
Abstract
Gaps identified in this scoping review highlight inconsistencies in the reporting of treatment specificity that may affect the replication and translation of Ayres Sensory Integration® (ASI) research into practice.
Clinical research is conducted with the purpose of increasing evidence-based practices that clinicians can implement for the benefit of their client population. Research findings are often conveyed to practicing clinicians through the publication of research articles. Although this transaction appears simplistic, a 17-yr gap exists between the publication of research and the intended clinical implementation (Morris et al., 2011). Some attribute this phenomenon to the “black box of rehabilitation” or “the absence of a shared and standardized way to define rehabilitation treatments with respect to the elements that bring about changes in patients/clients” (Dijkers, 2019, p. 144). A lack of specificity when describing interventions may significantly contribute to a gap in the communication between researchers and consumers of research. This barrier is thought to emerge when researchers do not clearly define the essential characteristics, elements, and clinical reasoning processes that underlie complex and multifaceted rehabilitation interventions (Reynolds, 2023).
To solve the predicament of the black box, clinicians and researchers from a variety of disciplines have been working toward developing a way to specify rehabilitative interventions across disciplines (Hart et al., 2019). As a result, the Rehabilitation Treatment Specification System (RTSS) framework has been developed. This system aims to provide a universal system for specifying rehabilitation interventions using a theory-based framework (Zanca et al., 2019). The RTSS provides researchers with a set of guidelines to follow to specify which impairments are being treated and which aspects of treatment are expected to produce a functional change (Dijkers, 2019). Treatments are specified by the following triad of components: (1) the intervention target, (2) the active ingredients of the intervention, and (3) the hypothesized mechanism of action, which is often based on the treatment theory (Hart et al., 2019). The target indicates which aspect of functioning is being directly targeted for change, the ingredients are what the clinician does, and the mechanism of action is how the treatment is expected to work.
Application of the RTSS has not been widely adopted in the occupational therapy literature, although the profession continues to have the same translation gaps as other rehabilitation professions (Juckett et al., 2019). Even interventions that have moderate to strong levels of evidence, such as Ayres Sensory Integration® (ASI) intervention (Schoen et al., 2019), continue to have challenges with accurate implementation in clinical practice. Such challenges are due to the various applications of ASI under diverse conditions or to specific patient populations. Although the complexity of this intervention is advantageous, it requires the practicing clinician to understand the conditions and decision- making behind the approach, which may or may not be well described by the research team.
The purpose of this scoping review was to identify gaps in reporting of research relating to ASI interventions. Our guiding question was the following: Which elements of specificity (i.e., ingredients, targets, mechanisms of action, and progression) are most often present and most frequently omitted from research using ASI interventions? Our rationale was that elucidating the current specificity elements used when describing ASI intervention will help to establish a baseline and identify areas of need for future research reporting.
Method
Eligibility Criteria
The studies included in this review met a number of criteria to be considered eligible. The study designs had to be quantitative in nature and considered a Level 1, 2, 3, or 4 level of evidence (Oxford Centre for Evidence-Based Medicine, 2009). For studies to be included, the study participants had to be younger than age 18 yr (children) with differences in sensory processing and integration. Eligible studies had to assess the effectiveness of ASI intervention or occupational therapy using a sensory integration approach (OT–SI) in an outpatient clinic setting. To be considered for this review, studies had to be available in full text, published in a peer-reviewed journal, and published in English within the past 20 yr.
