
Abstract
This systematic review adds to the evidence base indicating that occupation-based interventions have the potential to promote the occupational performance of older adults living in long-term care.
The relationship between engagement in meaningful occupations and well-being later in life is well documented (Jessen-Winge et al., 2018; Stav et al., 2012). Research has consistently demonstrated that performance of meaningful leisure, productive, and self-care occupations improves quality of life and thriving among long-term-care residents (Björk et al., 2017; Maenhout et al., 2020), including those with dementia (Chan et al., 2015). However, long-term-care residents experience decreased occupational engagement and choice (Uemura et al., 2018) and low satisfaction across a range of occupations they identify as important (Atwal et al., 2003). Studies have indicated that nursing home residents spend up to 85% to 92% of their time inactive (den Ouden et al., 2015; Hearle et al., 2012). Reduced occupational performance among long-term-care residents is associated with increased care burden and greater demands on health care and economic resources (Marincowitz et al., 2022; Sköldunger et al., 2019). Interventions to improve occupational performance in this population should be prioritized because they may not only improve residents’ quality of life but also have the potential to positively affect staff and quality of care.
Occupational therapy can improve functional and quality-of-life outcomes among older adults living in long-term care (Livingstone et al., 2022; Portillo et al., 2022). Yet, internationally, occupational therapy service provision in long-term care is low and highly variable (Meulenbroeks et al., 2022). Limited time, skills, and resources and organizational, health care, and funding structures mean occupational therapy practice in long-term care is frequently restricted and not evidence based (Calderone et al., 2022; Fletcher-Smith et al., 2014; Rafeedie et al., 2018).
Occupation-based interventions, as defined by Fisher (2013), use engagement in occupation as a treatment modality to achieve clients’ occupational goals. There is growing evidence showing positive effects of occupation-based interventions on occupational performance among a variety of client populations (Moon et al., 2022; Murad et al., 2016; Powell et al., 2016). Occupation-focused and occupation-based interventions can maintain and improve occupational performance, social participation, and quality of life among community-dwelling older adults (Nielsen et al., 2017). However, these findings may not be generalizable to long-term-care residents, who represent a unique population with complex needs (Pham et al., 2021). Portillo et al. (2022) found moderate evidence that occupational therapy interventions improved quality of life among healthy long-term-care residents. However, participants with chronic diseases, physical or cognitive impairments, or social problems were excluded, although the prevalence of dementia in long-term care ranges from 40% to 70% (Lepore et al., 2021). Therefore, this systematic review aims to extend findings from prior research through an explicit evaluation of the effectiveness of occupation-based interventions for improving occupational performance among older adults living in long-term care.
Method
This systematic review followed the Cochrane Collaboration methodology (Higgins et al., 2019) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). This review was preregistered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42023400711).
Literature Search and Study Selection
A systematic search was developed in consultation with a health research librarian. Search terms were designed using the PICO framework (patient/population, intervention, comparison, and outcomes) to capture studies evaluating occupation-based interventions for older adults living in long-term care and incorporating a measure of occupational performance (see Supplemental Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Relevant studies were retrieved from MEDLINE, CINAHL, PsycINFO, SCOPUS, Web of Science Core Collection, and the Cochrane Central Register of Controlled Trials (CENTRAL). Searches were limited to peer-reviewed research published in English from journal or database inception until February 2023. Reference lists of included articles and relevant systematic reviews were hand-searched for further articles eligible for inclusion.
Selection Criteria
Studies were included if they met the following criteria: (1) Participants were older adults (M age ≥ 65 yr) living in long-term care (also referred to as residential aged care, nursing home, care home, residential care); (2) the intervention delivered was occupation based according to Fisher (2013); (3) changes in occupational performance and participation were measured using subjective or objective standardized and validated assessment tools; and (4) the study was a controlled trial, quasi-experimental trial, crossover trial, or pilot clinical trial. Articles were excluded if they were not published in English; did not report quantitative data; or were dissertations, theses, abstracts, study protocols, reviews, or conference papers. See Supplemental Table A.2 for full selection criteria.
