
Abstract
Occupational therapy based on the Comprehensive Environmental Questionnaire for older adults can improve health-related quality of life among community-dwelling older adults.
The World Health Organization (WHO) has predicted that the pace of population aging will continue to increase. In conjunction with global health resolutions, the WHO (2017) created a comprehensive global strategy and action plan on aging and health. This strategy and action plan has five strategic goals, one of which is “developing age-friendly environments” (WHO, 2017, para. 3). Age-friendly environments promote health, remove barriers, and can support those experiencing losses in capacity. The construction of such environments is being practiced even in Japan (Cabinet Office, 2018), which has a super-aging society, with more than 21% of the total population being people age 65 yr or older. However, the challenges are to continuously improve the physical environment, create a community, and promote social participation (Akita City, 2021). Occupational therapists are specialists involved in constructing age-friendly environments at either the individual or the small-group level. When an occupational therapist performs a comprehensive analysis of the quality and components that make up an environment, they can also clarify the impact of the environment, specifically its impact on the individual’s occupational performance and participation. Moreover, support can be offered to ensure that environmental changes are actually implemented, and the modified environment can be reevaluated for its impact on the individual (Fisher et al., 2017).
One benefit of environmental support for community-dwelling older adults was examined by Stark et al. (2017), who conducted a systematic review of the effects of home modification interventions. Most of the 36 studies targeted by that analysis were conducted by occupational therapists, who found that the main benefit of home modification was an improvement in functional performance, addressing issues such as frailty or functional disorders, care outcomes for those with dementia, and fall risk. In addition, Graff et al. (2006, 2007) conducted a randomized controlled study in which the effects of 5 wk of occupational therapy were examined among 135 pairs of older adults with dementia and their caregivers. The occupational therapist used both a compensatory strategy that adjusts the activities of daily living (ADLs) according to the target participant’s disability and as an environmental strategy that modifies their environment to accommodate their cognitive disorder. Significant improvements were observed in quality of life (QOL) and occupational performance skills among older adults with dementia, and these beneficial effects were maintained for 12 wk.
Studies of environmental support for community-dwelling older adults using occupational therapy have focused on the effects of interventions that modify the physical environment. However, the primary components of one’s environment include not only physical components (space and objects) but also social components (groups and occupational forms; Harrison et al., 2016), and few studies have comprehensively evaluated these environments and examined the effects of offering support in clinical trials. Meanwhile, with regard to comprehensive environmental support provided by occupational therapists to those living in care facilities, Fisher et al. (2014) developed the Residential Environment Impact Scale (REIS), and assessments of its utility for adults living in residential settings have begun (Svensson et al., 2018). However, the REIS is ot intended for use in community settings. As society moves toward the construction of age-friendly environments, occupational therapists must remember that to ensure that occupational therapy can proactively contribute to this process, they must comprehensively evaluate the unique environment surrounding community-dwelling older adults. Demonstrating the effects of these efforts on the basis of such evaluations in a clinical trial could establish supporting evidence for community-based occupational therapy that previous studies have lacked.
We conducted a randomized controlled trial (RCT) to clarify the effectiveness of occupational therapy– based comprehensive environmental support to improve the QOL of community-dwelling older adults in Japan.
Method
Trial Design
This study was a single-blind parallel-groups RCT with blinded participants and was conducted according to the Consolidated Standards of Reporting Trials (CONSORT) 2010 Statement (Schulz et al., 2010). The research protocol was reviewed by the Challenge Research Ethics Committee of the Japanese Association of Occupational Therapists (No. 2010-03).
Participants
The study was conducted in eight community-based settings under the long-term care insurance system in regional towns and cities throughout Japan. These community-based settings include adult day care centers, which primarily provide personal care and socialization opportunities, and adult day health care centers, which primarily provide rehabilitation services. In this study, we selected centers that provide occupational therapy. Services (including occupational therapy) were provided to older adults at least once a week. Participants were recruited between April 2011 and March 2012. All provided written informed consent before participating.
Inclusion criteria were as follows: age 65 yr or older, new users of adult day care or adult day health care in community-based settings cooperating with the trial, stable physical condition, and agreeing to participate in the study. Participants were excluded if they had major communication or cognitive deficits. Investigations were terminated for any participant who was unable to undergo occupational therapy at their day care or day health care center. The trial ended once follow-up for all participants was completed.
