens et al., 2023). The parent study was a feasibility pilot study that investigated the feasibility and acceptability of group yoga on multiple outcomes; we focus here on the included outcome measure of EF. Participants completed a yoga intervention and pre- and postyoga assessment visits; these were completed in university buildings on a college campus.
Participants
Participants were recruited through convenience and purposive strategies by word of mouth, prior related research studies, social media, newsletters in the local community, electronic mailing lists, and stroke and brain injury support groups. Inclusion criteria included self-reported chronic ABI (≥6 mo postinjury), self-reported balance issues, ability to stand with or without an assistive device, and the ability to read and understand English. The Colorado State University Institutional Research Board approved all study procedures, and all participants provided written consent to participate. Participants received yoga materials (mat and yoga blocks) and nominal financial incentives.
Intervention
The adaptive yoga intervention included 1-hr in-person sessions, once a week for 8 wk, along with the option to attend 90-min live online yoga sessions three times per week. In-person and online yoga sessions were delivered in a group format by a registered yoga teacher who specializes in adaptive yoga. All sessions included breathwork, postures, and meditation (Table 1). Although yoga was delivered in a standardized approach and was appropriate for beginner-level participants, postures were modified or adapted as needed to meet participants’ needs and abilities. Postures were completed while seated, standing (with or without support), and on the floor with props. Props were used during yoga to enhance successful completion of yoga postures: They included yoga mats, walls, chairs, bolsters, blankets, and yoga blocks. Supervision for safety and minimal physical assistance for adaptive poses was provided by assistants during in-person classes. Over the 8-wk period, yoga sessions were designed to build on one another and were progressively difficult. Attendance for both in-person and virtual sessions was recorded.
Yoga Protocol
Online sessions were offered three times a week by the same yoga teacher to increase the dose of yoga without the increased risk of exposure to coronavirus disease 2019 (COVID-19; this study was completed in Fall 2021). Live online yoga sessions were provided as a group intervention that involved a similar yoga protocol as the in-person classes. Assistants attended online sessions and provided one-on-one assistance in breakout rooms if needed.
Measures
Pre- and postyoga assessments were conducted approximately 2 wk before the start of yoga and 2 wk after the final yoga class by a trained assistant and included demographic data. EF in everyday functioning was assessed using the Behavior Rating Inventory of Executive Function—Adult Version (BRIEF–A; Roth et al., 2005). The BRIEF–A is a self-report measure of 75 items grouped into nine clinical scales of EF: Inhibit, Shift, Emotional Control, Self-Monitor, Initiate, Working Memory, Plan–Organize, Task Monitor, and Organization of Materials. The nine clinical scales form two summary indices: the Behavioral Regulation Index (BRI) and the Metacognition Index (MI). The BRI consists of the Inhibit, Shift, Emotional Control, and Self-Monitor scales. The MI consists of the Initiate, Working Memory, Plan–Organize, Task Monitor, and Organization of Materials scales. The BRI and MI are combined for an overall total or summary score: the Global Executive Composite (GEC). Higher T scores reflect more reported problems, and T scores at or above 65 are generally considered clinically significant, indicating impaired EF (Roth et al., 2005). The BRIEF–A has demonstrated validity and reliability for the assessment of EF in adults with a range of abilities, particularly adults with TBI, and it is used in research and clinical settings (Roth et al., 2005; Seichepine et al., 2013; Waid-Ebbs et al., 2012). There is not a meaningful clinical difference or threshold established for the BRIEF–A.
Data Analysis
Data were analyzed using IBM SPSS Statistics (Version 28). Descriptive statistics, including means, standard deviations, proportions, and frequencies, were used to describe the demographics and ABI characteristics of the sample. The normality of the data was assessed with the Shapiro–Wilk test. For data that were normally distributed, we used paired t tests to assess change between baseline and 8-wk scores. The effect size (Cohen’s d) was calculated for statistically significant results. Additionally, a percent change calculation was performed for each scale, index, and summary score: [(Time 1 – Time 2)/Time 1] × 100. Because the subscales were nonoverlapping and measured different constructs, we did not use corrections for multiple comparisons.