Articles identified during database searches were imported into EndNote and uploaded to Covidence software (Veritas Health Innovation, Melbourne, Victoria, Australia), and duplicate records were removed. All articles were independently screened by two authors (Rachael Mitterfellner and either Nathan M. D’Cunha or Stephen Isbel) via title and abstract and then by full text using predetermined selection criteria (see Supplemental Table A.2), with reasons for exclusion presented using a PRISMA flow diagram (Page et al., 2021). Differences were resolved by discussion or consultation with a third reviewer (either Isbel or D’Cunha, depending on who completed the initial screen).
Data Extraction
For each of the included studies, key data were extracted by one reviewer (Rachael Mitterfellner) into an evidence table and checked by a second reviewer (Nathan M. D’Cunha) for accuracy. Data included author, year of publication, level of evidence (Oxford Centre for Evidence-Based Medicine, 2009), location, sample size, participant characteristics, study design, intervention and control conditions, outcome measures, and results (see Supplemental Table A.3).
Quality Appraisal
The Cochrane Collaboration’s Risk of Bias tool (Higgins et al., 2016) was used independently by two researchers (Mitterfellner and either D’Cunha or Isbel) to assess the methodological quality of controlled trials, and the National Heart, Lung, and Blood Institute (2014) guidelines were used to assess noncontrolled (single-group) studies. Disagreements were resolved via discussion or by a third author (Isbel or D’Cunha).
Data Synthesis
The included studies were analyzed for commonalities and differences and grouped into themes in terms of intervention. Each theme was analyzed for strength of evidence, taking into consideration study design, findings, and risk of bias, using the U.S. Preventive Services Task Force (2018) guidelines.
Results
Study Selection
The initial database searches retrieved 1,444 articles, from which 537 duplicates were removed. Twelve additional articles were identified by searching reference lists of relevant systematic reviews and included articles. After title and abstract screening, 60 references remained for full-text review. Forty-three records were excluded, and 17 articles reporting on 16 studies met the inclusion criteria (see Figure 1).
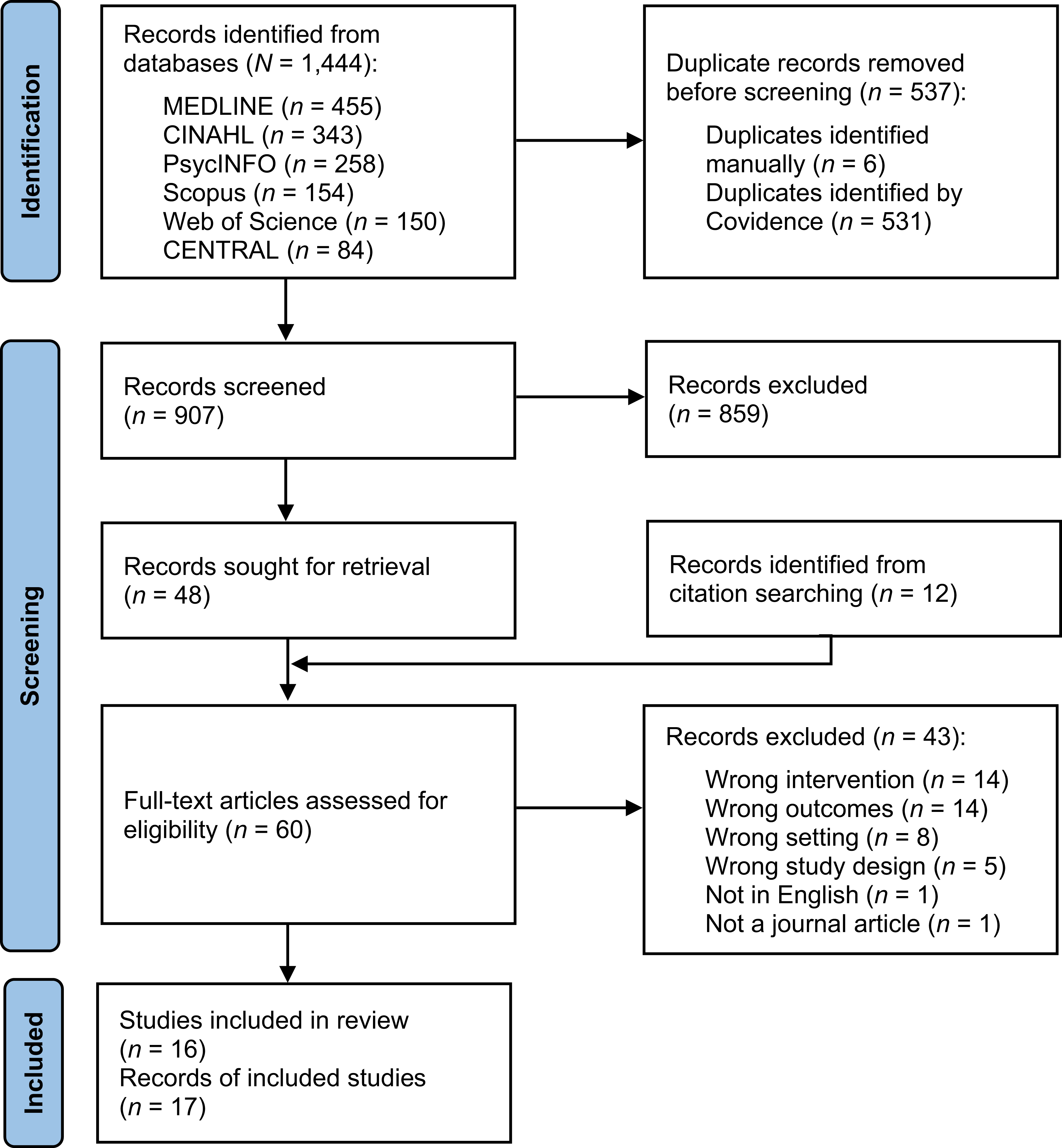