Environmental Assessment and Intervention
In this study, comprehensive environmental support refers to a novel method that supports factors that clients themselves are aware that they need, with a focus on physical, social, and institutional environmental factors considered important to Japanese older adults (Yabuwaki et al., 2007). The Comprehensive Environmental Questionnaire for older adults (CEQ; Yabuwaki et al., 2008) was used to evaluate what type of environmental support would be needed. The CEQ is based on a client-centered perspective and was developed in Japan to measure levels of satisfaction among community-dwelling older adults with regard to their environment. The questionnaire’s reliability, criterion-related validity, and construct validity have been reported (Yabuwaki et al., 2008). The CEQ consists of 14 items grouped into three factors (Secure Environment, Interactive Environment, and Family Environment). Figure 1 lists the CEQ items, each of which is scored on a four-point Likert scale (1 = not at all, 2 = a little, 3 = moderately, and 4 = very much). Specifically, clients are asked “to what extent are the environments in items 1–14 currently relevant to you?” and “which environmental factor is the priority item?” The questionnaire aims to identify any environmental factors that the client hopes to change in order to create a more satisfying life; providing the necessary support to meet this objective can help improve QOL among older adults.
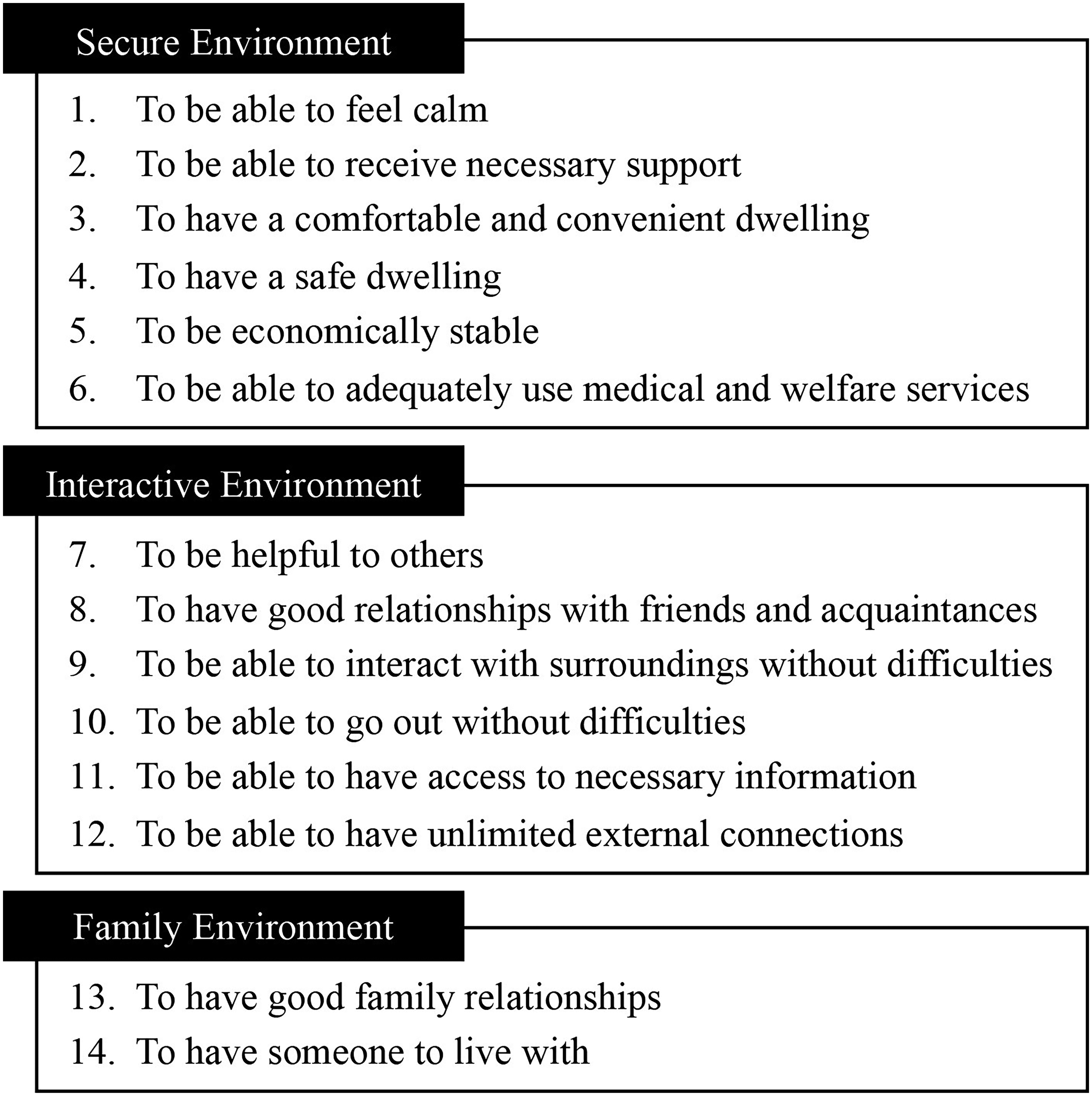
Items of the Comprehensive Environmental Questionnaire for older adults.
