
Abstract
This study provides information to help occupational therapists to work with family caregivers to prevent a decline in their self-care and improve their quality of life.
Caregiving is an occupation that involves two types of activities: providing care for others and child rearing, which may include providing care and supervisory activities (American Occupational Therapy Association [AOTA], 2020). Caring occupations are determined by culture, especially among Latin American–Mediterranean countries with a culture of familism, in which women have traditionally been assigned the social function of providing care in the private sphere. This model is characterized by high family involvement in care and a lack of formal care (Bagatell et al., 2023; Cetré Castilblanco, 2023; Santana et al., 2023).
Caring for loved ones is associated with several benefits, including personal fulfillment; however, it is also associated with physical, psychological, and financial burdens (Bagatell et al., 2023; Swartz & Collins, 2019). Caregivers of family members with a disability or chronic disease typically assume the caregiver role for an indefinite period, and the onset usually appears suddenly, involuntarily, and without any preparation. Caregiving is highly stressful, affects the family organization, and has a negative effect on health, especially that of the main caregiver (Agulló Cantos et al., 2019; Castellanos, 2022).
Consequently, family caregivers accumulate a series of symptoms such as emotional exhaustion, stress, depression, tiredness, and physical fatigue, which are all part of caregiver syndrome and which other researchers have associated with diseases such as hypertension, diabetes mellitus, dyslipidemia, depression, circulatory disorders, thyroid disorders, and even cognitive impairment (Buenfil Díaz et al., 2016; Orta et al., 2016). Although some studies have reported the abandonment of self-care by family caregivers as a result of the demanding levels of caregiving, there have been no analysis of the activities that were affected and their relationship with health (Agulló Cantos et al., 2019; Guato-Torres & Mendoza Parra, 2022).
Self-care is one of the main areas of human occupation along with productivity and leisure. It consists of all those activities and tasks of daily living related to caring for oneself (Forn de Zita, 2009). Difficulty in carrying out these activities and participating in daily life situations can affect a person’s health and well- being (AOTA, 2020). Knowing which self-care activities (SCAs) are affected among family caregivers can contribute to the creation of more effective intervention programs.
Study Purpose
In this article, we analyzed the SCAs that were affected in caregivers of a family member with a disability or chronic illness, based on three objectives: Objective 1: to describe the sociodemographic and caregiving profile of family caregivers Objective 2: to analyze the affected SCAs and their relationship with occupational performance, satisfaction, and quality of life (QoL) Objective 3: to analyze whether there are differences in the alterations of SCAs related to the age and gender of the family caregiver.
Method
We conducted a descriptive, cross-sectional, and analytical study of family caregivers from 20 social health care entities in the city of Zaragoza, Spain, that care for people with physical, mental or cognitive, sensory, intellectual, and developmental disabilities in 2018.
The following inclusion criteria were established for the sample selection: ▪ family caregivers age 18 yr of age or older who have no mental illness or cognitive impairment and who do not receive specific remuneration for the care provided. ▪ being the primary caregiver, sharing caregiving with other family caregivers or collaborating in care on an ad hoc basis for at least 1 yr. ▪ family member receiving care with some functional limitation, whether physical, mental, intellectual, or sensory, due to age or chronic illness, and may be dependent or only require supervision or support in activities of daily living on a long-term basis.
The sample size was defined as 377 persons with a maximum margin of error of 5% for a confidence level of 95% and under the assumption of maximum variance (p = q = .5). We obtained a sample of 500 persons; therefore, the margin of error was 4.3% for a confidence level of 95%.
Assessment Instruments
We collected sociodemographic information of the caregivers and their family members using an ad hoc questionnaire and administered two assessment instruments. The Canadian Occupational Performance Measure (Law et al., 2014) assesses occupational performance and satisfaction. The respondents identify the activities in which they have problems with their performance and assign them a value from 1 (lowest) to 10 (highest) to rate their satisfaction and performance when carrying out these activities (Gatta et al., 2022; Law et al., 2014).
The World Health Organization–Quality of Life (WHOQOL–BREF) measures a person’s QoL (WHO, 2012). It consists of 26 questions and is scored from 1 to 5, where 1 represents the worst condition and 5 represents the best condition. The WHOQOL–BREF provides a profile of QOL perceived by the person in four areas: physical health, psychological health, social relationships, and environment (Salinas-Rodríguez et al., 2022 ; WHO, 2012).
The questionnaires were delivered, collected, and analyzed personally by Laura Gonzalo-Ciria, thus safeguarding the identity of the participants at all times.