Flow of articles through the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) systematic review process.
Overview of Included Studies
The reviewed studies included 6 Level 1b randomized controlled trials (RCTs) in 7 articles (Brooker et al., 2011; Cichocki et al., 2015; Frändin et al., 2016; Grönstedt et al., 2013; Lam et al., 2010; Sackley et al., 2009, 2015), 5 Level 2b studies (Jung et al., 2018; Mozley et al., 2007; Nagayama et al., 2016; Przybylski et al., 1996; Sackley et al., 2006), and 5 Level 3b studies using quasi-experimental designs (Chard et al., 2009; De Vriendt et al., 2019; Fisher et al., 2007; Pozzi et al., 2020; Rogers et al., 1999; see Supplemental Table A.3). The study by Frändin et al. (2016) was a follow-up to a previous study also included in the review (Grönstedt et al., 2013); therefore, these studies were combined for the analysis. Meta-analysis was precluded by the heterogeneity of methods, measures, and resultant data across the included studies.
Included studies were published between 1996 and 2020 (Pozzi et al., 2020; Przybylski et al., 1996), with the largest number of studies conducted in the United Kingdom (n = 5). Two studies each were from Canada and the United States; 2 articles reported on a study completed across Sweden, Norway, and Denmark; and 1 study each was from Korea, Hong Kong, Japan, Austria, Italy, and Belgium. Eight of the studies were multicenter studies (Brooker et al., 2011; Cichocki et al., 2015; Frändin et al., 2016; Grönstedt et al., 2013; Nagayama et al., 2016; Rogers et al., 1999; Sackley et al., 2006, 2009, 2015).
Setting and Participants
A total of 2,974 participants were included across the reviewed studies, with a mean age of 83.8 yr (median age = 84.2 yr; range = 44–102), and, overall, 2,138 (71.9%) were female. The sample sizes ranged from 5 (Chard et al., 2009) to 1042 participants (Sackley et al., 2015), with a median of 115 participants. Further details are in Supplemental Table A.3.
Ten studies included only participants with a form of impairment or limitation, including dependence in activities of daily living (ADLs; Fisher et al., 2007; Frändin et al., 2016; Grönstedt et al., 2013; Sackley et al., 2009), dementia (Brooker et al., 2011; Chard et al., 2009; Lam et al., 2010), stroke-related dependence in ADLs (Sackley et al., 2006, 2015), dementia-related dependence in ADLs (Rogers et al., 1999), and delirium superimposed on dementia (Pozzi et al., 2020).