Results
Twelve people enrolled in the study. An overview of patient demographics and ABI characteristics are reported in Table 2. The participants’ ages ranged from 29 to 74 yr. Most participants were White (92%), were female (58%), and had an education level of baccalaureate or greater (50%). Etiologies of brain injuries included stroke (n = 3), TBI (n = 4), mild TBI or multiple concussions (n = 3), anoxic brain injury (n = 1), and hydrocephalus (n = 1). Of the 12 participants who enrolled in the study, 9 completed all study procedures. The mean number of in-person sessions attended by the 9 participants was 7.1 (SD = 1.1). Three participants attended online classes. Study withdrawal was due to scheduling issues (n = 2) and unrelated illness (n = 1).
Demographics and ABI Characteristics
Note. n = 12. M age = 45.0 yr (SD = 15.8); age range = 29–74. ABI = acquired brain injury; TBI = traumatic brain injury.
Data were normally disturbed; thus, paired t tests were used to evaluate changes in EF scales, indices, and the overall summary score (Table 3). Results indicated a significant improvement in the BRI between preyoga scores (M = 56.3, SD = 11.8) and postyoga scores (M = 53.7, SD = 11.2, p = .046, d = 0.226). Cohen’s d was 0.226, indicating a small effect size. There were no statistically significant changes between pre- and postassessments on the EF scales, the MI, or the GEC. A decrease in scores indicates improved EF in daily living (Figure 1).
Changes in Executive Functioning (EF) on Behavior Rating Inventory of Executive Function—Adult Version After Yoga (n = 9)
Note. A decrease in T score indicates improvement in EF. BRI = Behavioral Regulation Index; EF = executive function; GEC = Global Executive Composite; MI = Metacognition Index.
a[(Time 1 – Time 2)/Time 1] × 100.
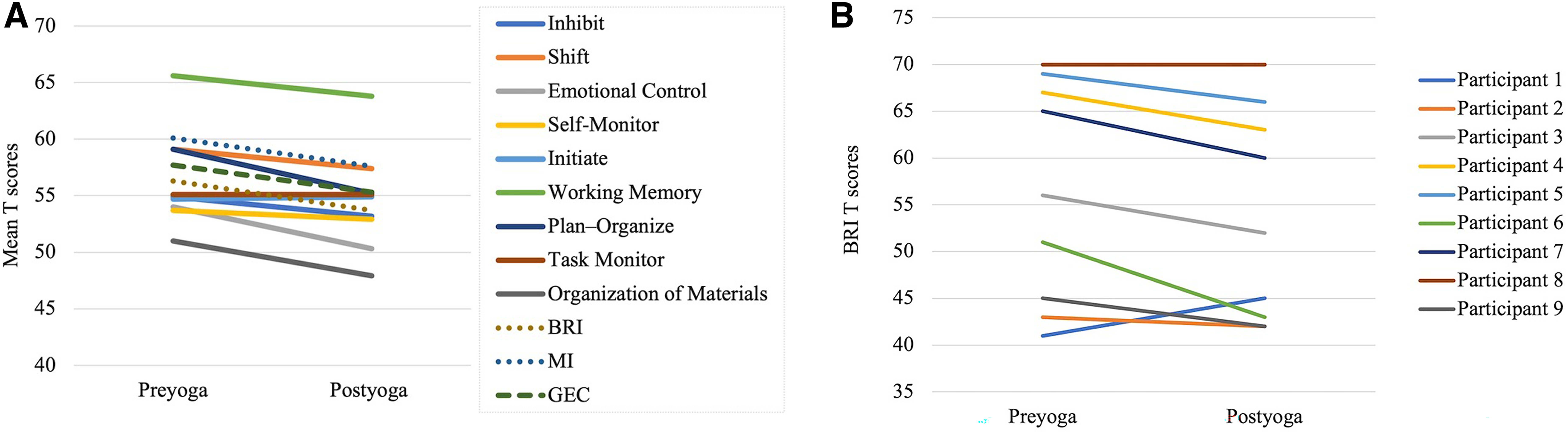
BRIEF–A: (A) changes in executive function pre- to postyoga and (B) individual changes on the BRI pre- to postyoga.
