
Abstract
This research identifies barriers and facilitators regarding insufficient knowledge about occupational therapy’s role in cancer care and adds a better understanding of gaps in referrals to occupational therapy.
As the survival rate for persons living with and beyond cancer (PLWBC) increases, some of their functional daily needs remain unmet. PLWBC have many treatment-related symptoms associated with short- and long-term restricted daily participation and quality of life (Keesing et al., 2018; Loubani et al., 2022; Sleight & Duker, 2016). Despite the fact that many PLWBC live with restricted participation after cancer and cancer treatments (Polo & Smith, 2017), they are not referred to occupational therapy services (Sleight & Duker, 2016).
Occupational therapy services are underutilized despite growing evidence of their effectiveness in cancer care. There is increasing evidence of the positive outcomes of occupational therapy interventions in ameliorating functional deterioration and enhancing daily participation for PLWBC (Amatya et al., 2017; Pergolotti et al., 2016; Polo & Smith, 2017; Robb & Davis, 2015). However, according to various international articles (Baxter et al., 2017; Halkett et al., 2010; Mackenzie, 2021), there is an underutilization of occupational therapy services that creates a gap in cancer care. One factor contributing to the underutilization of occupational therapy services is a lack of referrals.
Referrals of PLWBC to occupational therapy from other cancer health care professionals are limited internationally (Mackenzie, 2021; Pergolotti et al., 2016; Sleight et al., 2022). It is believed that a limited understanding of occupational therapy’s role in cancer care hinders comprehensive care and negatively affects the provision of services, referrals, and collaboration with other health care professionals (Ellen et al., 2021; Mackenzie, 2021; Maiwald et al., 2022; Olsson Möller et al., 2020; Pergolotti et al., 2016; Sleight et al., 2022). Additional barriers may stem from gaps in research and education focusing on holistic functional perspectives that can contribute to appropriate occupational therapy referrals (Baxter et al., 2017; Sleight & Duker, 2016). Identifying these barriers is essential if solutions to support rehabilitation services (including occupational therapy) for PLWBC are to be developed.
Studies that have explored barriers to referral and utilization of occupational therapy services among cancer health care professionals are scarce (Halkett et al., 2010). Cancer care nurses, nurse navigators, and social workers, who work with ordering sources (oncologists), typically are the ones responsible for care coordination and referrals to ensure that PLWBC receive occupational therapy services. Therefore, interviewing these health professionals can help us gain a deeper understanding of the barriers to and facilitators of referrals to occupational therapy services.
This study is Part 1 of an international collaboration among occupational therapy researchers from Israel and the United States. This collaboration includes two studies that were performed simultaneously in both countries. The purpose of this collaboration is to explore cancer health care professionals’ perspectives on the role of occupational therapy and describe current barriers to and facilitators of referrals to occupational therapy. In this article, we describe Part 1, which was conducted in Israel. The aims of this part of the study were as follows: ▪ explore the perspectives of cancer health care professionals in Israel regarding the role of occupational therapy in cancer care, ▪ explore health care professionals’ knowledge of the need for occupational therapy services for PLWBC, ▪ understand the current barriers to occupational therapy from the perspective of cancer health care professionals, and ▪ explore solutions suggested by cancer health care professionals to optimize occupational therapy referrals.
Method
To understand and generate a general explanation of the experience of cancer health care professionals, we adopted a grounded theory approach using a multiple-explanatory case study with a semistructured interview guide (Creswell & Poth, 2016; Yin, 2018). This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research guidelines (Tong et al., 2007).
Participants and Recruitment
We conducted purposeful sampling at a large health care institution; all participants were recruited from the main medical cancer center and three community health care clinics in major cities across Israel. The medical cancer center offers inpatient and outpatient clinics that encompass hematology–oncology, supportive services, palliative care, integrative medicine, social work, nutrition, psycho-oncology, psychiatry, physical therapy, and survivorship. Three community cancer clinics offer day care services for cancer treatments such as chemotherapy, biological and hormonal therapy, immunotherapy treatments, nutrition and diet services, physiotherapy, and complementary therapies. To meet inclusion criteria, at the time of the study, participants needed to practice in cancer health care as an oncologist, a nurse, or a social worker.
