
Abstract
The study findings identify factors that occupational therapy practitioners can target separately or in combination to improve real-world use of the more-affected upper limb poststroke.
Stroke is a common and costly health care event that results in long-term disability (Centers for Disease Control and Prevention, 2021). Approximately 50% to 70% of stroke survivors have upper limb (UL) impairments (Michielsen et al., 2012). Early after stroke onset, patients develop nonuse of the more-affected UL, resulting in reduced ability to perform daily occupations (Lee et al., 2018). Over time, nonuse becomes learned nonuse, an acquired habit in which individuals choose not to use the more-affected UL to perform daily occupations (Hirsch et al., 2021 ; Lee et al., 2018). Recent evidence has suggested that clinical trials (Kwakkel et al., 2016; Levy et al., 2016; Waddell et al., 2017) investigating the efficacy and effectiveness of interventions to promote more-affected UL function and overcome learned nonuse (e.g., constraint-induced movement therapy, robot-assisted functional electrical stimulation) show gains only in motor capacity, which is often quantified by laboratory-based assessments of impairments in body structures and functions (e.g., Fugl-Meyer Assessment Upper Extremity [FMA–UE] score, range of motion; Hsieh et al., 2014; O’Brien et al., 2018; Straudi et al., 2020). However, these gains in motor capacity are not translated to gains in real-world use of the more- affected UL, which is the ability to use the more-affected UL in real-life environments outside a laboratory or clinic (e.g., patients’ homes; Franck et al., 2019; Waddell et al., 2017). This is problematic because, despite spending billions of dollars investigating the efficacy and effectiveness of novel interventions, the majority of stroke survivors might not be able to use the more-affected UL (Bailey, Birkenmeier, & Lang, 2015). Diminished use of the more-affected UL is associated with a loss of long-term independence (Lemmens et al., 2014) and increased caregiver burden (Cheng et al., 2014) and requires costly resources (Mayo et al., 2002). It is estimated that the total costs associated with stroke-related disability in the United States are projected to increase from $105.2 billion in 2008 to more than $240.0 billion in 2030 (Harcum et al., 2019). Therefore, a comprehensive understanding of the factors influencing real-world use of the more-affected UL is critically needed. This knowledge may potentially assist in selecting active ingredients to develop personalized interventions to improve real-world use of the more-affected UL after stroke.
Real-world use of the more-affected UL has been measured in two ways. Self-reported standardized assessment scales, such as the Motor Activity Log (MAL; Taub et al., 1993; Uswatte et al., 2005) and Stroke Impact Scale (Duncan et al., 1999), have been implemented to quantify patients’ perceptions of their ability to use their more-affected UL in daily tasks (Lang et al., 2013). However, self-reported measures are often affected by patients’ motivation, comprehension, and recall ability (Lang et al., 2013). To overcome these issues, movement sensors such as accelerometers provide an objective and high-fidelity measure of use of the more-affected UL (Li et al., 2020). Accelerometers have been used in several studies to reliably measure more-affected UL use poststroke (Bailey, Klaesner, & Lang, 2015; Franck et al., 2019; Lang et al., 2021; Li et al., 2020). An accelerometer quantifies the duration and intensity of use of the more-affected UL outside the clinic (Bailey, Klaesner, & Lang, 2015). Therefore, this scoping review focused on literature objectively measuring more-affected UL use outcomes poststroke.
The objective of this scoping review was to systematically map the factors that influence real-world use of the more-affected UL poststroke. The reporting of the scoping review was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA–ScR; Tricco et al., 2018) statement and the Joanna Briggs Institute reviewers’ manual (Joanna Briggs Institute, 2015).
