
Abstract
This study explored implementing evidence-based practice (EBP) and its relationships to burnout and work-related self-efficacy among occupational therapists.
Evidence-based practice (EBP) denotes the use of the best evidence from research combined with the therapist’s expertise and the client’s preferences and values (Brown, 2017; Sackett, 2000; Thyer & Myers, 2011). Implementing EBP is essential for ensuring optimal quality care and obtaining positive outcome in treatment (Brown, 2017; Sackett, 2000; Thyer & Myers, 2011). The level of research evidence is based on the methodological quality of the study design, validity, and applicability to patient care (Ackley et al., 2008). Randomized controlled trials and, especially, systematic reviews and meta-analysis of several randomized controlled trials are considered the best evidence, but other experimental design studies can help guide clinical practice. Under conditions when sufficient research evidence is obtained, the practice should be guided by it in conjunction with clinical expertise and patient values.
Although occupational therapists and other health care practitioners think EBP is important, they do not always have the information and support needed to fully implement it (Krueger et al., 2020; Upton et al., 2014).
Potential barriers to implementing EBP consist of personal and environmental factors (Weng et al., 2013). These include time constraints, organizational barriers, the high costs of professional courses, and therapists’ perceptions that research is mostly theoretical (Dysart & Tomlin, 2002; Upton et al., 2014). Lack of clarity regarding EBP implementation—as well as lack of training, skills, and knowledge—and low motivation pose additional challenges for therapists that may preclude them from implementing EBP (Marr, 2017; Munce et al., 2017; Snibsøer et al., 2017; Yost et al., 2014). In a recent study, the importance of evidence and tools in assessing EBP implementation has arguably been overshadowed by discussion about how to teach and practice it. The study emphasizes that merely instructing students on the procedural steps of EBP implementation is insufficient (Thomas et al., 2021).
Implementing EBP appears to benefit not only clients but also health care practitioners themselves, because it has been found to be related to their burnout and self-efficacy (Abrahamson et al., 2013; Gómez- Urquiza et al., 2017; Maslach & Jackson, 1981), which are the focus of the present research.
Burnout syndrome is characterized by three main dimensions: emotional exhaustion, depersonalization manifested in the health care practitioner’s negative and cynical attitudes toward others, and low personal accomplishment manifested in the health care practitioner’s negative self-evaluation and inability to feel fulfilled in their job (Gómez-Urquiza et al., 2017; Maslach & Jackson, 1981). Burnout can negatively affect both the quality and the effectiveness of the care provided and may have serious implications for practitioners, clients, and health care organizations. These include elevated rates of patient complaints, lower effectiveness, poorer treatment outcomes, staff absenteeism, and lower staff retention (AbuAlrub & Al-Zaru, 2008; Garcia et al., 2019; Shin et al., 2022).
Previous studies on EBP implementation and burnout among therapists have indicated a link between the two. For example, a study conducted among clinicians who work in university counseling centers revealed that health care practitioners who implement EBP daily were less burned out than those who did not report implementing EBP (Wilkinson et al., 2017). Similarly, a study conducted among physical therapists in Spain found that an improved attitude toward EBP was associated with less burnout and suggested that EBP may improve therapists’ sense of mastery and personal accomplishment (Rodríguez-Nogueira et al., 2021).
Nonetheless, to the best of our knowledge, no research to date has explored the relationship between EBP implementation and burnout among occupational therapists. Therefore, it is unclear whether these relations are applicable for this population, as found for other health practitioners. Furthermore, previous studies have not investigated the processes at the basis of the relationship between EBP implementation and burnout. Therefore, the mechanisms underlying these relationships are unknown.
Work-related self-efficacy may serve as such a mechanism, underlying the relation between EBP implementation and burnout. Work-related self-efficacy refers to one’s belief that one is capable of handling tasks and challenges related to their clinical practice (Wood & Bandura, 1989). This belief shapes therapists’ experience and performance as well as their ability to cope with changes and challenges in their work environment (Schaubroeck & Merritt, 1997; Stajkovic & Luthans, 1998).