Data Collection
Khawla Loubani approached (via email and telephone) directors of cancer care departments and various community primary care clinics (i.e., oncologists, nurses, social workers) in one health care institution and invited them to participate. After an explanation of the study’s aims and Loubani’s professional background, the focus groups were scheduled. Focus groups were conducted with homogeneous samples of participants grouped by profession (i.e., social workers and nurses separately), as recommended by Creswell and Poth (2016). Participants provided signed consent and then filled out a short demographic and work-related questionnaire before the focus group began. Next, the focus group discussions were accomplished using questions from the semistructured interview guide (Table 1). Focus groups were conducted by Loubani, who has a PhD and is a postdoctoral occupational therapy researcher with experience in qualitative research and cancer care. She also audio recorded the group discussions, took field notes and memos, and transcribed the group discussions verbatim. Focus groups lasted about 90 min.
Interview Guide
Note. OT = occupational therapy; PLWBC = persons living with and beyond cancer.
Tools
The demographic questionnaire included questions regarding age (yr), educational degree (BA, MA, PhD, MD), workplace, position at work, years working in cancer care, and previous collaboration with occupational therapy (yes, no). In addition, an interview guide was used to guide the group discussions. The interview guide was developed by Loubani, Katie M. Polo, and Mary Frances Baxter, all doctoral-level occupational therapy researchers with experience in qualitative research. The questions were based on the study’s aims and were sufficiently unstructured to allow us to discover and generate an understanding of the barriers to and facilitators of occupational therapy referrals and what is needed to address the barriers. Before the first group was conducted, the study team reviewed and revised the interview guide with the assistance of two external PhD-level occupational therapy researchers with extensive qualitative research experience, one of whom also served as a note-taker and cofacilitator with Loubani for the first focus group.
Data Analysis
Descriptive statistics were used to describe the participants (demographic and work data). Qualitative data were analyzed by Loubani and Polo using grounded theory approach principles that included creating and organizing transcribed files, reading through the text, making margin notes, and forming initial codes. We then used open coding categories to identify key elements and formulate a codebook for continued data analysis. Axial coding was used to identify relations between the elements, and selective coding was used to create propositions and a theory to explain the relations in a final logic diagram (Creswell & Poth, 2016).
Procedures to Address Trustworthiness and Credibility
Loubani and Polo used an audit trail, including tracking of initial and final coding, the definition of codes, and notes about when and why decisions were made to support dependability and confirmability (Krefting, 1991). Our coding reached thematic saturation after the coding of four transcripts. A third PhD-level occupational therapy researcher, Debbie Rand, who has expertise in qualitative data analysis, performed an external audit to confirm logical reasoning and support dependability. We also conducted member checking with participants to determine the accuracy and credibility of the results and major themes.
Ethical Considerations
This project was reviewed and approved for human subjects protection by the Helsinki Committee of a nationwide health system. Participants signed written informed consent before the interview and were informed that they could refuse to answer any questions or withdraw from the study at any time. Participants’ anonymity was protected by deidentifying interview transcripts and ensuring that only the researchers had access to the data.
Results
The focus groups included cancer care nurses and social workers with different levels of experience and expertise within subfields of cancer care. Despite our best efforts to include oncologists (who were largely unavailable), we were able to recruit only nurses and social workers. Six focus groups were conducted (three groups included nurses, and three groups included social workers). There were 3 to 6 participants in each group, with a total of 28 participants. Additional demographics and work characteristics are described in Table 2.
Participants’ Sociodemographic Characteristics
Note. N = 28. All participants were women. “—” = not applicable; BA = bachelor of arts degree; MA = master of arts degree; OT = occupational therapy; SW = social worker.
a M = 49.79 (SD = 9.51).
bBA, n = 9 (25.0%); MA, n = 19 (67.9%).
cNurses, n = 15 (53.6%), SW, n = 13 (46.4%).
dHospitals, n = 16 (57.1%); community, n = 12 (42.9%).
e Mdn = 15.50 (interquartile range [IQR] = 7–21).
f Mdn = 5 (IQR = 5–11).
gYes, n = 9 (32.1%); No, n = 18 (64.3%); Sometimes, n = 1 (3.6%).
The qualitative findings identified two main themes regarding referrals to occupational therapy: (1) barriers to occupational therapy referrals and (2) partial facilitators of occupational therapy referrals. In addition, participants suggested practical solutions to overcoming perceived barriers and to enhance referrals to occupational therapy services.