Discussion
To our knowledge, this is the first study to examine the impact of yoga on EF for people with ABI. Despite our small sample size, we found that participants significantly improved on the BRI. Although changes pre- to postyoga for the nine EF scales, the MI, and the GEC did not reach statistical significance, changes were in the expected downward direction, with lower scores indicating improved EF.
The findings of our study align with those of previous studies on the effects of yoga on EF in non–brain-injury populations. Luu and Hall (2016) completed a systematic review on hatha yoga and EF and concluded that varying doses of hatha yoga show promising benefits for EF in healthy adults, healthy children and adolescents, healthy older adult populations, prisoners, and people with diabetes. Most commonly, the studies highlighted in the Luu and Hall (2016) review used objective measures to measure changes in EF. In contrast, our present study used a self-report measure.
Our study adds to the literature on cognitive and EF benefits for people with ABI postyoga. The BRI is made up of the Inhibit, Shift, Emotional Control, and Self-Monitor scales. Although significant changes were not found on these scales, mean T scores for each scale improved from pre- to postyoga. It is likely that changes in emotional control led to significant improvements on the BRI. Improvements in behavioral regulation, as seen in our study, align with previous findings from Grimm et al. (2017), who found improvements in emotional regulation for 3 participants with TBI after an 8-wk yoga program. In contrast to our findings on behavioral regulation, Donnelly et al. (2021) found no improvements in emotional and behavioral dysregulation in a mixed-methods, pre-post study on yoga for people with TBI (n = 705); however, qualitative content analysis in their study revealed better ability to regulate impulsivity, anger, stress, and anxiety.
In studies of non–brain-injury populations, yoga has been shown to have a downregulatory effect on the sympathetic nervous system (SNS) and HPA axis in response to stress (Menezes et al., 2015; Ross & Thomas, 2010). This quieting effect on the SNS–HPA axis potentially allows for improved emotional and behavioral regulation (Menezes et al., 2015). It is unknown whether this response is also seen after brain injury, but it is likely to be the reason for changes in behavioral regulation, as reported in our study.
Limitations
One limitation of this study is that there was a small sample size, and, therefore, the study likely lacked the statistical power to detect significant decreases in all EF scales. Additionally, we did not correct for multiple comparisons, leaving us at risk for Type 1 statistical error. Because of the sample size and lack of representation of the larger population, the results are not generalizable. This study was conducted in a smaller city in the western United States that includes a highly educated population who may have been more likely to participate in complementary therapies. Furthermore, not all participants were yoga naïve; some reported participating in yoga before this study. Another possible limitation is the inclusion of people of various abilities and ages in the same yoga class, because the yoga intervention may not have been challenging enough for all participants. Perhaps separating into multiple classes on the basis of skill level would have been more beneficial for participants.
The use of the BRIEF–A self-report alone to measure EF may be considered a limitation: Although the BRIEF–A is valid and reliable for TBI populations, the self-report form may not have accurately gathered information about EF, because people with ABI may experience deficits in self-awareness (Prigatano, 2005). Likewise, the BRIEF–A consists of 75 items, and participants may have struggled to complete the entire form. Thus, although the chosen assessment was appropriate for the study population, it is unknown whether the study participants were able to accurately complete the BRIEF–A self-report form (Prigatano, 2005; Roth et al., 2005). Perhaps, including the BRIEF–A informant report (to be completed by a spouse, caregiver, adult child, etc.) or an objective EF measure would provide additional information or demonstrate differences between informant ratings, self-report ratings, and objective performance (Roth et al., 2005). An additional consideration is that, at preyoga, the mean summary score (GEC) on the BRIEF–A was a T score of 57.7. T scores of 65 or higher are typically considered clinically significant (Roth et al., 2005). Therefore, participants in this study may not have been experiencing notable difficulties in EF and, consequentially, significant improvements in EF were not seen on all areas of this measure. Likewise, the BRIEF–A may not have been sensitive enough to detect changes in EF because of the 3-point Likert scale (on which 1 = never, 2 = sometimes, and 3 = often).