Interventions
All studies implemented client-centered, occupation-based interventions designed or delivered by occupational therapists as the primary approach and tailored interventions to residents’ goals, interests, or abilities to improve occupational performance, participation, or both. In most cases, the intervention was implemented by occupational therapists; however, in 1 study the intervention was delivered by a research therapist (Rogers et al., 1999), in 1 study an enriched opportunities program (EOP) intervention was delivered by a senior staff member appointed as the “EOP locksmith” (Brooker et al., 2011), and in 3 studies the intervention was delivered conjointly by occupational and physical therapists (Cichocki et al., 2015; Frändin et al., 2016; Grönstedt et al., 2013; Sackley et al., 2009), with no differentiation made between these two disciplines in one of the studies (Przybylski et al., 1996).
The duration of interventions ranged from 6 days (Pozzi et al., 2020) to 2 yr (De Vriendt et al., 2019; Przybylski et al., 1996), with a median length of 3 mo. The intensity of occupational therapy ranged from 3.6 hr delivered over 12 wk (Sackley et al., 2009) to 1-hr sessions provided daily over 2 wk (Chard et al., 2009).
Individual interventions with residents were implemented in 11 studies (Brooker et al., 2011; Chard et al., 2009; De Vriendt et al., 2019; Fisher et al., 2007; Nagayama et al., 2016; Pozzi et al., 2020; Przybylski et al., 1996; Rogers et al., 1999; Sackley et al., 2006, 2009, 2015); 2 studies implemented group interventions (Cichocki et al., 2015; Lam et al., 2010); and 3 studies implemented both individual and group-based interventions (Frändin et al., 2016; Grönstedt et al., 2013; Jung et al., 2018; Mozley et al., 2007).
Five studies explicitly focused on improving the performance of personal ADLs such as bathing, toileting, dressing, feeding, grooming, and personal hygiene (Pozzi et al., 2020; Rogers et al., 1999; Sackley et al., 2006, 2009, 2015), and 11 studies focused on improving performance of ADLs, instrumental activities of daily living (IADLs), or social or leisure activities, depending on residents’ individual goals, needs, and interests (Brooker et al., 2011; Chard et al., 2009; Cichocki et al., 2015; De Vriendt et al., 2019; Frändin et al., 2016; Grönstedt et al., 2013; Jung et al., 2018; Lam et al., 2010; Mozley et al., 2007; Nagayama et al., 2016; Przybylski et al., 1996; Rogers et al., 1999).
In this review, few studies reported on adverse events during the trial period. Four studies reported no adverse events directly attributable to the intervention (Cichocki et al., 2015; Frändin et al., 2016; Grönstedt et al., 2013; Sackley et al., 2009, 2015).
Four major intervention themes became apparent during the analysis: (1) occupation-based interventions delivered directly to residents, (2) occupation-based interventions incorporating care partner training, (3) occupation-based interventions accompanied by functional training and task-specific physical activities, and (4) multilevel occupation-based interventions, consisting of interventions both delivered directly to individual residents and also aimed at achieving longer term change through staff training and organizational-level changes.
Control Conditions
Seven studies compared the intervention with usual care (Frändin et al., 2016; Grönstedt et al., 2013; Jung et al., 2018; Mozley et al., 2007; Przybylski et al., 1996; Sackley et al., 2006, 2009, 2015). Four studies used an active control, in which participants received generic activities that were not personally tailored (Brooker et al., 2011; Lam et al., 2010), social leisure activities (Cichocki et al., 2015), or an impairment-based approach (Nagayama et al., 2016). The five remaining quasi-experimental studies compared occupational performance from preintervention to postintervention (Chard et al., 2009; De Vriendt et al., 2019; Fisher et al., 2007; Pozzi et al., 2020; Rogers et al., 1999).
Outcome Measures
The outcome of interest, occupational performance, was measured using heterogeneous assessment tools, reflecting different aspects of occupational performance, including the Barthel Index (BI) for Activities of Daily Living (n = 5; Mozley et al., 2007; Nagayama et al., 2016; Sackley et al., 2006, 2009, 2015), the Canadian Occupational Performance Measure (COPM; n = 4; Cichocki et al., 2015; De Vriendt et al., 2019; Jung et al., 2018; Pozzi et al., 2020), Assessment of Motor and Process Skills (n = 3; Chard et al., 2009; Fisher et al., 2007; Lam et al., 2010), FIM™ (n = 2; Frändin et al., 2016; Grönstedt et al., 2013; Przybylski et al., 1996), occupation-based assessments and observational tools (n = 2; Brooker et al., 2011; Rogers et al., 1999), and the Functional Assessment Measure (n = 1; Przybylski et al., 1996).