In the experimental group, the intervention involved providing CEQ-based comprehensive environmental support. We took 1 day to educate occupational therapists at each center on how to use the CEQ and offer comprehensive environmental support. Within the 1st wk after participants began using a new adult day care or adult day health care service, the occupational therapists administered the CEQ to identify up to three environmental factors that participants wanted to change to create a more satisfying life. The reasons why the participants wanted to change these environmental factors were confirmed, and the importance and urgency of each factor was discussed, considering other evaluation results as needed. On the basis of the results, the occupational therapist determined the intervention content from a client- centered perspective. Over the next 3 mo (1–4×/wk), occupational therapists offered participants support in making improvements in these environmental factors, collaborating with other professions as needed. For example, if a participant’s CEQ results indicated that they wanted to focus on being “able to go out without difficulties,” occupational therapists provided services to improve that environmental factor through home modification, effective use of transportation, and human support.
In Japan, the approach to occupational therapy in long-term care is centered on improving physical function via exercise therapy and improving ADLs. Accordingly, control group participants received the standard occupational therapy provided at the center for 3 mo, which included exercises considered necessary by an occupational therapist on the basis of assessments of physical and mental functions and ADLs. Because environmental support for the control group involved only modifications to the living environment to improve ADLs, their environmental support differed considerably from that provided to the experimental group, except when it was related to support “to have a comfortable and convenient dwelling” and “to have a safe dwelling” (i.e., CEQ Items 3 and 4). Occupational therapists offered support to improve participants’ physical function, ADLs, or both 1 to 4×/wk.
Outcome Measures
The primary outcome measure was score on the Japanese Medical Outcomes Study 36-Item Short-Form Health Survey (SF–36) at 3 mo postrandomization (Fukuhara, Bito, et al., 1998; Fukuhara, Ware, et al., 1998). The SF–36 is used to measure health- related QOL (HRQOL), and scores on eight domains (Physical Functioning [PF], Role–Physical [RP], Bodily Pain, General Health, Vitality, Social Functioning, Role–Emotional [RE], and Mental Health [MH]) and three component summaries (Physical Component Summary [PCS], Mental Component Summary, and Role/Social Component Summary [RCS]) are calculated using norm-based scoring. The reliability of the SF–36 has been confirmed on the basis of test–retest reliability and internal consistency, and the three- component model has been evaluated by equation modeling as valid (Suzukamo et al., 2011).
Additionally, the Short-Form Six-Dimension (SF–6D) health state utilities measure is a preference-based index derived from SF–36 data (Brazier et al., 2002). The Japanese version of the SF–6D has six domains: Physical Functioning, Role Limitations, Social Functioning, Pain, Mental Health, and Vitality (Brazier et al., 2009), with utility scores ranging from 0.29 to 1.00. In the present study, SF–6D utility scores were calculated by Qualitest, Inc. (https://www.qualitest.jp).