Theme 1: Barriers to Occupational Therapy Referral
Barriers included issues related to gaps in knowledge of the effects of cancer symptoms on daily functioning, gaps in knowledge regarding occupational therapy’s role in cancer care, bureaucracy, and a lack of occupational therapy availability.
Gaps in Knowledge About Symptoms’ Effects on Daily Functioning
In general, cancer care nurses demonstrated a good understanding of various cognitive, emotional, and physical symptoms; however, they could not explain how these symptoms specifically affect daily functioning, which is imperative for occupational therapy referrals. In particular, participants shared many examples of different symptoms and side effects of medical cancer treatments, such as describing how “the lymphedema problems . . . restrict movement. . . . It is very difficult for [patients] to function with it” (Participant [P]10). Some participants pointed out that mental and cognitive symptoms appear immediately after a cancer diagnosis and later in the survivorship continuum: “[Patients] have memory problems; quite a few talk about it. . . . Years later they even claim that memory problems affect them” (P12). Others mentioned that “The psychological factors are very dominant; [patients] have depression, anxiety, and fear that leads . . . to limited daily functioning” (P24).
Although participants shared extensive knowledge of the side effects of cancer treatment, many could not share how these symptoms affect daily functioning, which is required for an occupational therapy referral. Even with the interviewer (Loubani) prompting, “In terms of function, what do the patients say?” the participants had difficulties providing specific examples that tie symptoms to difficulties in daily functioning: [Neuropathy] complaints always [arise] even after finishing the treatments; there are some who have it for a long time in the palms of their hands and feet. Sometimes there are sensation problems that are related to nerve damage [and] hair loss during the treatments. These complaints are many. (P22)
A few participants did demonstrate good knowledge with regard to how the side effects cause “difficulty managing the household, cooking, cleaning the house, everything related to housekeeping, complaints about hand numbness, which is very limiting . . . [difficulty] buttoning buttons of shirts or pants, which requires finger movements” (P24); however, this knowledge was not sufficient to refer patients to occupational therapy.
Gaps in Knowledge Regarding Occupational Therapy’s Role in Cancer Care
Participants expressed gaps in knowledge regarding the scope of occupational therapy practice in cancer care. We coded data regarding gaps in knowledge in three different categories: (1) complete lack of knowledge, (2) minimal knowledge, and (3) partial knowledge.
Several participants expressed a lack of knowledge about occupational therapy as a profession and occupational therapy’s specific role in cancer care, as well as the difference between occupational therapy and other rehabilitation professionals: “Is occupational therapy a profession? Do you have a license from the Ministry of Health (MOH)?” (P23). One participant said, with regard to interdisciplinary cancer care teams, “One hundred percent, they don’t know what you [occupational therapists] actually do” (P22). Participants wanted to understand what conditions [occupational therapists can] treat . . . that’s the most basic thing [we need]. Except for neuropathy, tell us a little what your main work is, like characteristics, main things, principles . . . because I do not think many people know what the work of [occupational therapists] is. (P10)
However, participants were open to knowing more about the role of occupational therapy and shared their need and desire to gain greater knowledge to properly refer patients: “I would also be happy to know how you can contribute to them” (P7).
Some participants expressed minimal knowledge, indicating that they had very basic or limited knowledge of the side effects of cancer treatment related to occupational therapy: An [occupational therapist] came to visit one of my patients at home, I don’t know . . . but [the patient] was a bit disabled. . . . There was someone who came to help her [relearn] how to cook. . . . I think it was an [occupational therapist]. (P26)
Other participants showed partial knowledge of occupational therapists’ work with PLWBC. They provided either general or missing information regarding our work, such as “Functional problems related to organization [cognition], that relate to functioning, to fine motor skills . . . what else . . . and I also know about [occupational therapy] in-home care” (P5). Another participant was not able to elaborate on occupational therapy’s scope of practice for various clients or areas: “In the burns unit [occupational therapists] were really involved in the practice” (P22). One participant shared that she had gained knowledge of occupational therapy “through a patient, who desperately wanted to ride a motorcycle again and learn driving . . . [the occupational therapists] worked with him to return his license” (P7).
Bureaucratic and Organizational Barriers
This theme encompassed procedural or policy issues related to the referral process to occupational therapy. Issues were identified at the national, organizational, and individual professional levels.