In all studies, outcome measures were administered preintervention and postintervention. Only 5 studies reported additional follow-up at different time points postintervention, ranging from 1 to 6 mo (Frändin et al., 2016; Lam et al., 2010; Sackley et al., 2006, 2009, 2015).
Quality Assessment
The quality of studies varied, with overall risk of bias analyses resulting in 11 low, 5 moderate, and 1 high risk of bias study. Factors affecting methodological quality included a lack of blinding, underpowered sample sizes, attrition, and incomplete reporting of outcome data. Overall risk of bias assessments are included in Supplemental Table A.3, and the full risk of bias evaluations are presented in Supplemental Tables A.4. and A.5.
Synthesis of Results by Theme
Occupation-Based Interventions Delivered at the Resident Level
Five studies offered occupation-based interventions directly to residents. A Level 1b study by Lam et al. (2010) evaluated the effectiveness of individually tailored occupational therapy functional task and skills training, compared with a control occupational therapy program consisting of randomly selected activities, in improving ADL performance among residents with mild to moderate dementia. At 1-mo follow-up, both the intervention and control groups demonstrated significant improvements in ADL performance; however, at 4-mo follow-up, ADL performance deteriorated in both groups (Lam et al., 2010).
A Level 2b pilot cluster RCT by Nagayama et al. (2016) examined the effectiveness of an intervention involving occupation-based goal setting, occupational performance analysis, and occupation-based practice in enhancing residents’ occupational performance. Across 12 nursing homes, the intervention resulted in significantly greater independence in ADLs compared with an impairment-based approach.
A Level 2b feasibility cluster RCT investigated the effects of introducing a client-centered occupational therapy program using individual and group-based activities to address complex occupational performance problems on care home residents’ independence in ADLs and found no significant differences in resident ADL outcomes compared with a usual-care control (Mozley et al., 2007). Another Level 2b non-RCT (Jung et al., 2018) evaluated a personally tailored leisure activity program consisting of individual and group activities and reported a significant improvement in occupational performance in the intervention group. However, COPM scores were not reported for the control group, and this study was likely underpowered to detect between-groups differences.
Finally, a Level 3b study by Fisher et al. (2007) evaluated an occupation-based intervention informed by the Occupational Therapy Intervention Process Model to improve occupational performance of eight residents of an assisted living facility and found significant improvements in residents’ ADL motor skills from baseline to posttest.
For occupation-based interventions delivered at the resident level, moderate strength of evidence exists based on mixed findings from 1 Level 1b, 3 Level 2b, and 1 Level 3b study and a pilot or feasibility design in 3 of the 5 studies.
Care Partner Training in Occupation-Based Intervention Techniques
Three Level 3b studies trained primary or professional care partners in occupation-based techniques to improve ADL performance of residents with dementia (Chard et al., 2009; Rogers et al., 1999) or delirium superimposed on dementia (Pozzi et al., 2020). Chard et al. (2009) examined the effectiveness of care partner training in verbal cueing and verbal reinforcement tailored to residents’ abilities on ADL performance among residents with Alzheimer’s disease and found significant improvements in ADL process abilities. Similarly, Rogers et al. (1999) explored the impact of a skill elicitation intervention that used task analysis and supervised skills training to tailor care partner assists to residents’ capabilities on performance of personal ADLs. Participants’ independence in dressing tasks significantly improved during the skills elicitation intervention compared with usual care. Furthermore, residents’ participation in assisted dressing significantly increased, and residents made more appropriate requests for assistance with ADLs, with improvements maintained over a 3-wk follow-up period (Rogers et al., 1999).
Pozzi et al. (2020) focused on an occupation-based intervention for nursing home residents with delirium superimposed on dementia that consisted of tailored ADL training and care partner education and involvement in therapy sessions to effectively promote residents’ ADL performance. Occupational performance and satisfaction were observed to improve from delirium onset to delirium resolution according to the COPM, despite BI and Mini-Mental State Examination scores indicating that participants’ functional status worsened at delirium onset and only partially recovered at delirium resolution.