Among health care professionals, higher levels of EBP implementation were correlated with higher levels of self-efficacy, which has been supported by large and heterogeneous studies (Abrahamson et al., 2013; Weng et al., 2013). Whereas Abrahamson et al. (2013) suggested that this relationship reflected the effects of self-efficacy on EBP implementation, one might offer the inverse explanation, according to which EBP implementation enhances knowledge, confidence, and treatment success and thereby boosts therapists’ self-efficacy. Furthermore, given the documented relationship between self-efficacy and low burnout (Abaoğlu et al., 2021; Shoji et al., 2016), it might be that the elevated self-efficacy that stems from EBP implementation could, in turn, contribute to low levels of burnout.
In this study, we aimed to fill the knowledge gap and explore this supposition by assessing the role of self-efficacy in the relationship between EBP implementation and burnout among occupational therapists. Being the first, to our knowledge, to address this topic among occupational therapists, we set three main objectives: to describe EBP implementation, burnout, and self-efficacy among occupational therapists; to assess correlations between EBP implementation, burnout, and self-efficacy; and to assess the mediating role of health care practitioners’ self-efficacy in the relationship between EBP implementation and burnout.
Method
Participants and Procedure
We conducted a cross-sectional study using an online survey to include a large sample of Israeli occupational therapists. Inclusion criteria were as follows: Participants had to be (1) licensed occupational therapists, (2) with at least 1 year of clinical experience, and (3) who were not absent from work for more than a year (after vacation or illness). Our survey was sent by email to university graduates and posted on all relevant social network groups. The survey was accessible through Qualtrics, a secured web-based survey data collection system. The survey took approximately 25 min to complete and was open from December 23, 2020, to March 14, 2021. The survey was anonymous, and no data were collected that linked participants to recruitment sources. The university institutional review board approved all procedures and instruments. Clicking on the link to the survey guided potential respondents to information regarding the purpose of the study, the nature of the questions, and a consent form (i.e., the survey was voluntary; respondents could quit at any time, and responses would be anonymous). The first page also provided the researchers’ contact information.
A total of 268 participants took part in the survey. Overall, 0% to 17.2% of data were missing across variables. To decide whether the data had missing values in a random pattern, we analyzed the differences between participants with missing values and those without missing values in all of the variables, using Little’s Missing Completely at Random (Collins et al., 2001) test. The analysis revealed that the data were missing completely at random and lacked pattern bias, χ2(3114) = 1,391.96, p = 1.00. Nevertheless, we decided to use the more advanced method of maximum likelihood (ML) via IBM SPSS Statistics (Version 27; Collins et al., 2001; Schafer & Graham, 2002). Compared with the conventional methods, such as the arithmetic mean or the listwise or pairwise deletion, the ML method was recommended as an optimal method for attrition (Collins et al., 2001). Given that only 7 participants (2.6%) were men, these participants were not included in the present study. Thus, the final sample consisted of 261 female occupational therapists. A power calculation using G*Power (Version 3.1.9.7) indicated a sample size of 55 participants, for a medium effect size (f 2 = 0.15), an α error of .05, and power of .8. Given that the mediating role of self-efficacy was determined by using the bootstrapping procedure, we also adopted a Monte Carlo simulation approach for power analysis, as suggested by Schoemann et al. (2017). The analysis derived a sample size of 136 observations for a power of .8, in a 1,000-replicate procedure, given the estimates of the correlation coefficients from our data.
Measures
Participants completed a brief demographic questionnaire assessing age, marital status, level of education, clinical experience (seniority and student supervision), and field.
We used the EBP Implementation Scale (Melnyk et al., 2008) to assess the implementation of evidence-based interventions. This questionnaire includes 18 items, with each statement rated on a 5-point Likert scale regarding how often it was performed during the past 8 wk; the scores range from 0 (never) to 4 (eight times). The total scores range between 0 and 72 points; higher scores indicate greater EBP implementation. This questionnaire has very good internal reliability (Cronbach’s α = .96; Melnyk et al., 2008). This study found good internal reliability (Cronbach’s α = .87).