Identification of Relevant Studies
The literature was searched using keywords related to sensory integration intervention and its application to individuals with difficulties in sensory integration and processing. The databases searched were PubMed, CINAHL, PsycINFO, Cochrane Library, and ERIC. Searches were conducted between May 22 and 23, 2023. The search terms and strategy used for each database are reported in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Study Selection
The selection process was organized using Covidence (Veritas Health Innovation, 2023), a web-based collaboration software platform that streamlines the production of systematic and other literature reviews. Studies yielded from the search were imported into Covidence for screening and the removal of duplicates. Two reviewers (Ishanie Choudhury and Mary Davis) independently reviewed the titles and abstracts of all remaining studies on the basis of the predetermined eligibility criteria. Conflicts were resolved by a third member of the research team (Stacey Reynolds). Studies that passed the initial screening received a full-text review to assess eligibility. These studies were also dual screened independently with a third party resolving conflicts. The remaining studies were included in the review with data extracted to answer our research question. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for study inclusion is presented in Figure 1. Included studies were independently reviewed and data were extracted by the first author (Choudhury). Of the 22 included studies, 10 were selected at random and dual reviewed (by Reynolds) to ensure accuracy.
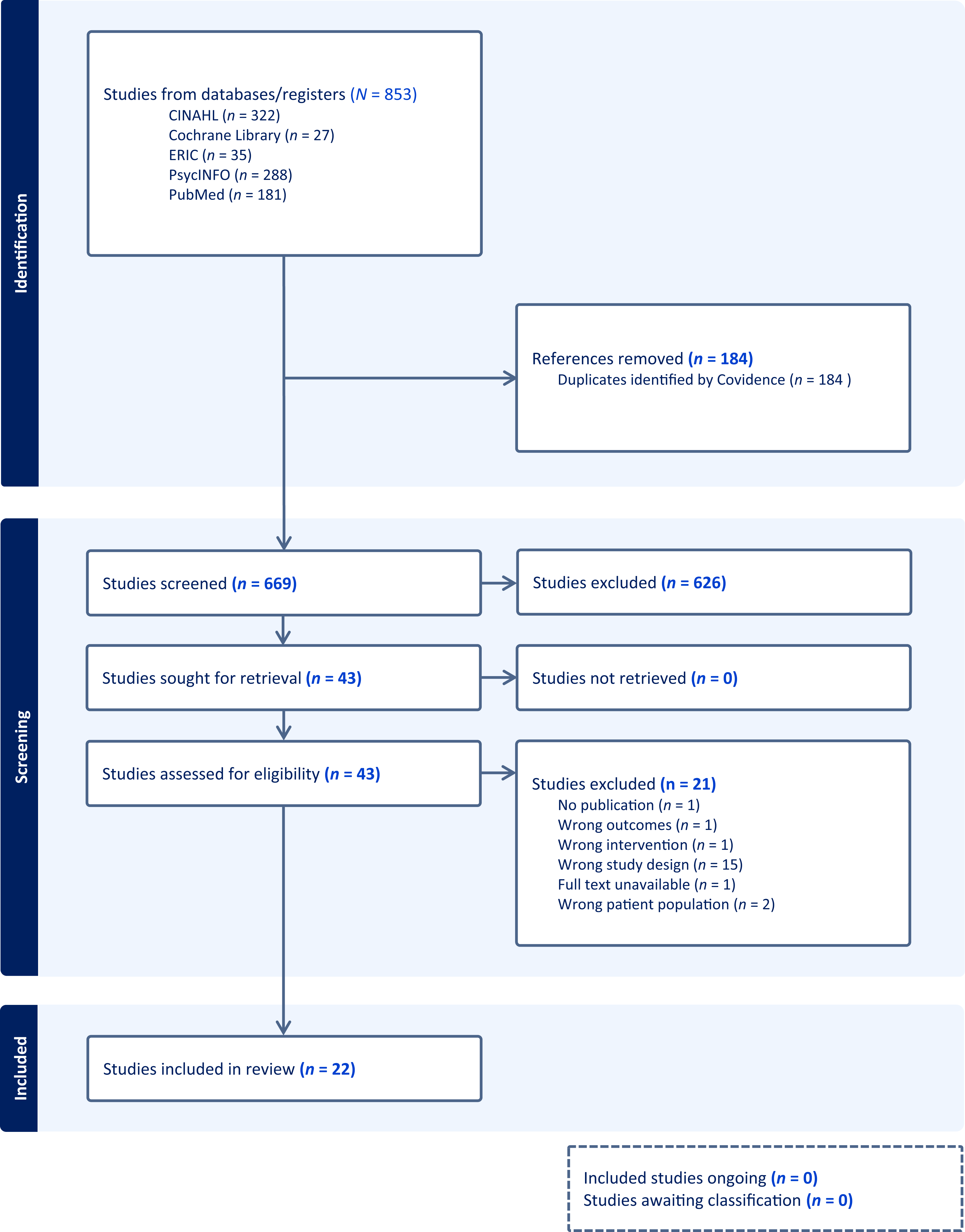
PRISMA flow diagram of the scoping review process.