Despite promising results and low overall risk of bias, there is low strength of evidence to support the implementation of care partner training in occupation-based techniques to improve occupational performance of long-term-care residents because there were only 3 Level 3b studies, 2 of which had small sample sizes (Chard et al., 2009; Pozzi et al., 2020).
Occupation-Based Interventions Incorporating Functional Training and Physical Activities
Four studies explored the effects of occupation-based interventions in combination with, or supplemented by, individually tailored physical activities. A Level 1b study (Cichocki et al., 2015) examined the effectiveness of a low-threshold physical activity program developed by occupational therapists and delivered by residential care staff under the supervision of an occupational or physical therapist compared with a social leisure activity control. No significant differences were found between groups in occupational performance on the COPM at posttest, and both groups improved. Another Level 1b (Sackley et al., 2009) study compared an intervention involving individualized occupation-based practice, accompanied by physiotherapy, to improve residents’ ability to perform ADLs independently, with usual care. After adjusting for baseline characteristics and care home effects, no significant differences were found in ADL outcomes between groups postintervention or at 3-mo follow-up.
One Level 1b study (Frändin et al., 2016; Grönstedt et al., 2013) explored the efficacy of a 12-wk individual and group-based physical and daily activities program targeting residents’ individual ADL and IADL goals and conducted a long-term follow-up. Although no between-groups differences were found, at 3 mo postintervention independence in ADLs significantly declined in the control group, but not in the intervention group, as assessed with the FIM. However, no significant differences were found between the groups in ADL performance at 6-mo follow-up (Frändin et al., 2016).
Finally, a Level 2b study (Przybylski et al., 1996) evaluated the effects of a fourfold increase in occupational therapy and physiotherapy staffing in a single nursing home, comparing a 1:200 staff-to-resident ratio (usual care) with a 1:50 ratio (intervention). The authors reported that therapy was tailored to individual residents; however, components of the intervention protocol were not described. Significantly greater improvements in functional independence as measured by the FIM and Functional Assessment Measure were observed in the intervention group 6 and 12 mo after implementation, but not at 18 and 24 mo (Przybylski et al., 1996).
Overall, the evidence for implementing occupation-based physical and daily activities to improve occupational performance of long-term-care residents is moderate because of inconsistent findings across studies.
Multilevel Occupation-Based Interventions
Four studies examined the effects of multilevel occupation-based interventions, where the intervention was delivered at both the individual and site level. A Level 1b study by Brooker et al. (2011) evaluated an EOP in which a senior staff member provided staff training, management, and leadership and worked with individual residents with dementia to improve their engagement in meaningful occupations. Active control homes received a project support worker coach and, after 12 mo, crossed over to the EOP intervention. Significant improvements in occupational performance were observed in both the intervention and the control groups at 6 and 12 mo postrandomization; however, occupational performance was significantly higher in the control homes 6 mo after their conversion to the EOP intervention (Brooker et al., 2011).
A Level 1b study (Sackley et al., 2015) and a Level 2b study (Sackley et al., 2006) evaluated an occupational therapy intervention for care home residents with stroke-related disabilities incorporating occupation-based goal setting and personal ADL training delivered to residents, together with the provision of staff training to continue therapy and to support residents’ mobility and participation in ADLs. Sackley et al. (2006) found a significant reduction in the number of residents who died or declined in ADL performance among participants in the intervention group compared with a usual-care control. However, Sackley et al. (2015) found no between-groups differences in occupational performance as measured with the BI.
Finally, a Level 3b feasibility study by De Vriendt et al. (2019) involved nursing home residents, managers, and staff in the development of a multilevel occupational therapy–led intervention conducted over 2 yr. Training, supervision, and support in occupation-based assessment, goal setting, and intervention were provided to staff to improve residents’ participation in meaningful daily activities. At follow-up, no significant differences were found in self-perceived occupational performance or satisfaction with performance, as measured with the COPM; however, residents reported engaging in a significantly greater number of household activities and greater satisfaction with leisure activities (De Vriendt et al., 2019).