At the national level, occupational therapists’ involvement in cancer care was not emphasized and shared with other professions. In Israel, “the cancer care nurses can refer patients. . . . It’s a project of the [MOH] to give permission to nurses in the cancer care clinics for more advanced activities, such as referrals” (P4). However, when the MOH gave the mandate to refer PLWBC to other specialists, occupational therapy was not listed as one of these professions. One participant suggested that “as soon as [occupational therapy] is exposed, through the Israeli cancer association, that is, at a national [level], we will see that there is [more] demand and referrals” (P10). At the organizational level, “I see more problem[s] with the [organization] procedure” (P26); another participant added, “You may need a medical referral . . . and who the referral is from?! Obviously not from me. It’s only through the family doctor or an oncologist” (P24). At the individual level, participants mentioned that “[The] doctors, in my opinion, are the biggest barrier because they don’t deal with [functional difficulties]” (P10) and that the referral process “should be easier. . . . Nurses see the patients much more than doctors and know more about their function than doctors” (P26). The participants shared that they heavily focus on the side effects and medical aspects of care rather than on function and quality of life of PLWBC. They mentioned that asking specific questions of patients is meant “to understand what the symptoms are in order to balance them if there is anything unusual” (P22); however, these questions do not focus on daily activities or function.
Unavailability of Occupational Therapy Services
Lack of occupational therapy availability was identified as a barrier; participants discussed issues related to difficulty finding occupational therapy services to refer patients to and their organization’s lack connection to or availability of occupational therapy staff. They generally reported that occupational therapists were not present in cancer care. Even though the interdisciplinary teams included many other specialists, occupational therapists were neither physically present nor in the minds of the participants, which resulted in a lack of awareness: The [occupational therapy] service is not an in-house service at the cancer care department. Our services include a doctor, nurses, social workers, dietitian, secretary, physical therapists, and complementary therapists. . . . I really ask myself why no [occupational therapist] is there?! What should I do in case I believe it is necessary to involve an [occupational therapist]? (P24)
Participants expressed the lack of occupational therapy services within departments and a low number of practitioners as barriers to referrals. Most of them wondered, “Do we have enough [occupational therapists] in the hospital? I have not met any [occupational therapists] in the hospital” (P4). Participants also shared that the lack of occupational therapy availability causes inconvenience for the patients, who will have to travel to a faraway place; in addition, “Patients who are often treated by [occupational therapists] say that their appointments are like three months away” (P6). Concerns were raised about the lack of occupational therapy hours compared with the number of patients requiring future referrals: “We have dozens of patients to refer, but who will treat them?” (P4).
Theme 2: Partial Facilitators of Occupational Therapy Referral
Compared with barriers, only a few facilitating factors were uncovered. Participants mentioned issues related to communication and collaboration with occupational therapy and awareness of occupational therapy services in cancer care.
Collaborations and Communication With Occupational Therapists
This theme included in-person and ongoing communication between cancer health care professionals and occupational therapists through interdisciplinary meetings and presentations given by occupational therapists. Throughout this subtheme, participants shared interactions with occupational therapists at the interdisciplinary level, allowing for a better understanding of occupational therapy’s role. Participants also expressed how increased communication and collaboration facilitated knowledge and understanding of when a referral to occupational therapy was appropriate: Since the last 4 to 5 years we have been doing multidisciplinary meetings, including the participation of an [occupational therapist] within the meeting, talking about the patients. We introduce the patients and there are lots of things that we have discovered thanks to this process. This can help, and that it is very good for the patients. By the way, we already refer patients to rehabilitation. . . . We refer while [the patients] are undergoing treatments. It was created because of the collaboration with the occupational therapist and physiotherapy. (P5)
Awareness of Occupational Therapy Services
Awareness of occupational therapy as a profession and an understanding of the services occupational therapists provide was a subtheme that partially supported occupational therapy referrals. Some participants were able to provide clear, good examples of what occupational therapists do in cancer care and their contribution as part of the cancer health care team. These examples provided some evidence of support for referrals to occupational therapy: When [the occupational therapist] helps the patient, it also helps me. If the patient is frustrated by the functional decline, [the occupational therapist] can take her to a completely different place. If for a 60-year-old housewife the most important thing is cooking for the grandchildren, that’s what’s meaningful to her, I don’t have the knowledge to help her with that. And if I refer her to [occupational therapy] and she begins to feel an improvement in daily functioning, we can start talking together about other things, such as emotional issues, improving quality of life, and positive thoughts, but when she is stuck in daily functioning, she really gets stuck. (P24)
We created a visual logic diagram to capture the interrelations of the themes and subthemes and interconnection to occupational therapy referral in cancer care (Figure 1). Overall, barriers to occupational therapy referrals outweighed the partial facilitators.