Data Extraction
Data were organized in a table using elements from the RTSS framework (Hart et al., 2018) as well as additional information used to specify the intervention. The table contained the following fields for each study: level of evidence, use of a fidelity measure (yes or no), ingredients, mechanism of action, target, aims, progression, and external sources. We used the Oxford levels of evidence table (Oxford Centre for Evidence-Based Medicine, 2009) to rank methodological rigor and study design. Using the RTSS guidelines, we defined ingredients as the observable actions of the clinician during intervention, target as the aspect of functioning that is being targeted for change, and mechanism of action as how the intervention is expected to work (Hart et al., 2018). Also using the RTSS, aims were defined as the overall goals of the intervention, and progression was defined as how the intervention changed on the basis of a variable such as time or patient response (Hart et al., 2018). External sources were defined by our team as resources authors used to inform their intervention.
Data Synthesis
As part of our analysis process, we identified the percentage of studies including specificity elements (i.e., ingredients, targets, and mechanisms of action) to learn more about what was most commonly present in or omitted from research reporting. In addition to overall percentages, the data were also reviewed to ascertain the percentage of times an ingredient was listed in conjunction with its target or mechanism of action or cases in which all three elements were present. We then proceeded to describe the percentage of studies that specified how a client was progressed through the intervention as an added element of treatment specificity. Finally, we looked at any potential relationships between the level of evidence of a study and the number of elements of specificity listed.
Results
A total of 853 studies were imported into Covidence for screening. Of these, 184 duplicates were removed, leaving 669 for title and abstract screening. Of these, 626 studies were deemed irrelevant, leaving 43 full-text articles to be assessed for eligibility. Of these studies, 21 were excluded, leaving 22 studies to be included for analysis.
The levels of evidence (Oxford Centre for Evidence-Based Medicine, 2009) for the included studies are as follows: three Level 1b, seven Level 2b, eight Level 3b, and four Level 4. Study designs included randomized controlled trials, nonrandomized controlled trials, a quasi-experimental study, pilot and feasibility studies, interrupted time series, nonconcurrent multiple-baseline case studies, retrospective pretest–posttest studies, and single-subject case studies. All but 1 of the studies used the ASI Fidelity Measure© (Parham et al., 2011) as part of their study design.
Results of individual studies are listed in Table A.2 in the Supplemental Material. Of the 22 included studies, 100% included ingredients, 63% included mechanisms of action, and 86% included targets. When looking at the total number of ingredients (134) across studies, 49% were listed in conjunction with a target, 15% were listed in conjunction with a mechanism of action, and 11% were listed in conjunction with both a target and a mechanism of action. Of the studies, 23% included a description of how the client was progressed through the intervention.
When analyzing a study’s level of evidence in relation to its included elements of specificity, we found that the Level 4 studies included in this review tended to list more ingredients, mechanisms of action, and targets than studies of other levels. Level 4 studies included 6 to 15 ingredients, 1 to 2 mechanisms of action, and 4 to 7 targets; Level 3b studies, 4 to 9 ingredients, 0 to 2 mechanisms of action, and 1 to 6 targets; Level 2b studies, 1 to 7 ingredients, 0 to 2 mechanisms of action, and 0 to 4 targets; and Level 1b studies, 5 to 8 ingredients, 1 to 2 mechanisms of action, and 2 to 4 targets.