We used the Maslach Burnout Inventory (Maslach & Jackson, 1981 [Hebrew version: Chayu & Kreitler, 2011]) to assess burnout. This questionnaire includes 22 items that measure burnout on three subscales: Emotional Exhaustion, Depersonalization, and Personal Accomplishment. Each statement is rated for frequency on a scale ranging from 1 (a few times a year or less) to 6 (every day). Intensity is rated on a scale ranging from 1 (very mild, barely noticeable) to 7 (major, very strong). A high degree of burnout is characterized by a high score on emotional exhaustion and depersonalization, and a low score on personal accomplishment. The overall score (1–6 for frequency and 1–7 for intensity) is calculated as the mean score after the personal accomplishment scores are reversed (Maslach & Jackson, 1981). The internal reliability of this questionnaire is high (Cronbach’s α = .86–.90; Chayu & Kreitler, 2011; Stav et al., 1987). This study found very good internal reliability for the intensity and frequency scales (.86 and .85, respectively).
We used the Occupational Therapy Self-Efficacy Questionnaire (Berkovich, 2017 ; Derdall et al., 2002) to assess self-efficacy at work. This questionnaire assesses the level of confidence of occupational therapy students. We used the Hebrew version, which has been adapted for the use of occupational therapists (Berkovich, 2017). It includes 39 items, measuring self-efficacy in six areas related to clinical work: communication, adaptation, innovation, training, clinical work, and professional ability. Each item is rated on a 5-point Likert scale ranging from 1 (do not agree at all) to 5 (agree to a great extent); only the most appropriate option can be selected. An overall score is calculated by averaging the scores of all the statements. Higher scores indicate greater self-efficacy at work. The English version has excellent internal reliability (Cronbach’s α = .94; Derdall et al., 2002). This study found the scale to be highly homogeneous (Cronbach’s α = .96), similar to the excellent internal reliability reported previously for the Hebrew version (Cronbach’s α = .96; Berkovich, 2017).
Data Analysis
We used IBM SPSS Statistics (Version 27), and the PROCESS computational macro (Hayes, 2012) to analyze the data. To explore the relationships between EBP implementation, self-efficacy, and burnout, we conducted Pearson correlations. To assess the mediating role of self-efficacy in the relationship between EBP implementation and burnout, beyond background variables, we used a bootstrapping method with 1,000 bootstrap resamples in PROCESS (Model 4; Preacher & Hayes, 2008). Bootstrapping is a nonparametric method that generates an estimate of the indirect effect, including a 95% confidence interval (95% CI). When zero is not in the 95% confidence interval, one can conclude that the indirect effect is significantly different from zero at p < .05 (two-tailed). Thus, the effect of the independent variable (i.e., EBP implementation) on the dependent variable (i.e., burnout) is mediated by the proposed mediating variable (i.e., self-efficacy). Given that age, education, seniority, and student supervision have been previously associated with burnout (Ben-Porat & Itzhaky, 2011; Brewer & Shapard, 2004; Tartakovsky, 2016), these factors were treated as covariates in the mediation analyses. The scores for all variables were standardized.
Results
Table 1 shows the demographic characteristics and study variables of the sample. Participants’ ages ranged from 24 to 65 yr. The majority of them were married and had at least one child. Approximately half of the participants had a bachelor’s degree in occupational therapy. They had 1 to 40 yr of clinical experience, and most of the participants did not instruct students during their clinical placements. Participants worked in various clinical fields (pediatrics, physical rehabilitation/geriatrics, mental health, academia). Pediatrics was the most common field (53.46%). The type of clinical field was not associated with intensity or frequency of burnout (ps = .49 and .58, respectively).
Demographic Characteristics and Description of the Study’s Variables
Note. N = 261. Field variables reflect the domain in which the occupational therapist is engaged. EBP = evidence-based practice.
aBurnout frequency was rated on the Maslach Burnout Inventory from 1 (a few times a year or less) to 6 (every day).
bBurnout intensity was rated on the Maslach Burnout Inventory from 1 (very mild, barely noticeable) to 7 (major, very strong).