Method
Studies were identified by searching MEDLINE, Embase, PsycINFO, and the Physiotherapy Evidence Database (PEDro). We also conducted a manual search in 2023. A health sciences librarian designed the MEDLINE search and translated it for use in the other databases. For three databases (MEDLINE, PsycINFO, and Embase), a search string was created that consisted of natural language terms and controlled vocabulary (e.g., Medical Subject Headings), representing the search concepts of stroke, upper extremity paresis, and real-world use. In PEDro, a series of keyword searches, consisting of words representing these same concepts, was constructed and run. The MEDLINE, Embase, and PsycINFO searches were run on February 21, 2022, and the PEDro searches were run on February 17, 2022. Where available, limits to English-language articles were applied. The validity of accelerometers as a measure of real-world use of the more-affected UL was noted in 2012 (Lang et al., 2021), and so a publication date limit from January 1, 2012, to 2023 was applied to search results. Duplicate records were removed by the health sciences librarian using the Amsterdam Efficient Deduplication method (Otten et al., 2019) and a process developed by Bramer et al. (2016).
A protocol was established a priori for the search strategy, screening process, data extraction, and management. To be considered for inclusion, study participants had to (1) be age 18 yr or older, (2) have a stroke diagnosis, and (3) have UL impairment. Studies had to include an objective measure of real-world more-affected UL use (e.g., accelerometer) and assess at least one related factor of real-world more-affected UL use. Studies were excluded if (1) an assessment of more-affected UL use was done solely with a self-report instrument (e.g., MAL), (2) accelerometer data were used for validation, (3) accelerometer data were collected for structured activities within a limited time, (4) the accelerometer was not placed on the more-affected UL, and (5) the article was an editorial, review, commentary, book chapter, conference abstract, or dissertation.
In Level 1 screening, titles and abstracts were independently screened by two authors (Anadil Bayazeed and Ghaleb Almalki) using a standardized form based on the inclusion criteria. Before this screening, reviewers were trained in use of DistillerSR software (Version 2.35; https://www.distillersr.com/) and pilot tested the form with 25 studies. Disagreements between reviewers were identified weekly and resolved through discussion with a researcher (Amit Sethi) with more than 20 yr of clinical and research experience in stroke rehabilitation. In Level 2 screening, full-text articles were screened by Bayazeed using a standardized form. In Level 3 screening, data were extracted from the eligible studies using the inclusion criteria and guidance from a researcher (Sethi). Data extracted included authors’ names, publication year, study design, sample age, time since stroke, outcome measures, identified factors, and related findings. The findings were categorized using the International Classification of Functioning, Disability and Health (ICF) model’s domains Body Structures and Functions, Activity, Participation, Environment, and Personal Factors (World Health Organization, 2023).