Secondary outcome measures were scores on the N geriatric rating scale for Activities of Daily Living (N–ADL; Nishimura et al., 1993) and the Life Satisfaction–100 (LS–100; Kobayashi & Miyamae, 2002), assessed 3 mo postrandomization. The N–ADL was set as a secondary outcome measure because the intervention with the control group aimed to improve ADLs. The LS–100 was set as a secondary outcome measure to assess the influence of the intervention on subjective QOL, a proximal concept of HRQOL. The N–ADL is used to measure ADLs of older adults on a scale ranging from 0 (lack of activity or response that requires total assistance) to 10 (independent). It is used to assess levels of dependency in five categories of self-care (gait–sitting, zone of life, dressing–bathing, eating, and excretion). The LS–100 is used to measure older adults’ state of life satisfaction. Participants are asked, “How many points is your life satisfaction now, if the most satisfying life is 100 points?” The participant’s oral response to this question is recorded as the life satisfaction score. The LS–100 is reportedly correlated with the Philadelphia Geriatric Center Morale Scale and is a useful evaluation method for older adults because vision is not required.
Sample Size
The effect sizes were 1.3 for QOL and 0.8 for health status, in reference to a previous clinical trial of community-based occupational therapy for older adults by Graff et al. (2007). We conducted a power analysis using G*Power Version 3.1.9.6 for Mac (Faul et al., 2009) and determined that a total sample size of 60 (30 in each group) would provide 80% power for detecting a difference with an effect size of 0.8 in HRQOL scores using a two-tailed test and an α level of .05, allowing for 15% attrition based on the clinical trial by Graff et al. (2007).
Randomization and Blinding
Participants were divided into blocks of those age 75 yr and older and those younger than 75 yr for stratified block randomization (block size = 4) because QOL and ADLs among older Japanese people are known to be affected by aging (Sato et al., 2002). An independent researcher who was not involved in the study carried out the randomization, and participants were then randomly allocated to either the experimental or the control group using sealed envelopes. In this manner, the allocation process was concealed. In this single-blind RCT, clients were blinded to group allocation, but the occupational therapists were aware of the treatment assigned. Assessors were also not blinded to group allocation. This is because there are only a few occupational therapists per community-based setting in Japan, and thus it was difficult to separate the individual providing the intervention and the assessor. Only one community-based setting had three occupational therapists involved in providing the intervention and assessments, whereas the remaining settings had only one occupational therapist.
Statistical Analyses
Primary and secondary effects were determined by analyses of covariance of the outcome measures (SF–36, SF–6D, N–ADL, and LS–100 at 3 mo) between the experimental and control groups, with posttest scores set as the outcome and pretest scores as a covariate (Van Breukelen, 2006). In this analysis, 1,000 bootstrap replicates were performed. All data were analyzed on the basis of an intention-to-treat analysis of all available data, applying the last-observation- carried-forward method for withdrawals. To compare with the allocation-focused results, per-protocol analysis, which excludes participants who dropped out of the protocol, was also carried out. Effect sizes (Hedges’s g; Hedges, 1981) were calculated by comparing the experimental group with the control group. The formula was as follows:
Standardized effect size is typically expressed as 0.2 for a small effect, 0.5 for a moderate effect, and 0.8 for a large effect (Cohen, 1988).
The numbers needed to treat with a 95% confidence interval (CI) were calculated. A clinically relevant improvement was defined as an improvement of 0.041 points in SF–6D score (Walters & Brazier, 2005). IBM SPSS Statistics (Version 27) was used for the analysis, and p < .05 (two-tailed) was considered statistically significant.
Results
The eligibility of 96 individuals from eight community- based settings was evaluated, and 60 were selected for inclusion in the study (Figure 2). Of the 36 excluded, 31 did not meet the inclusion criteria, 2 chose not to participate, and 3 discontinued using the center. The experimental group consisted of 29 individuals, but 1 dropped out of the study because of hospitalization. The control group consisted of 31 individuals, 2 of whom were hospitalized and 2 of whom dropped out because they either discontinued using the center or completed their rehabilitation services. Ultimately, data from 55 participants were included in the per-protocol analysis.