Overall, there is low strength of evidence to support multilevel occupation-based interventions in long-term care, based on the lack of significant findings across studies and a pilot or feasibility design in 2 of 4 studies.
Discussion
To our knowledge, this is the first review to synthesize current evidence on occupation-based interventions for improving occupational performance among older adults living in long-term care. Overall, low to moderate strength of evidence suggests that occupation-based interventions delivered directly to residents, with care partner involvement, or integrated with physical activities can potentially promote the performance of everyday occupations among long-term-care residents. On the basis of these findings, it is recommended that occupational therapy practitioners offer occupation-based interventions, delivered directly to residents or integrated with physical activities, to enhance occupational performance in this population. Furthermore, practitioners should consider the implementation of occupation-based interventions with care partner involvement and multilevel occupation-based interventions based on individual client characteristics and practice context. The low to moderate strength of evidence found in this review is attributable to the significant heterogeneity in participant characteristics, interventions, and outcome measures across studies and the small number of high-quality studies with significant findings in each intervention theme.
This review found moderate evidence for occupation-based interventions delivered directly to residents to improve their occupational performance. Similar findings have been reported in studies with community-dwelling older adults (Hunter & Kearney, 2018) and people with dementia (Smallfield & Heckenlaible, 2017). Furthermore, moderate evidence was found for occupation-based interventions incorporating physical activities to improve occupational performance. Physical functioning is known to be a significant driver of ADL performance (Mlinac & Feng, 2016). Occupation-based physical activity has been shown to improve ADL performance among community-dwelling older adults, with greater effects observed among older adults with ADL performance difficulties or at risk of functional decline (Liu et al., 2018; Orellano et al., 2012). The present review found low evidence for training care partners to provide effective ADL assistance to promote occupational performance among residents with dementia. However, a systematic review by Smallfield and Heckenlaible (2017) found that care partner training and involvement in individualized interventions can effectively maintain occupational performance of people with Alzheimer’s disease and related dementias. Furthermore, evidence for multilevel occupation-based interventions involving collaboration with residents, managers, care workers, and clinicians is limited. High staff turnover and workload and financial, regulatory, cultural, and structural factors have been described as barriers to implementing complex multilevel interventions to improve resident outcomes (Smith et al., 2019). We found limited assessment of intervention effects over time, with only 5 studies reporting longer term follow-up. Hence, future research is needed to evaluate the short- and long-term effects of occupation-based interventions with care partner involvement and multidisciplinary and multilevel collaboration.
Several reasons may account for the nonsignificant findings observed in the reviewed studies. Although intervention effects in many of the included studies were small or did not reach statistical significance, even minor improvements or maintenance of function may represent a clinically meaningful difference in this population. Long-term-care residents experience increasing disability and frailty over time and a concomitant decline in occupational performance (Milte et al., 2022; Palese et al., 2016). Indeed, a systematic review examining occupation-based interventions for improving occupational performance among community-dwelling older adults found effect sizes to be small and benefits to be greater for older adults without multiple chronic health problems (Nielsen et al., 2017). Many studies in the present review included participants with multiple complex physical, cognitive, and functional impairments and a high-level dependency in mobility or ADLs, which may have affected their ability to participate in and benefit from therapy, contributing to the lack of observed intervention effects.
Furthermore, the duration or intensity of the interventions may have been insufficient to show significant effects on occupational performance in this population. Intervention duration and intensity varied widely across the reviewed studies, with interventions being predominantly 3 mo or shorter. In most included studies, we judged the intensity of the interventions as low to moderate; however, intensity was typically unclear because the interventions were tailored to residents or it was not reported. A prospective cohort study found that older adults who received higher intensity occupational therapy were more likely to achieve clinical and statistically meaningful improvements in ADL performance, regardless of frailty or severity of functional impairment at baseline (Marston et al., 2022), suggesting that interventions of greater intensity and duration may demonstrate a larger effect on occupational performance in this population.