Results
Search Results
A total of 1,347 records were collected during the initial search, of which 774 remained after duplicate records were removed. Thirty-three studies were included in the review. Refer to Figure 1 for the flow diagram and Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot, for study characteristics and evidence. The results are based on observational, secondary analysis, and experimental studies.
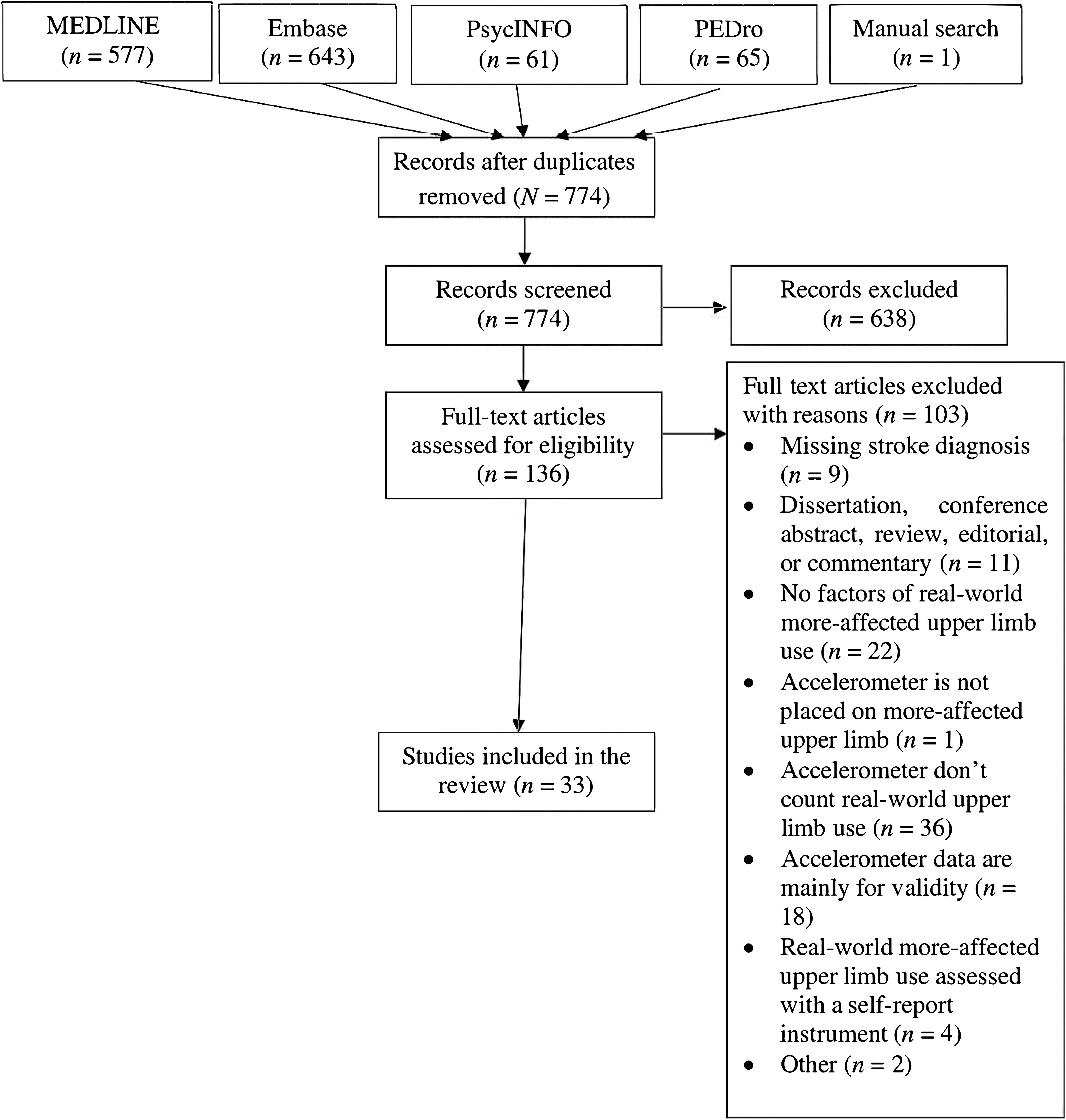
Flow of studies through the scoping review.
Body Structures and Functions
Cognitive and Psychological Factors
Cognitive skills, depression, neglect, and patients’ perceptions were identified as factors influencing more-affected UL use (Bhatnagar et al., 2020; Lang et al., 2021; Lundquist et al., 2021; Waddell et al., 2019). Absence of cognitive impairments was associated with greater use of the more-affected UL poststroke (as indicated by the acceleration profile of the more-affected UL; Chin et al., 2021; Lang et al., 2021). Additionally, more-affected UL use was significantly associated with knowledge about the importance of exercise and UL use to regain functional levels and self-efficacy (Chin et al., 2021). Also, when patients with stroke have unilateral neglect, it predicts less than the normal ratio of more-affected UL use (Lundquist et al., 2021). The perception of having less disability, as measured with the MAL (Taub et al., 1993), was associated with increased more-affected UL use (Bhatnagar et al., 2020). Similarly, perceived UL use and perceived barriers to UL recovery were correlated with better UL use in daily life (Essers et al., 2021 ; Narai et al., 2016; Waddell et al., 2019). For instance, higher self-perceived barriers to UL use were associated with less use of more-affected UL among patients with stroke (Waddell et al., 2019). Alternatively, increased self-perceived UL use was similar to increased objective more-affected UL use after individuals with stroke received constraint-induced movement therapy and conventional rehabilitation (Taub et al., 2013). Depressive symptomatology was also correlated with more-affected UL use; patients without depressive symptoms or those with reduced depressive symptoms showed greater use of their more-affected UL than those who had more depressive symptoms (Lang et al., 2021). Finally, self-efficacy was associated with more-affected UL use. Self-efficacy refers to an individual’s belief in their own capacity to successfully perform a specific task (Waddell et al., 2019). According to Chin et al. (2021) and Chen et al. (2023), patients with higher self-efficacy tended to use their more-affected UL more. In contrast, Gohlke et al. (2020) showed no association between social and cognitive activity levels and more-affected UL use.