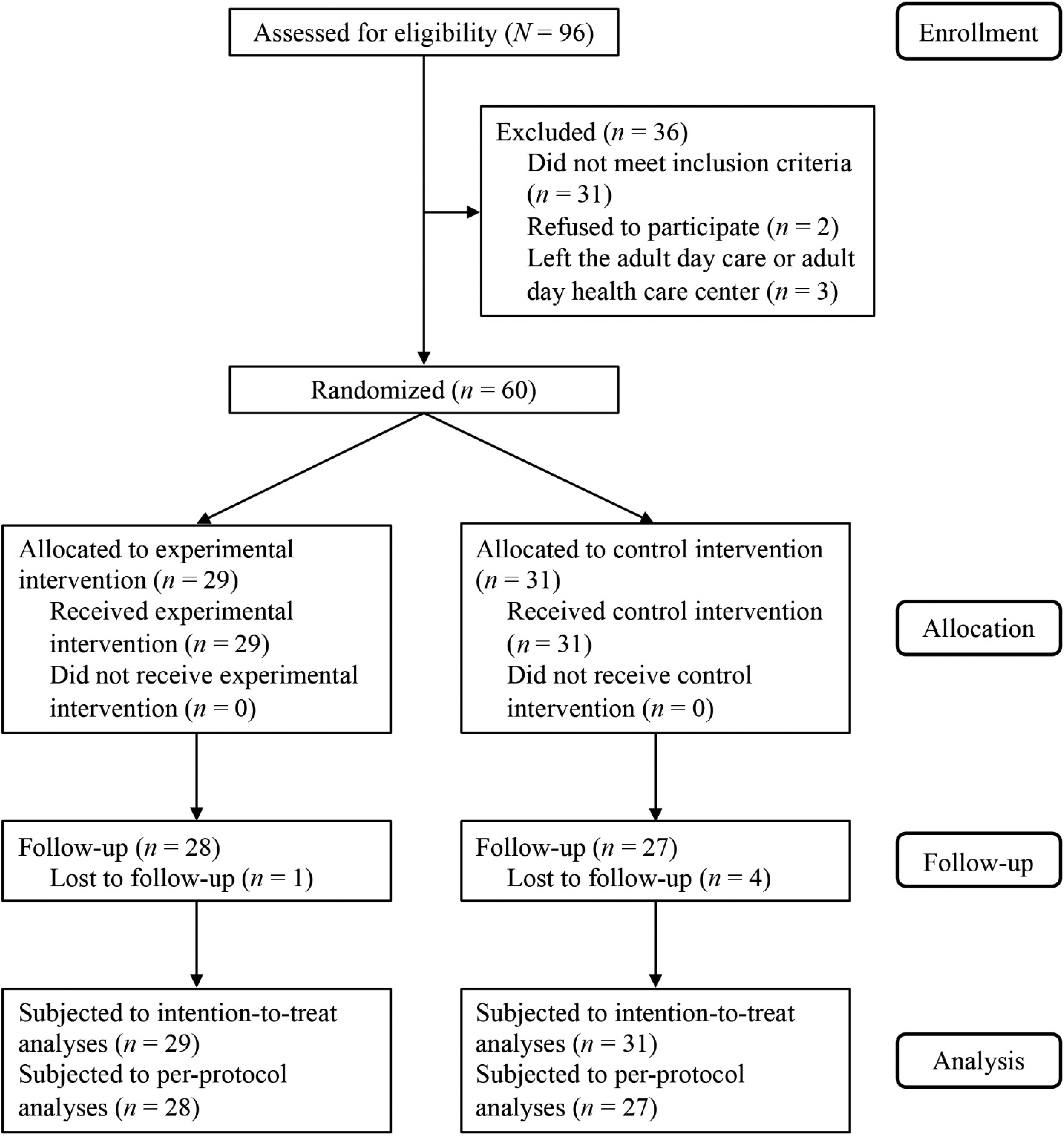
Flow diagram of participant selection.
Participant characteristics at baseline are shown in Table 1. In both groups, women and those living with family made up the majority. SF–36 scores showed marked declines in PCS, PF, and RP, with a mean SF–6D score of approximately 0.5. Meanwhile, scores on the LS–100 showed a slight group-dependent difference, with the control group exhibiting a slightly lower mean than that of the experimental group. However, no significant difference was found between the experimental and control groups for any of the baseline characteristics.
Baseline Characteristics of Participants
Note. LS–100 = Life Satisfaction–100; MCS = Mental Component Summary; N–ADL = N Geriatric Rating Scale for Activities of Daily Living; PCS = Physical Component Summary; RCS = Role/social Component Summary; SF–6D = Short-Form Six-Dimension; SF–36 = MOS 36-Item Short-Form Survey.