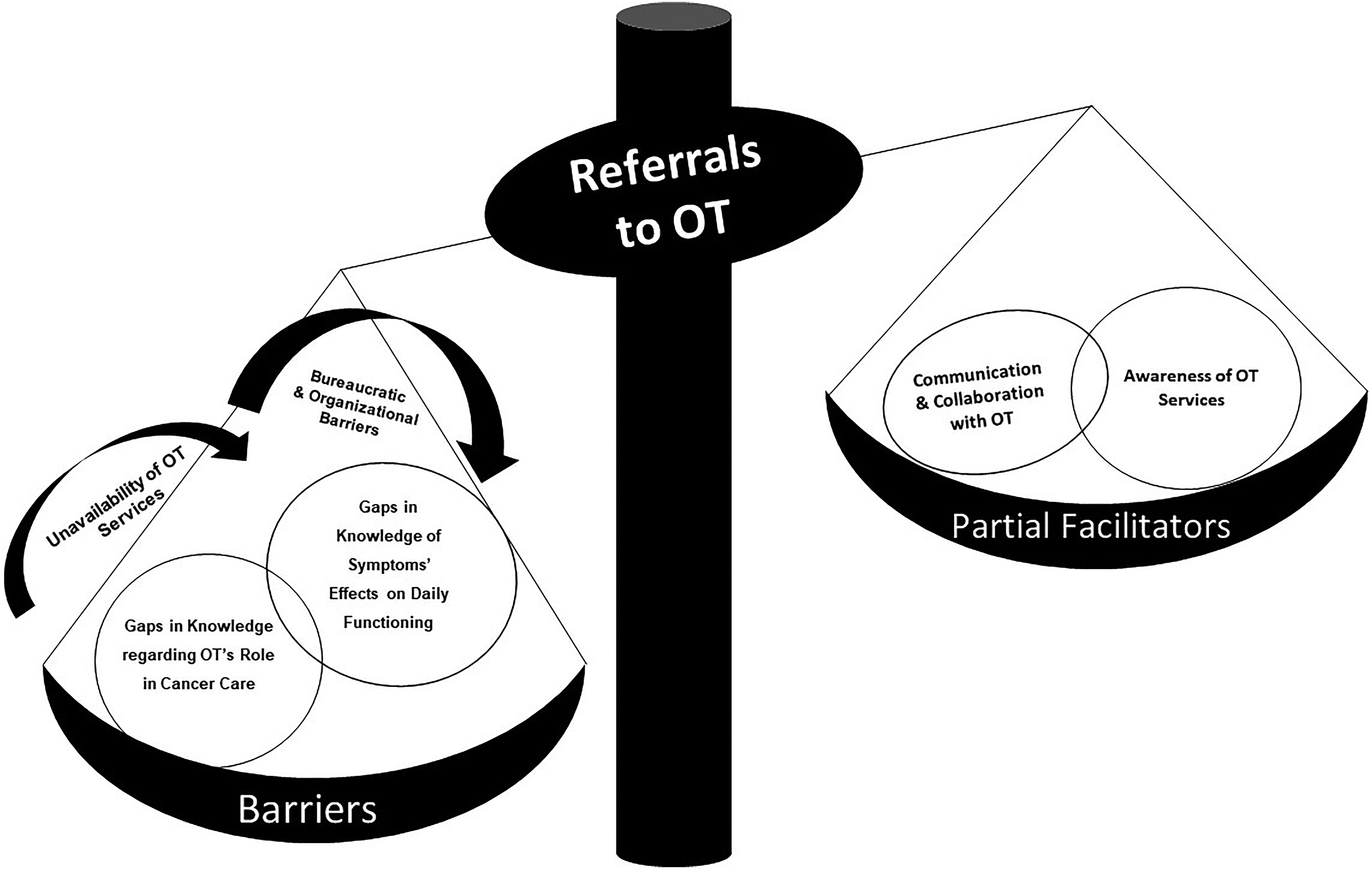
Logic diagram of the study results describing the barriers to and partial facilitators of occupational therapy referral in cancer care.