Neurophysiological Factors
Homotopic connectivity, which is defined as the interhemispheric connectivity between similar regions of each hemisphere, correlated significantly with more-affected UL use (Urbin et al., 2014). In addition, the presence of a motor-evoked potential (MEP), which indicates the integrity of the lesioned corticospinal pathway, also predicted more-affected UL use (Lundquist et al., 2021). In contrast, Lakhani et al. (2017) found that the precentral myelin water fraction asymmetry ratio did not predict or correlate with more-affected UL use (measured by accelerometer) among individuals with chronic stroke.
Biomechanical Factors
Current evidence predominantly favors gains in UL impairment (such as muscle strength, FMA–UE score) as a factor that influences use of the more-affected UL poststroke (Bhatnagar et al., 2020; Chin et al., 2019, 2020, 2021; Essers et al., 2021; Franck et al., 2019 ; Narai et al., 2016; Rand & Eng, 2015; Regterschot et al., 2021; Shim et al., 2014). Strength, dexterity, and functional ability accounted for variances in use of the more-affected UL (Rand & Eng, 2015). Higher grip force, lateral pinch force, and balance were also associated with higher use of the more-affected UL poststroke (Chin et al., 2021). Motor compensation by the less-affected UL influenced use of the more-affected UL. Barth, Geed, et al. (2020) revealed that although bilateral UL use was reduced, unilateral less-affected UL use increased substantially among stroke survivors. In fact, fewer compensatory movements were associated with higher more-affected UL use intensity and time (Barth, Klaesner, & Lang, 2020). Although evidence from the previously mentioned studies supported the aforementioned factors, some studies reported no association between more-affected UL use and these factors. For instance, no significant association was found between body posture and more-affected UL use. Change in posture (sitting vs. standing) resulted in no difference in the amount of more-affected UL use (Michielsen et al., 2012). In addition, there were inconsistencies between more-affected UL use and more-affected UL impairment after stroke (Flury et al., 2021). The cross-sectional case series by Flury et al. (2021) revealed that discrepancies existed between more-affected UL use and UL impairment because mobile individuals with stroke who have less UL impairment as measured by the FMA–UE showed a wide range in more-affected UL use.
Activity Factors
Motor Ability
Motor ability, which includes bilateral functional capacity (Vier et al., 2022) and UL function, was associated with more-affected UL use (Bailey, Klaesner, & Lang, 2015 ; Bhatnagar et al., 2020; Gohlke et al., 2020; Lang et al., 2021; Narai et al., 2016; Rand & Eng, 2015). Bilateral functional capacity is defined as the ability to use both ULs in daily tasks, and it is often measured using standardized tests such as the Chedoke Arm and Hand Activity Inventory and the Upper Extremity Performance Test for the Elderly (TEMPA). UL function is defined as the motor ability to use the more-affected UL in laboratory-based standardized functional assessments such as Action Research Arm Test (ARAT) and Wolf Motor Function Test (WMFT). According to Vier et al. (2022), bilateral functional capacity (measured with the Brazilian version of the TEMPA) showed a positive correlation with more-affected UL use (measured by a behavioral map). Although bilateral functional capacity showed a consistent relationship with more-affected UL use, UL function showed variable patterns of associations with more-affected UL use. For instance, Doman et al. (2016) showed an inconclusive relationship between UL function (measured with the ARAT) and more-affected UL use (measured with an accelerometer). Individuals showed three different patterns: (1) an increase in ARAT scores and an increase in accelerometer profile, (2) an increase in ARAT scores and no change in accelerometer profile, and (3) no change in ARAT scores and no change in accelerometer profile.