EBP Implementation, Self-Efficacy, and Burnout
Table 2 presents the intercorrelations between the study variables. As can be seen in Table 2, education and student supervision were associated with EBP implementation. Having at least a graduate degree and supervising students were associated with elevated levels of EBP implementation. Participants’ age was not associated with EBP implementation. Age, education, seniority, and student supervision were all found to be associated with intensity and frequency of burnout as well as with self-efficacy: Being older, having at least a graduate degree, having more years of experience as an occupational therapist, and supervising students were associated with lower levels of intensity and burnout frequency and elevated self-efficacy.
Pearson Coefficient Correlations (r) Between the Study Variables
Note. N = 261. EBP = evidence-based practice.
aSpearman correlation tests were used for this variable.
**p < .01. ***p < .001.
As shown in Table 2, there were significant negative correlations between EBP implementation and burnout: More EBP implementation was correlated with lower levels of burnout frequency (p < .001) and intensity (p < .001). We also found significant positive correlations between EBP implementation and self-efficacy (p < .001): More EBP implementation was correlated with elevated self-efficacy. In addition, we found significant correlations between self-efficacy and burnout (p < .001). Higher self-efficacy scores were correlated with lower burnout (Table 2).
EBP Implementation and Burnout: The Mediating Role of Self-Efficacy
To test the significance of self-efficacy mediation effect, we generated bootstrapped CIs around the indirect effects of EBP implementation on burnout from 5,000 resamples controlling for age, education, seniority, and student supervision. As shown in Table 3, analyses revealed that the indirect effects for self-efficacy were significant for both frequency (bootstrapped 95% CI of standardized effect [−.12221, −.0036]) and intensity (bootstrapped 95% CI of standardized effect [−.1079, −.0012]) of burnout. EBP implementation was related to higher levels of self-efficacy (p < .001), which, in turn, were associated with lower frequency (p < .001) and intensity of burnout (p < .001; Figure 1).
Standardized Regression Coefficients and Bootstrap 95% Confidence Intervals for Predicting Burnout by EBP Implementation Through Self-Efficacy
Note. N = 261. The 95% confidence intervals that do not include 0 (null association) are significant; age, education, seniority, and students’ supervision served as covariates.
*p < .05. ***p < .001.
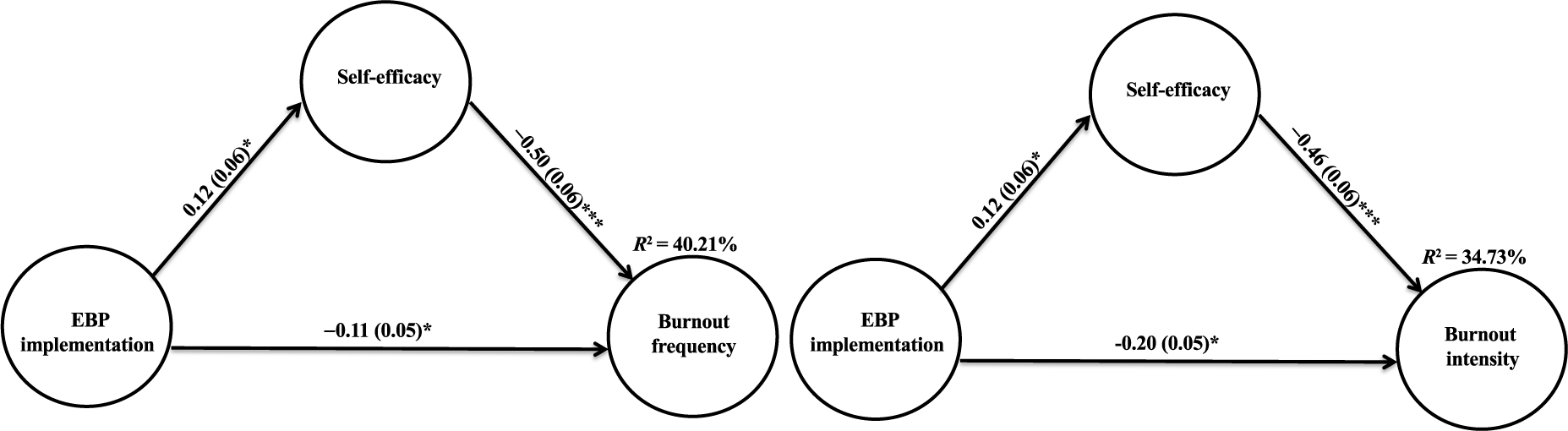
Self-efficacy as a mediator in the relationships between the implementation of evidence-based practice and the frequency (left) and intensity (right) of burnout.