Suggestions to Address the Barriers and Optimize Occupational Therapy Referrals
Participants expressed a need for more information about occupational therapy’s role and suggested practical solutions to address the barriers and optimize the referral process. The suggestions for improving referrals, based on the main barriers we found, are summarized in Table 3.
Participant Suggestions for Addressing Barriers and Improving Referrals
Note. OT = occupational therapy/occupational therapist; PLWBC = persons living with and beyond cancer.
Discussion
This study was Phase 1 of a larger multiphase international collaboration between Israeli and American occupational therapy researchers. Our aim is to understand the barriers and facilitators identified by Israeli cancer health care professionals with regard to referring PLWBC to occupational therapy. Four subthemes related to barriers emerged, and two subthemes regarding facilitators to occupational therapy referral were noted. Although participants identified facilitators for occupational therapy referrals, these did not outweigh the barriers. Therefore, we defined facilitators as partial and included communication and collaboration with occupational therapy professionals and participants’ awareness of occupational therapy services in cancer care. To overcome the barriers that were identified, participants offered many practical suggestions and ideas for how to improve referrals to occupational therapy services in cancer care. These broad suggestions could be internationally considered for implementation by interdisciplinary cancer care teams, including cancer care nurses, to improve occupational therapy referrals and reduce gaps in care.
The dominant theme we uncovered is the lack of knowledge about occupational therapists’ scope of practice and role in cancer care. This theme supports evidence, observations, and statements from other researchers (Ellen et al., 2021; Pergolotti et al., 2016; Sleight et al., 2022). It provides a foundation for understanding the low referral rates to occupational therapy services. In addition, the lack of knowledge about services is a barrier that hinders referrals to rehabilitation, including occupational therapy (Cheville & Tchou, 2007; Cheville et al., 2011). Participants expressed good knowledge of the symptoms of cancer that affect daily functioning; however, they could not connect the symptoms to performance issues that indicate a need for occupational therapy referrals. This also highlights the importance of a holistic perspective, such as identifying functional needs to accurately refer patients to rehabilitation services, including integrating occupational therapists as part of cancer care teams (Cheville et al., 2011; Stout et al., 2021). These findings are problematic because performance issues, and the knowledge of occupational therapy practitioners’ role in cancer care, are key to understanding whether an occupational therapy referral is needed. Participants did share solutions, including a need for written materials, lectures, and further information about how to identify daily activities that indicate a need for an occupational therapy referral. They also suggested that, to improve referrals, more occupational therapy practitioners increase their collaborations with interdisciplinary cancer care professionals.
Facilitators of referral were raised by a few participants; specifically, nurses and social workers who had past communication or collaborations with occupational therapy services shared more awareness of occupational therapy practitioners’ role in and potential contribution to cancer care. However, these facilitators were considered partial because they were inconsistent among participants, and most did not result in routine referrals to occupational therapy services. The solution of having occupational therapy present with interdisciplinary interaction was validated in the partial-facilitators-of-occupational-therapy-referrals theme. Moreover, the participants with knowledge of occupational therapy were able to provide better examples of how occupational therapy can contribute to cancer care and the importance of their role as part of a health care team.
We also found that occupational therapy referrals were negatively impacted by participants who did not report previous collaborations with occupational therapy practitioners, and those participants had a limited understanding of occupational therapy practitioners’ role in cancer care. This is supported by existing literature (Mackenzie, 2021). Collaboration between the interdisciplinary cancer care and rehabilitation teams is essential and is recommended as a health services agenda to integrate cancer rehabilitation services into standard cancer care (Söderback & Paulsson, 1997). However, we discovered that it is not enough to have knowledge, awareness, and education about occupational therapy practitioners’ role in cancer care at the level of the interdisciplinary team because the accessibility of occupational therapy services and other bureaucratic barriers affect referrals.