Task Type
The ability to use the more-affected UL in unilateral or bilateral tasks also influences more-affected UL use after stroke. Patients with stroke used their more-affected UL exclusively in bilateral tasks (Michielsen et al., 2012). This was evident in an intervention study in which individuals with stroke who received a combination of robotic therapy and task-oriented training showed greater intensity and duration of more-affected UL use in bilateral tasks than unilateral tasks (Lemmens et al., 2014). The individuals in the robotic therapy and task-oriented training group showed treatment-specific effects because the robot trained the more-affected UL in bilateral tasks.
Functional Independence
Functional independence, which is the ability to perform daily occupations independently, was also associated with more-affected UL use. Narai et al. (2016) examined the relationship between functional independence and more-affected UL use after acute and subacute stroke. Not surprisingly, more-affected UL use, which was measured by means of the movement counts ratio (between the more-affected and less-affected ULs) and movement counts of the more-affected UL over 24 hr showed a significant positive correlation with functional independence (measured with the FIM® 1 ). A similar finding was observed in a secondary analysis study by Waddell et al. (2017), who examined whether task-specific training improved more-affected UL use after stroke. Individuals received task-specific intervention sessions over 8 wk. Use of the more-affected UL was quantified over 24 hr using accelerometers once a week and postintervention. Although none of the accelerometer variables showed significant changes postintervention, baseline more-affected UL use showed a positive significant association with functional independence (Waddell et al., 2017). Additionally, reduced functional independence was correlated with reduced more-affected UL use (Bailey, Birkenmeier, & Lang, 2015). In contrast, higher use of the more-affected UL was significantly associated with higher functional independence and mobility (Chin et al., 2021).
Physical Activity
Physical activity, which is defined as purposeful physical movement, is another factor that was associated with increased use of the more-affected UL (Gohlke et al., 2020). For every 1% increase in physical activity, there was a 0.0036 increase in the more-affected UL use ratio among individuals with subacute stroke during inpatient rehabilitation (Gohlke et al., 2020).
Environmental Factors
Social environments such as family support and social context (alone or not) had a significant correlation with use of the more-affected UL (Chen et al., 2023 ; Chin et al., 2021). Patients who had no family support tended to use their more-affected UL more than those who had family support (Chin et al., 2021).
Personal Factors
Current evidence exists for different factors in more-affected UL use, such as gender and age (Li et al., 2020; Lundquist et al., 2021; Rand & Eng, 2015). Age accounted for 27% of the variance in use of the more-affected UL 12 mo poststroke (Rand & Eng, 2015). According to Li et al. (2020), being male predicted minimal clinically important changes in more-affected UL use. Moreover, paresis (or weakness) in the dominant UL (also known as concordance) was associated with increased use of the more-affected UL (Lang et al., 2021; Lundquist et al., 2021). In contrast, Rand and Eng (2012) and Alt Murphy et al. (2019) found that hand dominance had no influence on more-affected UL use.
Stroke-Related Factor
Time since stroke also influenced use of the more-affected UL. For instance, more-affected UL use increased from Week 3 to Week 12 poststroke (Regterschot et al., 2021). However, a study by Lakhani et al. (2017) showed that time since stroke did not correlate with or predict UL use. Refer to Figure 2 for categorization of themes on the basis of the ICF model.