As mentioned earlier, this study was completed during COVID-19, which affected the planned dose of in-person yoga. The planned dose of yoga for our research trials was typically 16 in-person sessions, delivered twice per week over 8 wk (Grimm et al., 2017; Schmid et al., 2012; Stephens et al., 2020). In our study, in-person classes were only offered once a week to minimize the risk of COVID-19 exposure. To increase the dose, there was an option of online live classes; however, most participants (n = 6) only attended in-person classes. Because of the small sample size, a sensitivity analysis is not appropriate to examine the relationship between dosage and response. Although doses of yoga vary among previous brain injury studies, yoga once a week for 8 wk may not have been enough to see significant improvements in the nine clinical scales of the BRIEF–A.
Future Research
There is limited research on the impact of yoga on EF for ABI populations; thus, more research is needed in this area. In the future, researchers may consider using the informant-report version of the BRIEF–A, in addition to the self-report form, to gain a better understanding of each participant’s EF and subsequent changes. Additionally, direct observation or task-based measures evaluating EF may be used in conjunction with the BRIEF–A (Roth et al., 2005). Future researchers may consider incorporating an anxiety or stress measure to examine these factors as potential mediators of the yoga–EF relationship. Last, although yoga delivered through online classes is possible for some populations, we recommend that future research continue in-person yoga interventions for the ABI population, because of the difficulty accessing online classes, safety concerns, and the improved ability to deliver the intervention as planned (i.e., standing and floor poses; Engström et al., 2010; Schmid et al., 2016; Schulz-Heik et al., 2017).
Implications for Occupational Therapy Practice
Current occupational therapy treatment of cognitive deficits often involves cognitive rehabilitation (Radomski et al., 2016; Wheeler et al., 2016). Occupational therapists may use remedial or compensatory treatment approaches to address cognitive impairments. Because of mixed findings regarding the efficacy of cognitive rehabilitation on outcomes of EF for persons with ABI, other intervention approaches, such as yoga, may be considered (Chung et al., 2013; Radomski et al., 2016; Raymer et al., 2018). Yoga can be included in occupational therapy practice as a preparatory or purposeful activity, and it appears that occupational therapists are using yoga after stroke and other brain injuries (Andrews et al., 2021). This study confirms previous work that group yoga is a possible intervention for people with ABIs of various etiologies (Schmid et al., 2012; Stephens et al., 2020).
The findings of this study have the following clinical implications for occupational therapy practice: Adaptive group-based yoga may improve behavioral regulation for adults with chronic ABI, although larger studies that demonstrate similar findings are needed. The treatment is a possible intervention for adults with chronic ABI and shows potential to address aspects of EF.
Conclusion
In conclusion, our findings suggest a group yoga intervention for people with ABI may improve some aspects of EF. Overall, more research is warranted to examine the impact of yoga on EF–cognition for people with ABI, including studies with larger sample sizes, randomized controlled trials, and different types of EF assessments.
Footnotes
Acknowledgments
This study was funded by an Early Career Investigator grant from the Colorado State University, College of Health and Human Sciences, to Jaclyn A. Stephens and Arlene A. Schmid. We thank Jennifer Atkins for delivering the yoga intervention, along with Samy Mattei, Carly Huyber, and Sara Dunn who served as yoga intervention aides. Additionally, we acknowledge our research assistants, Susan Mingils, Brea King, Abby Richards, Abril Butler, and Denny Press, who supported data collection and entry. Finally, we acknowledge the study participants, without whom this research would not have been possible.