Discussion
The purpose of this scoping review was to scan the literature to determine the level of specificity used when reporting research on ASI interventions. The review included 22 studies, and each was assessed for elements of specificity (ingredients, mechanism of action, target). All included studies listed ingredients (actions of the therapist), albeit in varying degrees. Although some studies included up to 15 ingredients, others listed as few as 1 ingredient. The way ingredients were described ranged from general statements, such as “individually designed interventions (based on sensory profiles) that expose children to multisensory stimulations through play” (Raditha et al., 2023, p. 1668), to more specific descriptions, such as providing individually tailored sensory–motor activities embedded in play . . . with the child’s active participation. . . . [that provided] opportunities for
▪ High levels of proprioception (wheelbarrow walk; pulling, climbing, or carrying heavy items)
▪ Pressure touch (e.g., hug, massage, using a weighted blanket, playing in spandex, moving under large pillows)
▪ Oral–motor activities (e.g., resistive chewing, blow toys, drinking thick liquid, using a straw to blow items across table)
▪ Antigravity control positions during play
▪ Opportunities to rearrange, remove, and replace equipment or materials, based on the child’s response
▪ Changes in intensity, duration, frequency, or rhythm of sensory experiences, based on the child’s response. (Faller et al., 2016, pp. 5–6)
The element of specificity that was reported least often was mechanism of action, with only 63% of studies reporting at least one mechanism of action. Very rarely (11%) were all three elements of specificity from the RTSS framework listed in conjunction.
Collectively, these findings suggest that authors are most comfortable identifying the actions required by therapists during the intervention process. However, authors are less consistent in reporting the direct outcome they expect to see because of that action or the reasoning process behind the choice of that action. Published work often omits the clinical reasoning process used in delivering interventions, which presents a problem in translating this work into clinical practice.
We also noted that many of the studies relied heavily on the ASI Fidelity Measure (Kuhaneck et al., 2023; Pfeiffer et al., 2011; Raditha et al., 2023; Schaaf, Benevides, et al., 2012; Waldman-Levi & Kuhaneck, 2023) as a basis for their intervention description. It is important to note that the ASI Fidelity Measure was designed to measure structural and process aspects of ASI intervention so that researchers could determine whether an intervention was delivered in a manner true to the underlying therapeutic principles on which it is based (Parham et al., 2011). Fidelity measures are not intended to replace intervention manuals, intervention protocols, or descriptions of the decision-making processes. Moreover, the ASI Fidelity Measure lists only key elements that should be included in true ASI intervention, but it does not link these elements to specific client outcomes. Linking therapist actions to client outcomes (via a mechanism of action) is the responsibility of the research team and should be reported as part of the research article; this step cannot be replaced by citing a fidelity tool or referencing general treatment principles.
Similar to heavily referencing the ASI Fidelity Measure, many authors cited key references in lieu of fully describing their intervention in the article. For example, a clinical textbook published by Schaaf and Mailloux (2015) was cited by multiple authors as a means of providing a detailed description of the intervention in the published article. Although this text does provide a clinical guide for implementing ASI in children with autism, referencing this text does not replace providing specificity elements unique to the study conducted; in most cases, the authors also did not identify how the guidelines were adapted for children who did not have autism. The textbook Sensory Integration: Theory and Practice (Bundy et al., 2002) was also cited by multiple authors in the intervention description section of their article. Given that this textbook is more than 400 pages long, it is difficult for a reader to determine which aspects of the text were extracted in designing, implementing, and evaluating the specific intervention.
A contributing factor to the lack of intervention specification can likely be attributed to journal restrictions related to word count and art elements (e.g., tables, figures, images). Authors are often in a position of having to decide which sections of the research article to give the most space to, likely sacrificing intervention specificity for results or discussion sections. As more publications move to digital publishing models, there is an opportunity for authors to include supplemental tables or appendices that outline the specific elements of their intervention approach and the way in which clients were progressed through the intervention. Rehabilitation journals may also need to clarify which elements of specificity are required, provide templates for these required elements, and identify which types of articles these requirements apply to.