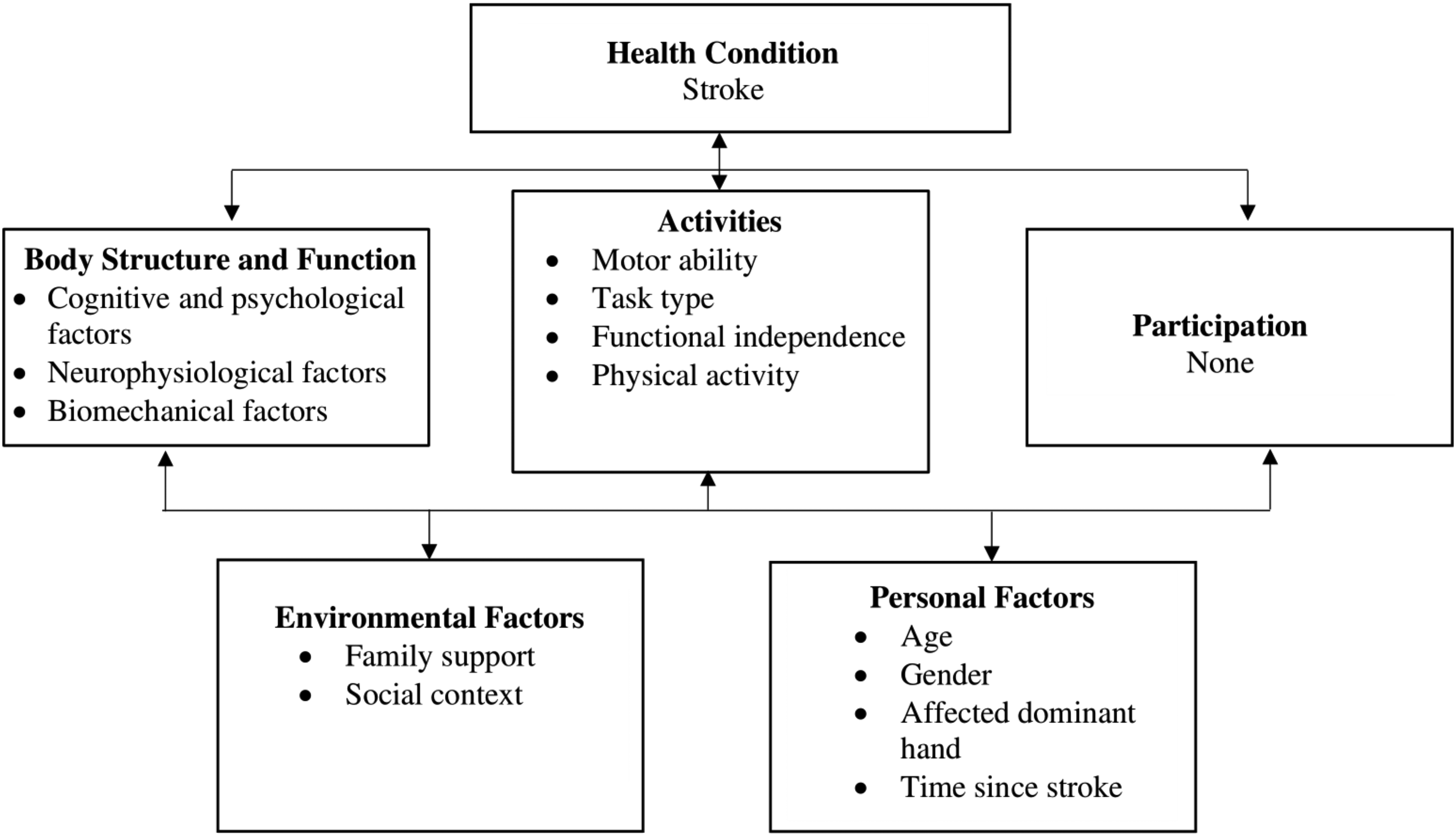
Factors of real-world use of the more-affected upper limb that are embedded in the International Classification of Functioning, Disability and Health model.
Discussion
We focused on systematically reviewing the evidence for factors that influence real-world use of the more-affected UL poststroke. English-language articles published beginning in 2012 were searched. The emerging factors for more-affected UL use poststroke were categorized using ICF model domains, namely, (1) Body Structures and Functions, (2) Activity, (3) Environment, and (4) Personal Factors.