Data Analysis
Qualitative variables were described using absolute (n) and relative (%) frequencies, and means and standard deviations were used for quantitative variables. We performed comparisons between groups using the χ2 test (qualitative variables) after the assumptions of normality (Kolmogorov–Smirnov test) and homogeneity of variances (Levene test) had been verified. We made two-by-two comparisons, using the Bonferroni correction in cases in which there were more than two groups and the statistical test was significant.
To determine the possible relationship between quantitative variables, we calculated Pearson correlation coefficients. We performed a statistical analysis using IBM SPSS Statistics (Version 23.0) for Windows. Values with p < .05 were considered statistically significant.
The study was approved by the Research Ethics Committee of the Autonomous Community of Aragón and was carried out in accordance with the ethical considerations of the World Medical Association in the Declaration of Helsinki. All participants signed the informed consent form, and both their privacy and the confidentiality of their personal information were protected. All the collaborating entities in the study signed a written agreement and gave their authorization for the study.
Results
The sample consisted of 500 family caregivers. Table 1 shows participants’ sociodemographic information and caregiver profile. Notably, the mean age of caregivers was 60.3 yr, most of the primary caregivers were women (72.8%), more than half of them had a secondary education or higher, and 61.6% did not have a paid job. The total number of family members cared for was 500, mostly women (55.8%), with mixed disability in 69.8% of the cases with high dependency. Participants had assumed the role of caregiver for an average of 13.2 yr, for 15 hr a day, with 4 hr off each day. More than one-third of caregivers had illnesses that hampered their caregiving duties, and 75.4% (n = 377) were living with the family member they cared for (Table 1).
Sociodemographic Information and Characteristics of Family Caregivers and Care Recipients
Regarding the affected activities, greater difficulty was found in activities related to caregivers’ self-care, followed by those concerning community management and mobility. About one-third (32.8%) of caregivers considered that they had difficulty in fulfilling all the activities related to self-care that they would like to perform. Getting enough rest and sleep was found to be the most affected activity (46.6%), followed by receiving treatments to improve health (31.6%) and physical exercise (31.2%; Figure 1).
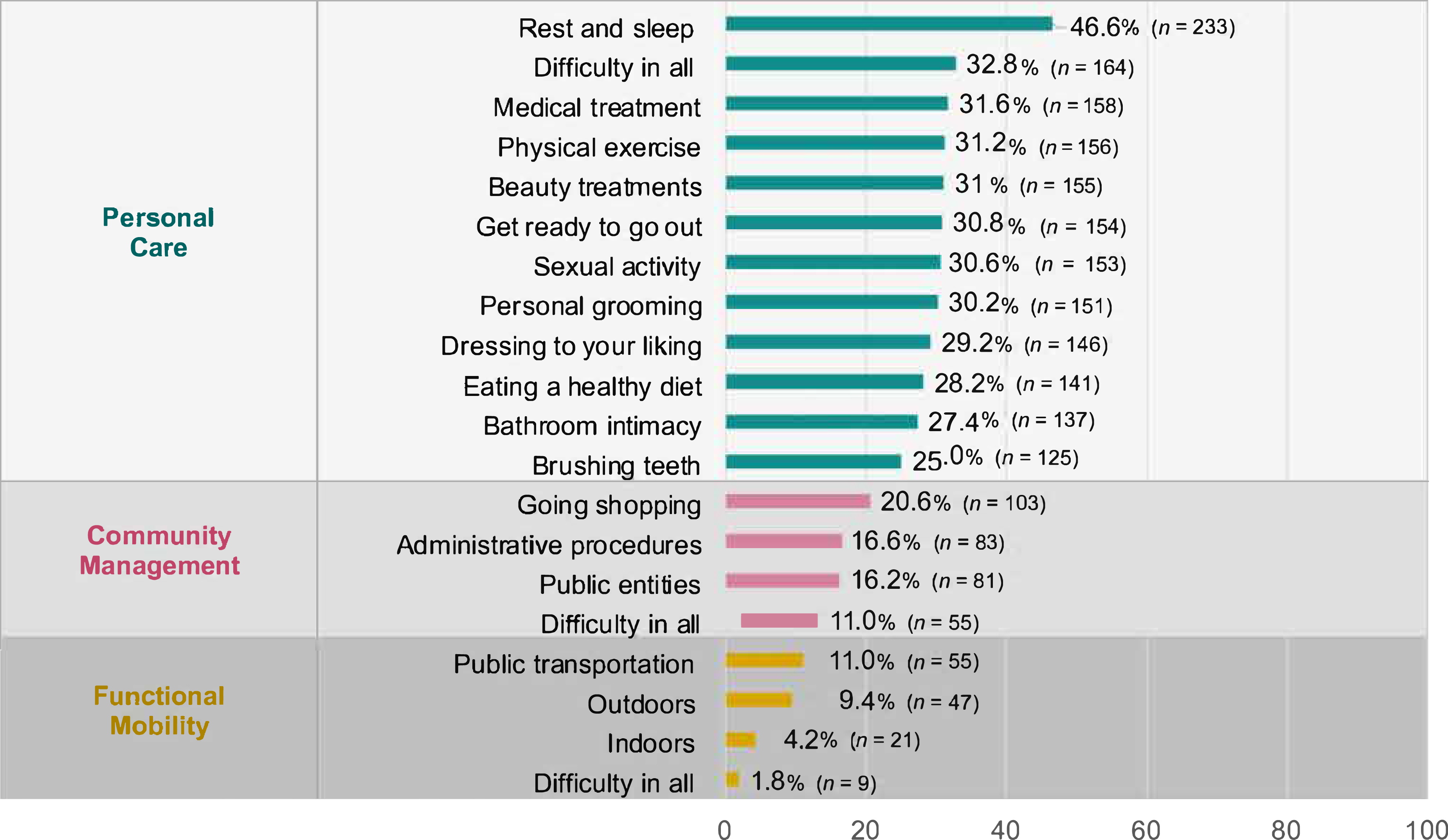
Prevalence of affected self-care activities among family caregivers.