Interestingly, we found that Level 4 studies tended to include a higher number of ingredients, mechanisms of action, and targets than higher level (i.e., Level 1–3) studies. This was surprising given that Level 1b and Level 2b studies were usually randomized controlled trials or pilot or feasibility studies with more rigorous methods overall compared with the individual case–control (Level 3b) or case-series (Level 4) studies published. The case-based studies with smaller samples may possibly have had more room in the article to describe the intervention, or the intervention was possibly easier to specify when it was able to be tailored to a smaller sample of participants. Although this may be the case, higher levels of evidence often represent work further along the translation continuum and therefore most salient for implementation in practice. For this translation to happen, the published findings of such trials need to be specified in a way that can be comprehended and replicated by clinical practitioners. The RTSS framework provides a means by which researchers can initiate this process and report their interventions in a way that helps to reduce the black box of rehabilitation.
Limitations
The current RTSS manual was published in 2019, and our search spanned the past 20 yr. This contributes to the fact that none of the included studies used the RTSS framework, or its accompanying language, when describing their interventions. This led us to interpret what was described in the article as the elements of specificity (ingredients, mechanisms of action, targets). It is possible that we misinterpreted the authors’ intentions or designations of specific elements of the intervention process. However, this further supports the need for a unified language when reporting on research. The RTSS provides this common language and can be used when reporting interventions, which may contribute to the reduction or even prevention of research misinterpretation.
It is important to note that this review was limited to identifying the elements of specificity present in or omitted from the included studies rather than assessing the effectiveness of the interventions or the rigor of the studies. ASI is an evidence-based intervention used in occupational therapy practice. We chose to evaluate the specificity elements of this intervention because there was a robust body of literature to extract data from. Although gaps were identified in the ASI literature, there are likely greater gaps in the reporting of occupational therapy interventions that are not as robustly documented. There is a need to continue to examine how intervention specificity is reported more broadly across the profession and to improve research reporting more broadly for the translation of research into practice.
Implications for Occupational Therapy Research
This scoping review has the following implications for occupational therapy research: ▪ Gaps identified in research reporting include a lack of specificity regarding the reasoning (mechanism of action) behind ingredients of interventions as well as the desired outcome of the intervention (target). ▪ Researchers can use the RTSS to help fill these gaps because it provides a framework and common language that can be used to describe interventions and may increase research translation.
Conclusion
This scoping review used the RTSS to determine which elements of specificity are most frequently present in and omitted from research using ASI interventions. Of the 22 included studies, all included some specific actions used by the therapist (ingredients); however, these ingredients were only associated with targets and a mechanism of action 11% of the time. The percentage of studies describing how the clients were progressed through the intervention protocol (23%) was similarly low. These findings indicate that researchers consistently omit key details of their intervention that are needed for clinical replication. This omission is a hindrance to the translation of research into clinical practice. Presenting findings using a common language, such as the one provided by the RTSS, could help increase understanding of the clinical reasoning behind interventions, which in turn may increase replication potential.
Supplemental Material
Supplementary material for Studying the Specificity of Research Reporting for Ayres Sensory Integration® Interventions in the Published Literature: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050558.pdf for Studying the Specificity of Research Reporting for Ayres Sensory Integration® Interventions in the Published Literature: A Scoping Review by Ishanie Choudhury, Talicia Tarver, Mary Davis and Stacey Reynolds in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors have no conflicts of interest, funding, or sponsorship to disclose. Stacey Reynolds has served as an advisory board member to the RTSS group as part of a Patient-Centered Outcomes Research Institute–funded project (Principal Investigator: Jeanne Zanca; 2022–present), Award EASCS-24311, “Facilitating Rehabilitation Clinician Uptake of PCOR/CER Results via Improved Research Reporting.” We thank Virginia Commonwealth University Libraries and the Virginia Commonwealth University Department of Occupational Therapy for their support.
* Indicates studies included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.