Body Structures and Functions
Prominent factors under the Body Structures and Functions domain included cognitive and psychological, neurophysiological, and biomechanical factors. Motor and cognitive deficits are prevalent after stroke (Einstad et al., 2021). Deficits in grip strength are a common risk factor for cognitive impairment. Einstad et al. (2021) found a moderate to high correlation between cognitive function and grip strength 3 mo after stroke. The diminished cognitive capacity after stroke is associated with global disability seen after stroke, which might also influence the ability to complete daily occupations with the more-affected UL (Cramer et al., 2023). Additionally, self-efficacy, which can facilitate commitment to achieve a goal and motivate a change in the behavior of individuals with a chronic disability (e.g., learned nonuse after chronic stroke), could potentially promote use of the more-affected UL (Chen et al., 2023). So it is not surprising that cognitive functions were associated with more-affected UL use. In fact, combining cognitive training using the Cognitive Orientation to daily Occupational Performance approach with repeated task-specific training significantly improved the ability of individuals with subacute stroke to generalize and transfer learning of task-specific training from laboratory to real-world environments (McEwen et al., 2015). This could potentially explain the link between cognition and more-affected UL use after stroke.
Moreover, occupation-based behavioral activation therapy can be used to improve self-efficacy for more-affected UL use, and according to Cuijpers et al. (2007) the behavioral activation therapy aims to establish routines for activities engagement. Behavioral activation also inherently reflects the expectations underpinning occupational therapy identified by Murrell et al., (2021), as it enhances patients’ engagement in meaningful daily life activities by adopting an organized approach (Kringle et al., 2020). Therapists using behavioral activation during the first session can engage clients in a discussion of learned nonuse and the value of using the more-affected UL to perform occupations. Clients can then identify meaningful occupations in which to use their more-affected UL daily in real-world environments. Therapists can empower clients to monitor their use of the more- and less-affected ULs during occupations in waking hours using a log. Therapists can also encourage clients to schedule times to perform occupations with their more-affected UL. They can then guide clients in collaborative problem-solving to identify barriers to use of their more-affected ULs during the identified occupations. Therapists can also guide clients to reward themselves for using their more-affected UL during the scheduled occupations. Explicitly teaching these skills to translate gains in UL impairment and motor ability into daily occupations is a promising step toward promoting use of the more-affected UL after stroke.
Neurophysiological factors mainly included the presence of MEP using transcranial magnetic stimulation. An MEP indicates the integrity of the lesioned corticospinal pathway, which is the primary motor pathway controlling UL movement (Stinear et al., 2017). The presence of MEP predicted UL function recovery after stroke (Stinear et al., 2017), explaining the plausible relationship between the presence of MEP and more-affected UL use after stroke.
The link between biomechanical factors, which included UL impairment (measured by muscle strength and motor control [FMA–UE score]) as well as motor compensation and more-affected UL use, is apparent. Reduced UL muscle strength, motor control, and excessive movement compensation often limit individuals with stroke from using their more-affected UL in performing daily occupations (Cirstea & Levin, 2000). Therefore, it is not surprising that UL training is a key active ingredient for interventions to improve more-affected UL use after stroke (Waddell et al., 2017). However, gains from interventions based on UL training do not translate to improvements in more-affected UL use (Bailey, Birkenmeier, & Lang, 2015), suggesting that gains achieved from existing interventions are likely specific to the training environment (i.e., may only promote improvement on the trained tasks in a research laboratory or clinic) and rarely generalize to promote occupations in the client’s natural environment (i.e., real-world use of the more-affected UL). One of the new approaches to address this issue among individuals with severe impairment after stroke is to target the less-affected UL. According to Maenza et al. (2022), for manipulation in daily tasks, individuals with severe impairments after stroke rely on the less-affected UL. However, stroke often affects the less-affected UL, making task performance using the less-affected UL less efficient (Maenza et al., 2022). Therefore, interventions have recently been developed to train and remediate the less-affected UL to promote functional independence for individuals with severe impairments (Maenza et al., 2022).
Activity
Prominent factors under the Activity domain included motor ability, task type, functional independence, and physical activity. The relationship between bilateral functional capacity, which is categorized under motor ability, and performance of bilateral tasks seems apparent. Although individuals make their less-affected UL their dominant UL after stroke (Jones, 2017), they often tend or attempt to use their more-affected UL in bilateral tasks (Michielsen et al., 2012). For instance, individuals use their more-affected UL to stabilize an object and manipulate the object with their less-affected UL after stroke. Therefore, it is not surprising that bilateral functional capacity and performance of bilateral tasks were associated with more-affected UL use.