Discussion
In this study, we aimed to advance our understanding of the relationship between EBP implementation and burnout among occupational therapists and to investigate the mediating role of self-efficacy in this relationship. Our results indicated a relationship between EBP implementation and levels of burnout (both frequency and intensity) among occupational therapists. Higher levels of EBP implementation were associated with the lower frequency and intensity of burnout. Moreover, self-efficacy mediated these relationships: EBP implementation was related to elevated self-efficacy, which, in turn, was associated with lower burnout.
Our sample of female occupational therapists was heterogeneous in terms of age and clinical field, which allowed us to examine EBP implementation, burnout, and self-efficacy. On the basis of the overall scores, occupational therapists who participated in this study reported moderate levels of burnout and high levels of self-efficacy. These trends are consistent with previous studies conducted among smaller samples of occupational therapists in Israel and around the world (Abaoğlu et al., 2021; Greaves et al., 2002; Gupta et al., 2012; Vax et al., 2012).
Occupational therapists who participated in this study had very low scores in EBP implementation. This trend has been documented in previous studies (Krueger et al., 2020; Snibsøer et al., 2017; Stokke et al., 2014) apart from one study that revealed high rates of EBP implementation, which were probably due to a unique sample of therapists who were particularly involved in EBP (Moore et al., 2018). Several explanations can be offered for the present findings. It may be that the low EBP implementation scores found in this study reflected little EBP utilization among occupational therapists. Barriers such as limited time to search for research evidence, limited resources (Juckett et al., 2020; Marr, 2017), the complexity of EBP, and a perceived gap between research and practice (Hallé et al., 2021) may have led to low levels of EBP implementation.
Alternatively, the limited understanding of EBP implementation among the occupational therapists who participated in this study may have contributed to the inadequate reporting of their actual implementation efforts. Previous studies have documented this phenomenon, indicating that health care practitioners may struggle with the question of whether their practices reflect EBP implementation (Munce et al., 2017; Snibsøer et al., 2017; Yost et al., 2014). Last, the present findings may result from the limitations of the measure used in this study to assess EBP implementation. In their study, Snibsøer et al. (2017) referred to the low results obtained by most of the participants and questioned a possible floor effect of some of the items in the EBP Implementation Scale. In other words, the low scores may be due to the difficulty in meeting the questionnaire’s standards (Snibsøer et al., 2017).
The present results indicated significant negative associations, with medium effect sizes, between EBP implementation and burnout; namely, higher levels of EBP implementation were associated with lower levels of burnout frequency and intensity. These findings, which are in line with those of former studies (Abrahamson et al., 2013; Wilkinson et al., 2017), may be rooted in several processes. According to the first explanation, burnout among therapists may negatively shape their levels of EBP implementation. It might be that therapists’ emotional exhaustion, and the depersonalization as part of their burnout (Gómez-Urquiza et al., 2017), limits their ability to implement EBP.