Comprehensive environmental support for the experimental group was provided according to CEQ results. The most common environmental component item for which support was provided was “To be able to go out without difficulties” (7 participants; 24%), followed by “To be helpful to others” (6 participants; 21%) and “To be able to interact with surroundings without difficulties” (6 participants; 21%). Each of these items was included in the Interactive Environment factor of the CEQ. Comparison by factors showed that support for Interactive Environment was the highest, with 21 participants (72%), followed by Secure Environment with 7 participants (24%) and “Family Environment” with 1 participant (3%).
The interventions provided to the experimental group included considering mobility options other than walking (for CEQ Item 10), preparing for a tea party with staff (for CEQ Item 7), and increasing opportunities for group activities when using services (for CEQ Item 9). The interventions for the control group, however, involved range-of-motion training and relaxation to reduce joint pain, outdoor walking and stair climbing practice to improve mobility, practice transferring between a wheelchair and toilet or lifting and lowering underwear for safe toilet activities, and adaptation of assistive technologies to safely perform bathing activities at home.
Analysis of covariance results for the intention- to-treat analysis are shown in Table 2. On the SF–36, which was the primary outcome measure, the experimental group showed significant improvements in RCS (p < .01), RP (p < .05), RE (p < .01), and MH (p < .05). We also noted significant improvements in the experimental group on the SF–6D (p < .05), with moderate effect sizes. No significant difference was observed on the N–ADL, the secondary outcome measure. We observed an interaction (p < .05) between group-dependent differences and baseline values of covariates and were thus unable to analyze the LS–100.
Comparison of Postintervention Outcomes Between Experimental and Control Groups
Note. Dash indicates not applicable. CI = confidence interval; LS–100 = Life Satisfaction–100; MCS = Mental Component Summary; N–ADL = N geriatric rating scale for Activities of Daily Living; PCS = Physical Component Summary; RCS = Role/Social Component Summary; SF–6D = Short-Form Six-Dimension; SF–36 = Medical Outcomes Survey 36-Item Short-Form Survey.
aAnalyses of covariance.
Hedges’s g effect size and 95% CI for the per- protocol analysis of SF–36 components were as follows: RCS, g = 0.73, 95% CI [0.19, 1.27]; RP, g = 0.64, 95% CI [0.10, 1.17]; RE, g = 0.68, 95% CI [0.14, 1.21]; and MH, g = 0.56, 95% CI [0.02, 1.08]. The SF–6D had an effect size g of 0.52, 95% CI [−0.01, −1.05]. These were all moderate effect sizes, with essentially no difference from the effect sizes in the intention-to-treat analysis (Table 2). There were 14 (48%) participants in the experimental group and 6 (19%) in the control group with clinically relevant improvements on the SF–6D. The number needed to treat for the SF–6D was 3.46, with a 95% CI [1.93, 16.60], showing statistical significance.
Discussion
With regard to occupational therapy for community-dwelling older adults, those who received 3 mo of comprehensive environmental support based on our CEQ results showed a significant improvement in HRQOL, based on the CEQ results, relative to those who received standard services. HRQOL items showing improvement were primarily those involved with roles, such as the RCS of the SF–36, although the experimental group’s utility scores on the SF–6D also showed significant improvements over the control group. Improvements in HRQOL and utility scores all showed moderate effect sizes.
In a systematic review by Berger et al. (2018) that examined the effects of occupational therapy on the QOL of community-dwelling older adults, group intervention and the combination of interventions for both the group and the individual were found to be effective, but the individual interventions were effective only when specific diseases were targeted, such as Type 2 diabetes or chronic obstructive pulmonary disease. In this study, when environmental support was offered on an individual basis, we found that HRQOL increased among older adults in general. Previous studies of QOL for community-based occupational therapy reported 3.1 as the number of patients who need to be treated to have an impact on one person among older adults with dementia (Graff et al., 2007), whereas 4.82 was the number needed for older adults in the general population (Yoshida et al., 2018), although the latter was not a significant result. Considering that the number needed to treat was 12 to 17 for an environmental intervention targeting fall prevention among older adults (Clemson et al., 2008), the 3.46 needed to treat in the present study demonstrates that comprehensive environmental support is an effective approach for community-dwelling older adults.