The role of UL function and functional independence in more-affected UL use is evident, given the positive relationship observed between tests of UL function (e.g., ARAT, WMFT) and global function (i.e., FIM; Chae et al., 1995; Duncan et al., 1992; Fong et al., 2001). The role of physical activity in the prevention and management of stroke is highlighted across stroke management guidelines (Hoh et al., 2023). Individuals who exhibit high physical activity tend to be more active and to have recovered functional ability after stroke (Gohlke et al., 2020). Hence, it is plausible to believe that these individuals would show increased use of their more-affected UL in daily occupations.
Environment
Environmental factors included family support and social context. Although family support showed a negative association with use of the more-affected UL (Chin et al., 2021), social context significantly predicted more-affected UL use (Chen et al., 2023). An explanation for this discrepancy could be that individuals who live alone tend to use their more-affected UL more because they cannot rely on family support (Chin et al., 2021). However, social context, which includes the presence of motivating caregivers at home, provided individuals with a sense of safety that promoted more-affected UL use (Chen et al., 2023).
Personal Factors
Hand dominance constituted an important personal factor. When the dominant UL becomes the more-affected limb after stroke, it has a positive influence on the amount of UL use. According to Lang et al. (2021), this is explained by the fact that the world is designed more for right-handed people; thus, individuals with stroke who experience paresis in the right dominant UL had longer more-affected UL use. This could be reflected in an accelerometer profile as asymmetry. According to Bailey, Klaesner, and Lang (2015), although nondisabled individuals had symmetrical density plots indicating equal use of both ULs, individuals with stroke had asymmetrical density plots with reduced bilateral UL intensity and more lateralized (unequal) bilateral UL use. For individuals with stroke, those whose nondominant UL was affected had an increased negative magnitude ratio compared with individuals whose dominant UL was affected, indicating lesser use of the nondominant affected UL (Bailey, Klaesner, & Lang, 2015).
Future Research Directions
Future research is warranted to examine the effect of other factors (e.g., stroke location and type) on real-world UL use. In addition, the factors highlighted in this review could also be incorporated with the principles of behavioral activation to systematically develop and investigate an intervention to improve more-affected UL use.
Strength and Limitation
The strength of this scoping review is our collaboration with a health sciences librarian to conduct a comprehensive search. Our study was limited in that we did not appraise studies for their level of evidence.
Implications for Occupational Therapy Practice
Existing interventions (e.g., robot-assisted therapy, constraint-induced movement therapy, functional electrical stimulation) to improve more-affected UL use are designed using biomechanical factors (UL impairment and strength) and motor ability (UL function and functional independence). However, these interventions are not effective in improving use of the more-affected UL in real-world environments (Bailey, Birkenmeier, & Lang, 2015). Existing interventions typically do not address improving individuals’ self-efficacy and confidence in more-affected UL use, which is required to overcome learned nonuse and incorporate more-affected UL use in daily occupations. Therefore, this review has the following implications for occupational therapy practice: ▪ Therapists can incorporate behavioral activation theory in designing an occupation-focused intervention to augment self-efficacy and confidence in use of the more-affected upper limb in daily occupations. ▪ Therapists can incorporate the factors identified in this review as additional active ingredients that could be carefully added to behavioral activation to develop an intervention package to improve more-affected UL use poststroke.
Conclusion
The review identified multiple factors from ICF domains that influence more-affected UL use poststroke. UL impairment, motor ability, functional independence, task type, hand dominance, and perception of more-affected UL use were the prominent factors. Incorporating these factors with occupation-based behavioral activation may enhance more-affected UL use and advance occupational therapy practice.
Supplemental Material
Supplementary material for Factors Influencing Real-World Use of the More-Affected Upper Limb After Stroke: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050512.pdf for Factors Influencing Real-World Use of the More-Affected Upper Limb After Stroke: A Scoping Review by Anadil Bayazeed, Ghaleb Almalki, Amjad Alnuaim, Mary Klem and Amit Sethi in The American Journal of Occupational Therapy
Footnotes
1
FIM® is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
*
Indicates articles included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.