The family caregivers obtained a mean occupational performance score of 3.77 (SD = 2.18), a mean satisfaction score of 5.02 (SD = 2.69), and mean QoL scores as follows: physical health, 56.39 (SD = 19.49); psychological health, 54.75 (SD = 18.52); social relations, 50.1 (SD = 20.84); and environment, 54.31 (SD = 15.51). After analyzing the occupational profile variables and their relationship with performance, satisfaction, and QOL, we observed that as the number of affected activities increased, performance, satisfaction, and QOL decreased, with the exception of SCAs, which were not correlated with satisfaction (Table 2).
Pearson Correlations Between the Number of Self-Care Activities Affected and Occupational Performance, Satisfaction, and Quality of Life
*p < .05. **p < .01.
After analyzing the relationship between the affected SCAs and participants’ gender, χ2 tests revealed that female caregivers had greater difficulty than male caregivers in certain aspects related to self-care, such as taking a shower in peace, personal grooming, dressing according to their preferences, and receiving medical and beauty treatments. In addition, women had greater difficulty than men in moving around outside the home and using public transport. No significant differences were found between female and male caregivers in relation to community management tasks.
Significant differences were observed when age was related to self-care difficulties. Younger caregivers reported more difficulties fulfilling all SCAs, with the exception of sleeping, resting, and brushing teeth, for which no significant differences were observed in relation to the age of the caregiver. In contrast, older caregivers presented greater difficulty with their mobility both indoors and outdoors (Table 3).
Self-Care Activities in Which the Family Caregiver Has Difficulty, by Gender and Age
Note. p values were derived from
*p < .05. **p < .01. ***p < .001.
Discussion
To our knowledge, this is the first study to analyze the affected SCAs while relating them to performance, occupational satisfaction, and QoL in a population of family caregivers, providing a perspective on gender and occupational performance. Our results show how SCAs are impaired in family caregivers and their relationship with lower satisfaction and QoL, especially among women, consistent with other studies (Guato-Torres & Mendoza Parra, 2022; Van Roij et al., 2021). Caregiving has a negative impact on the health of caregivers, who are unable to get sufficient rest, receive medical treatment, or engage in healthy activities such as physical exercise. In fact, one-third of the caregivers had illnesses that hampered their ability to care for their family member.
A lack of self-care among family caregivers is evident, which would explain a decrease in adherence to medical treatments and unhealthy lifestyles, such as substance abuse (e.g., tobacco, alcohol, drugs), together with inadequate nutrition and a higher incidence of diseases. This pattern of behavior could be related to caregiver syndrome (Buenfil Díaz et al., 2016; Orta et al., 2016; Park, 2021), associated with lower subjective well-being and physical health (Castellanos, 2022; Guato-Torres & Mendoza Parra, 2022; King et al., 2021). Our results indicate that the reality faced by family caregivers does not correspond to a lack of awareness, as considered by other authors (Yip, 2021). Rather, it is more likely that they are unable to perform their own SCAs or do so with much difficulty because they prioritize time spent caring for their family member, which negatively affects their health because of their inability to carry out meaningful activities and participate in life situations (AOTA, 2020).