Most of our experimental group consisted of participants who received support for their interactive environment. Among older adults living in the community, in addition to support from spouses and children, support from friends and informal groups has been found to influence QOL (Gallardo-Peralta et al., 2018). Our environmental support enhances this type of social support and likely led to the observed increases in HRQOL. Moreover, the sense of isolation has increased among older adults receiving home care services because of the coronavirus disease 2019 pandemic and has further worsened because of their low sense of health (Johansson-Pajala et al., 2022); thus, support for the interactive environment among community-dwelling older adults is likely very important. Interventions that change the environment in order to ensure that these clients can lead satisfying daily lives represent a strategy similar to that of the compensatory model used in the intervention phase of the Occupational Therapy Intervention Process Model (Fisher & Marterella, 2019). The adaptation strategy of this compensatory model enables more efficient and safer task performance and is thought to increase the level of social participation. The fact that the RCS score for HRQOL showed marked improvements in the experimental group clearly demonstrates that client-centered environmental support using the CEQ can contribute to social participation.
The American Occupational Therapy Association (2020) defines environmental factors as an important construct that influences engagement and participation in occupations and includes many aspects of physical, social, and attitudinal surroundings. As such, it is not easy to comprehensively examine these factors in a community-based setting. The CEQ is characteristic in that it focuses on environmental factors that affect older adults’ QOL, which helps in gaining an understanding of their perceptions and identifying factors they hope to change to live a more satisfying life. By supporting improvement in such environmental factors, occupational therapy–based comprehensive environmental support, which led to changes in the MH score for HRQOL, clearly achieved client-centered practice in the present study.
Limitations and Future Research
This study has some limitations. First, the CEQ was administered as a premise of the intervention, but because the support offered was based on CEQ results, occupational therapists could not be blinded and were aware of the allocation. Except for one community-based setting, each center had only one occupational therapist who oversaw both the experimental group and the control group. We were also unable to ensure that our assessors were blinded. However, because the SF–36 (the primary outcome) is a self-report questionnaire and the assessors were essentially identical across both groups, we considered the effects of measurement bias, if any, to be negligible. Nonetheless, the occupational therapists and assessors not being blinded may have introduced contamination bias. In future studies, it will be important to use a method such as the stepped-wedge cluster randomized design, which minimizes such biases in settings in which blinding is difficult. Second, there was potential selection bias given that participants were limited to older adults new to the use of adult day care or adult day health care services, and our sample population did not represent all older adults receiving community-based occupational therapy.
In the future, we hope to conduct follow-up studies using a cluster randomized trial to examine the long-term and economic effects of CEQ-based comprehensive environmental support.
Implications for Occupational Therapy Practice
Our findings have the following implications for occupational therapy practice: ▪ Environmental support based on CEQ results can effectively improve HRQOL (e.g., support to promote an environment to go out without difficulties), particularly factors related to roles, among community-dwelling older adults. ▪ For community-based occupational therapy, applying the CEQ to older adults makes it possible to provide evidence-based practice focused on environmental factors. ▪ Support for the interactive environment promotes social support and participation among older adults, providing further evidence of increasing QOL.
Conclusion
By providing occupational therapy–based comprehensive environmental support to community-dwelling older adults in this RCT, we clarified the effectiveness of this approach by demonstrating that intervention group participants had moderate improvements in HRQOL. We also found that the CEQ is useful in determining environmental supports to provide to older adults. Our comparison of numbers needed to treat revealed this to be one of the more effective strategies among community-based occupational therapy methods. Our findings pave the way for the development of an effective compensatory intervention model in occupational therapy practice.
Footnotes
Acknowledgments
We thank all study participants and collaborators. This trial was supported by the challenge research grant program of the Japanese Association of Occupational Therapists (No. 2010–03) and was registered in the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (![]() ) with the identifier UMIN 000032305. Parts of this study were presented at the Asia Pacific Geriatrics Conference 2012, October 20–21, 2012, Hong Kong.
) with the identifier UMIN 000032305. Parts of this study were presented at the Asia Pacific Geriatrics Conference 2012, October 20–21, 2012, Hong Kong.