Participants shared that a lack of occupational therapy presence created two levels of barriers to referral. First, cancer care nurses and social workers expressed concern that occupational therapy practitioners are not currently present in cancer care departments, which could lead to a lack of referrals. This limits the ability to accurately screen patients for the need for occupational therapy services and can hinder an understanding of occupational therapy’s role in cancer care. Second, they expressed concern that occupational therapy practitioners do not have a strong presence in community or outpatient clinics, which could place an additional burden or stress on PLWBC. This finding was not surprising given that others have indicated that a lack of availability of rehabilitation services was a barrier to referrals. Some have called for rehabilitation practitioners to take a more active role in cancer care (Pergolotti et al., 2019; Stout et al., 2021). Participants in this study also suggested that occupational therapy practitioners should be present on the interdisciplinary cancer care team and be more present in outpatient and community settings once referrals have been identified. Occupational therapy practitioners are in a unique position to identify and address the needs of PLWBC on the basis of their expertise and focus on occupational performance, participation, and engagement. Therefore, they should advocate for their inclusion in interdisciplinary teams (Morikawa & Amanat, 2022).
According to the summative results of this study, knowledge and cooperation at the personal level with occupational therapy practitioners is not sufficient because of the many bureaucratic barriers that are preventing adequate occupational therapy referrals. The barriers identified by our participants need to be addressed on many levels. They discussed how, although doctors have the power to be the main source of occupational therapy referrals, they often have limited time to screen for patients’ functional issues. Participants also expressed the need to advocate at the national level with the Israeli MOH for a mandate that would allow for the direct ordering of supportive rehabilitation services such as occupational therapy.
Alongside individual barriers, participants expressed barriers at the organizational level preventing referrals. They stated that, within medical institutions, and specifically in cancer care departments, the referral process needs to be clear, including specific guidelines regarding who, how, and where to refer. Such barriers can be addressed by providing cancer care professionals with specific criteria indicative of an occupational therapy referral (Pergolotti et al., 2018, 2019) or a screening tool (Stout et al., 2021) to determine the need for a referral.
Limitations
Study limitations exist. Because of the qualitative nature of this study, and the use of focus groups, some participants with opposing views might not have felt comfortable voicing differing opinions (Corbin & Strauss, 2014). In addition, purposeful sampling was used from one large health care system in Israel. These limitations may reduce the transferability of results to other organizations and to oncology physicians. Further research and clinical work are needed to fill gaps in health care delivery for PLWBC, demonstrate the contribution of occupational therapy to this field, contribute to achieving enhanced daily participation and quality of life for PLWBC, and explore and overcome barriers to integrating occupational therapists into cancer rehabilitation in other health care settings.
Implications for Occupational Therapy Practice
This study supports the belief that the contributions of occupational therapy services to symptom management, participation in daily activities, and quality of life in cancer care are poorly understood by cancer health care professionals. A better understanding of barriers and facilitators related to knowledge and understanding of occupational therapy, as well as context related to barriers and facilitators, would contribute to minimizing gaps in referrals of PLWBC to occupational therapy services. Several implications for occupational therapy practice arise from this study; specifically, the participants offered suggestions to overcoming barriers and maximizing support for occupational therapy referrals in cancer care that could be implemented and used by occupational therapy practitioners: ▪ Occupational therapy practice would benefit from increasing awareness in cancer clinics regarding occupational therapy services, including sharing professional marketing tools and providing educational opportunities to enhance an understanding of the profession’s scope of practice. ▪ Occupational therapists can use the practical solutions suggested by our participants to improve referrals to occupational therapy services. This could be achieved through intentional collaboration with referral sources and cancer care centers and by developing screening tools and resources to facilitate and guide proper referrals. ▪ The lack of available occupational therapy services in cancer care is a significant barrier that occupational therapy practitioners must address by advocating at the organizational and policy levels to develop and adopt procedures for regular screenings for their services as a standard in cancer care plans across practice settings (i.e., hospitals, outpatient clinics, community).
Conclusion
Cancer care nurses and social workers expressed gaps in their knowledge about the link between side effect symptoms of PLWBC and functional difficulties and thus did not understand the need to refer patients to occupational therapy services. The limited referrals of PLWBC to occupational therapy services might also be explained by the fact that occupational therapy’s role in cancer care is poorly understood and services are not readily available. Occupational therapy practitioners can implement the strategies suggested by our participants to help overcome referral barriers, contributing to a reduction in the unmet needs of PLWBC.
Footnotes
Acknowledgments
We acknowledge the cancer care teams at Clalit Health services for their time, interest, and thoughtful insights into the study. We also thank chief occupational therapists Pnina Weiss, PhD, OT; Sharon Kirshner, PhD, OT; and Anat Cons, OT, for their assistance with initial participant connection. We also appreciate Naomi Schreuer, PhD, OT, for her expert review of our interview guide.