Our findings are consistent with those of de Wit et al. (2019) in their study on caregivers with a family member with amyotrophic lateral sclerosis. These researchers stated that mobility difficulties limited caregivers’ participation in social activities and that most of the caregivers’ time was dedicated to bureaucratic procedures, which, added to the need to accompany their family member to medical visits, reduced their own self-care time, affected their working life, and generated stress (Bagatell et al., 2023; de Wit et al., 2019). Our data show that difficulties involving rest and sleep affect more than half of the caregivers. These results coincide with those of Lauritzen et al. (2015), who highlighted insomnia and fatigue as the main repercussions of caregiving, with a negative impact on their physical, psychological, and social health. In contrast, Hijuelos García et al. (2018) reported that lack of sleep and the need for rest did not appear to be an issue affecting the performance of caregivers. These conflicting findings could be because the caregivers presented higher levels of performance and their relatives presented lower levels of dependency than those in our study. Moreover, Hijuelos García et al. (2018) presents certain limitations such as the small sample (18 caregivers) and the reduced number of variables, with a homogeneous population of caregivers of relatives with physical disabilities.
Caregivers ages 18–40 yr displayed the most difficulty in all the SCAs assessed, with the exception of sleeping and resting. Thus, a trend is observed, in which, as the caregiver ages, they report less difficulty in SCAs, in line with other studies (Roca Roger, 2000). Some authors interpret this as an acceptance of their condition as caregivers, which leads them to adjust their values and interests (Agulló Cantos et al., 2019).
There seems to be a tendency to consider care across the life span, with a focus on the care recipient rather than the caregiver. A study by De Oliveira et al. (2015) found that caring for children was associated with more depressive symptoms, whereas caring for older adults was associated with greater caregiver burden; however, no significant differences have been found concerning the caregivers’ QoL. In contrast, in our study we focused on the characteristics of family caregivers, and we found that QoL is impaired because of the difficulties related to the fulfillment of SCAs, which is in turn related to lower occupational performance and satisfaction.
Gender and occupational analyses are fundamental in research related to caregiving. However, we have not found any study that included analyses of both occupation and gender, as in our study. Our results can help to explain these differences, because the female caregivers in our study reported greater difficulties in aspects related to self-care such as personal grooming, receiving beauty treatments and medical treatments, and dressing according to their preferences. In addition, they had more difficulty than men regarding mobility outdoors, which may help explain why men perform more caregiving tasks outside the home (e.g., shopping, errands), which are protective activities in terms of perceived health decline (García Calvente et al., 2011). In addition, the greater self-care involvement of female caregivers could explain their worse QoL compared with male caregivers. García Calvente et al. (2004) showed that female caregivers who had no health problems before caregiving were those who perceived their health status as poor or very poor, in contrast to female caregivers who already had some kind of health problem before caregiving. Both studies show the impact on health and QoL of female caregivers; our findings complement this by also assessing male caregivers, providing evidence of a greater impairment of QoL among female caregivers than among their male counterparts. Moreover, if we consider the greater involvement of women in caregiving, this constitutes a key element for understanding the impact of gender roles on health inequalities (García Calvente et al., 2011). The obligation to care clashes with the concept of occupational justice, which ensures that people have the opportunity for full participation in occupations that define and complement them as persons (Bailliard et al., 2020). Similarly, the WHO and the philosophies advocated in the Ottawa Charter for Health Promotion recognize that health can be affected by a person’s inability to carry out activities and participate in life situations, thus highlighting occupational performance and participation as factors that benefit people’s health and well-being (AOTA, 2020). Consequently, programs directed toward family caregivers should consider their QoL and recommend appropriate treatments.
Limitations
Although our sample size was sufficient, our study population was limited to a single region in Spain, which limits the generalization of the results to other contexts. Variables such as age of care recipients, living with a relative, community resources, and social support (which has not been analyzed in this study) could have influenced the results. However, our study focused on caregivers so that their needs can be assessed from an occupational therapy standpoint. We believe that the results of this study are highly useful for health care workers and especially for occupational therapists who work with clients of all ages and their respective family caregivers.
Implications for Occupational Therapy Practice
Although additional research on the SCAs of family caregivers is necessary, the findings of this study have the following implications for occupational therapy practice. Occupational therapy practitioners can ▪ improve programs aimed at caregivers of family members with a disability or chronic disease by addressing their self-care needs to improve or preserve their QoL; ▪ improve management of resources on the basis of caregivers’ gender and age; and ▪ attend to the needs of family caregivers, which should be a priority in occupational therapy practice.
Difficulties related to the self-care of family caregivers should be addressed in the curriculum of future occupational therapists.
Conclusion
Caregivers of family members with disabilities or chronic disease, and to a greater extent young people and women, experience a decline in SCAs, especially with difficulty resting and sleeping. This decline is directly related to lower occupational performance, satisfaction, and QoL.
Footnotes
Acknowledgments
The support of all the entities and caregivers who participated in this study is gratefully acknowledged.