According to the second explanation, implementing EBP increases the chances that the health care practitioner experiences positive outcomes while treating patients, and this experience, in turn, may induce feelings of hopefulness and optimism, thereby limiting fatigue and burnout (Melnyk et al., 2010; Salyers et al., 2017; Skaggs et al., 2018). A third explanation, however, is that the relationship between EBP implementation and low burnout is rooted in good working conditions. According to this view, more time and resources at work both protect health care practitioners from burnout (Shin et al., 2022) and enable them to implement EBP. Last, a fourth explanation for the present findings is that health care practitioners who do not implement EBP might experience uncertainty when treating patients—a stressful experience that could put them at risk for burnout. Conversely, implementing EBP can enhance a sense of mastery and alleviate feelings of insecurity, limiting burnout (Iannello et al., 2017).
This explanation is supported by the present results, which indicate that self-efficacy significantly mediated the relationship between EBP implementation and burnout after adjusting for age, education, seniority, and student supervision: EBP implementation was related to elevated work-related self-efficacy, which was, in turn, associated with low burnout. The present findings imply that the unique qualities of EBP implementation may positively shape the experience of health care practitioners. Implementing EBP allows health care practitioners to search for existing knowledge; to apply it to different situations in their practice; and, therefore, to experience elevated self-efficacy—to feel self-assured and to believe in their capacity to handle tasks and challenges related to their clinical practice (Wood & Bandura, 1989). This belief, in turn, may serve as an important resource protecting health care practitioners against exhaustion, pessimism, and stress and, thus, may reduce burnout.
Limitations
The present findings should be considered in view of the study’s limitations. First, the possible implications of using convenience sampling should be taken into account. Although we distributed this survey to diverse groups of occupational therapists, our reliance on convenience sampling, along with the fact that that this study was conducted among Israeli female occupational therapists only, limits its generalizability. In Israel, all occupational therapists have bachelor’s degrees; therefore, future studies should assess occupational therapists with varying degrees of practice, which might affect EBP implementation. Second, although the study’s measures have good psychometric properties that are often used in the field (Derdall et al., 2002 ; Maslach & Jackson, 1981; Melnyk et al., 2008), the reliance on convenience sampling and self-report data may have led to response biases. Last, the study’s cross-sectional design precludes conclusions regarding the directionality of relations between the study variables. Therefore, longitudinal studies exploring the associations between EBP implementation, self-efficacy, and burnout among occupational therapists with varied cultural backgrounds are needed.
Despite these limitations, this study represents a step toward understanding the relationship between EBP implementation, self-efficacy, and burnout. Burnout is known to have devastating and comprehensive effects. These apply not only to the affected health care practitioners themselves but also to their patients, their colleagues, their workplace, and those who are close to them (AbuAlrub & Al-Zaru, 2008; Garcia et al., 2019; Shin et al., 2022).
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: ▪ The study sheds light on the relationship between EBP implementation, burnout, and self-efficacy among occupational therapists. The study’s results suggest that higher levels of EBP implementation are associated with lower levels of burnout and that self-efficacy plays a mediating role in this relationship. ▪ Occupational therapists should be encouraged to implement EBP in their practice as a possible means of reducing burnout and enhancing their self-efficacy. ▪ Incorporating EBP into occupational therapy education and training, creating guidelines and protocols for EBP, and providing resources and assistance to facilitate its implementation. ▪ Performing focus groups with occupational therapists to brainstorm how to better integrate EBP in clinical practice. Occupational therapy programs and organizations that provide training and resources should support EBP implementation. ▪ Health care administrators can perhaps leverage these findings to create supportive environments for EBP implementation. By providing resources, they can facilitate the integration of EBP into daily practice and enhance the well-being of occupational therapists while ensuring high-quality care for patients.
Conclusion
EBP implementation may serve as an important tool to limit burnout among occupational therapists by fostering their trust in their ability to handle clinical challenges. More research is needed. Future longitudinal studies, further illuminating the processes underlying the relationship between EBP implementation and burnout, are needed to promote using EBP-based strategies in occupational therapists’ workplaces to limit burnout.
Acknowledgments
This work was performed in partial fulfillment of the requirements for the Master of Science in occupational therapy degree by Tal Bar-Nizan at the Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. Yael Lahav and Debbie Rand declare equal contribution.