This review specifically examined the impacts of occupation-based interventions on occupational performance outcomes, measured using subjective or objective standardized and validated assessment tools with long-term-care residents, and thus excluded studies with interventions or outcome measures not considered to be occupation based. This narrowed the literature substantially, because a scoping review by Dancewicz and Bissett (2020) indicates that use of occupation-based outcome measures in long-term-care settings is low. A systematic review by Nielsen et al. (2017) also highlighted the high focus on ADL outcomes among community-dwelling older adults, with low use of outcome measures focused on client-centered occupational performance and engagement.
Many of the reviewed studies assessed other outcomes, with significant intervention effects demonstrated for medication use, self-perceived quality of the social network (De Vriendt et al., 2019), quality of life, depressive symptoms (Brooker et al., 2011), subjective health status (Cichocki et al., 2015), self-esteem (Jung et al., 2018), and behavior of unmet needs (Rogers et al., 1999). The fact that outcomes other than occupational performance improved in some included studies is promising, and suggests that the lack of observed effects may be related to the assessment tools used to measure occupational performance. For example, Cichocki et al. (2015) could not use the COPM at 1-yr follow-up because residents no longer performed many activities initially identified as problematic (Quehenberger et al., 2014). Moreover, the COPM, FIM, and BI have been shown to have floor and ceiling effects and low responsiveness for detecting small changes in the occupational performance of older adults (de Waal et al., 2022; Wales et al., 2016). Although 11 of the included studies focused on improving performance of ADLs, IADLs, and social or leisure activities, many of the studies used ADLs as a primary outcome measure. Moreover, several studies whose interventions addressed social and leisure activity goals used the BI and FIM as outcome measures, failing to capture these occupational performance domains. Future research should focus on developing standardized assessment tools to better enable measurement of the performance of a broad range of everyday occupations in this population.
Strengths and Limitations
A limitation of this review is the considerable heterogeneity across studies and underpowered sample sizes in several of the studies, which limit the ability to make conclusive recommendations regarding intervention effectiveness. The reviewed studies were conducted in a range of countries with different health and elder care systems, which may affect the generalizability of the results. Only peer-reviewed studies published in English were included, potentially introducing publication bias. Despite our aim to capture studies addressing the performance of a wide array of occupations through a comprehensive search strategy and inclusion and exclusion criteria, many of the included studies focused on ADL performance as a primary outcome measure. Strengths of this review include the inclusion of a broad array of study types that provide a thorough consolidation of the existing evidence for the effects of occupation-based interventions on the performance of daily occupations in older adults living in long-term care.
Implications for Occupational Therapy Practice
The findings of this review have important implications for future research on occupational therapy interventions to improve occupational performance of older adults living in long-term care: ▪ Sufficiently powered RCTs that include long-term follow-up and encompass different client populations are needed. ▪ Developing a standardized approach to measuring clinically important outcomes, such as small improvements or maintenance of occupational performance among older residents, would be beneficial because this would enable higher level synthesis of evidence in this field. ▪ Further exploration of the potential benefits of occupation-based interventions with residents, care partner involvement, and multidisciplinary and system-level collaboration is warranted. ▪ Future research should explore the influence of factors such as residents’ functional and cognitive status, and intervention components, duration, and intensity, on residents’ ability to benefit from occupation-based interventions. ▪ Given the lack of substantive high-quality evidence, practitioners should offer occupation-based interventions to older adults living in long-term care that are based on individual client characteristics, with careful monitoring and documentation of outcomes.
Conclusion
Currently, moderate strength of evidence suggests that occupation-based interventions delivered directly to residents and incorporating physical activities have the potential to promote the occupational performance of older adults living in long-term care. Evidence for the use of multilevel occupation-based interventions and care partner training in occupation-based techniques is limited, and these interventions should therefore be offered on the basis of individual characteristics and practice context. More rigorous research with longer term follow-up and assessment of clinically meaningful outcomes is critical for developing the evidence base in this practice setting.
Supplemental Material
Supplementary material for Occupation-Based Interventions to Improve Occupational Performance Among Older Adults Living in Long-Term Care: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050441.pdf for Occupation-Based Interventions to Improve Occupational Performance Among Older Adults Living in Long-Term Care: A Systematic Review by Rachael Mitterfellner, Nathan M. D’Cunha and Stephen Isbel in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We acknowledge Professor Jennie Scarvell and Murray Turner, Faculty of Health, University of Canberra, Australia, for their advice during the project.
*Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.