
Abstract
This study offers preliminary evidence that supports the potential advantages of involving both stroke survivors and their caregivers in a dyad-focused intervention process.
Stroke is a leading cause of long-term disability (GBD Neurology Collaborators, 2019). After discharge, transitioning back into the community is challenging for stroke survivors and their families (Cameron et al., 2008). In most cases, family members are unprepared for the caregiving role and report frustration and dissatisfaction with the transitional care provided by hospitals (Hare et al., 2006; Quinn et al., 2014; Yonaty & Kitchie, 2012). Thus, involving family caregivers in rehabilitation and discharge planning for stroke survivors is crucial to an effective postdischarge transition (Bakas et al., 2014; Lutz et al., 2011).
Despite the importance of caregivers in transitional care, current health care systems are focused on the needs of stroke survivors (Lutz et al., 2011). Caregivers, who often receive little attention from health care providers during stroke recovery, are often considered important resources for stroke survivors (Lutz et al., 2011). Nonetheless, family caregivers are often excluded from the care planning process (Creasy et al., 2015), so many of their needs go unmet. For example, they lack information on stroke recovery and strategies for fulfilling the needs of the individuals under their care (Creasy et al., 2015). This lack of support leaves family caregivers unprepared and isolated, leading to physical and psychological health problems, such as stress, emotional distress, and strain for both stroke survivors and caregivers (Haley et al., 2015; Moon, 2017; Perrin et al., 2009; van Exel et al., 2005).
Dyadic interventions target a survivor and their family caregiver as a pair of active participants (a dyad; Bakas et al., 2014). Dyadic interventions can improve the physical function and cognition of survivors and the well-being of caregivers (Pucciarelli et al., 2021). Although dyadic interventions are designed to be dyad based (i.e., involving both the survivor and their caregiver), they often prioritize the needs of either the survivor or the caregiver (Bakas et al., 2014, 2017; Pucciarelli et al., 2021). Dyadic interventions that address the needs of both survivors and their caregivers in a mutually beneficial manner are not prevalent in the literature (Pucciarelli et al., 2021). Attending to the needs of both the survivor and the caregiver in a dyad can positively contribute to the health outcomes and well-being of both individuals (Bakas et al., 2014, 2017).
Strategy training is a complex behavioral intervention designed to help survivors identify real-life problems and generate and implement problem-solving strategies (McEwen et al., 2010; Skidmore et al., 2011). Strategy training has been shown to reduce disability among stroke survivors (Skidmore et al., 2015, 2017). However, to the best of our knowledge, no study has adopted strategy training to optimize outcomes for both survivors and their caregivers. Empirical research on the feasibility and effectiveness of dyad-focused strategy training is warranted. The findings of such research may contribute to improving care in stroke rehabilitation services and provide a basis for payer coverage decisions.
In the current study, we adopted a dyad-focused strategy training intervention to aid stroke survivors and family caregivers in preparing for the hospital- to-community transition. The aims of this study were to (1) examine the feasibility of adopting our strategy training intervention to survivor–caregiver dyads and (2) evaluate the preliminary efficacy of this intervention for goal achievement, participation, and relationships among survivors and caregivers; the physical and cognitive functions of survivors; and caregiver burden and preparedness.
Method
Intervention Development
Our dyad-focused strategy training intervention was developed with the guidance of the first phase of the Medical Research Council Framework for Developing and Evaluating Complex Interventions (Craig et al., 2013), including (1) identifying current evidence on strategy training and dyadic interventions for stroke rehabilitation; (2) identifying theories, practice standards, or guidelines; and (3) modeling processes and outcomes.
We first performed a systematic search of the literature for articles on strategy training and dyadic interventions addressing stroke survivor and caregiver outcomes. The identified articles were used to outline the critical components of intervention protocols guided by strategy training guidelines (Skidmore et al., 2015), Bodenmann’s (1995) dyadic coping framework, and self-efficacy theory (Bandura, 1986). Next, we established an interdisciplinary panel consisting of 10 experts with backgrounds in medicine, rehabilitation, and psychology. Experts were selected if they had extensive expertise and experience in delivering or investigating interventions for stroke survivors and their caregivers. We then held a series of panel meetings to review and refine the intervention protocols and outcome measures. Finally, we conducted in-depth, one-on-two interviews with eight stroke survivor–caregiver dyads to refine the intervention protocols and assess the acceptability of the intervention and potential challenges related to it. The personal interviewing approach allowed us to obtain a comprehensive understanding of the perspectives of both the survivors and the caregivers, providing nuanced insights and valuable feedback. These perspectives were instrumental in the finalization of the intervention protocols.
Study Design
We conducted this single-group, repeated-measures study with the rehabilitation units of Taipei Medical University Hospital, Wan Fang Hospital, Shuang Ho Hospital, and National Taiwan University Hospital in the greater Taipei region. The participants underwent assessments before (T1) and after (T2) the dyad-focused strategy training intervention, and a final follow-up assessment was conducted 3 mo after the intervention (T3).
This study was approved by the institutional review boards of all participating hospitals, and written informed consent was obtained from all participants.
Participants
We recruited participants from the outpatient settings of four clinical institutions from September 2021 to December 2022. Stroke survivors and their caregivers were recruited if they were age 20 yr or older, could speak Mandarin, and could provide informed consent. Stroke survivors had to have had stroke onset within the previous 6 mo and a family caregiver. Caregivers had to be the primary family caregiver.
A survivor–caregiver dyad was excluded if either the survivor or the caregiver (1) required major medical treatment (e.g., chemotherapy, radiation therapy, hemodialysis, or peritoneal dialysis); (2) had severe aphasia; (3) could not participate in the 1-hr discussion sessions; or (4) had a diagnosis of a psychiatric disorder (e.g., dementia, major depressive disorder, and substance use).
Our trained research staff visited the participating clinical institutions regularly and collaborated with clinical staff at each clinical institution to identify eligible participants. Medical charts were reviewed, and personal interviews were conducted to determine eligibility for enrolment.
Intervention
Our dyad-focused strategy training intervention had five components: shared decision-making, shared goal setting, shared self-evaluation of performance, strategy development and implementation, and therapeutic guided discovery. A trained occupational therapist delivered 12 one-on-two intervention sessions (45-min sessions twice a week over 6 wk) with the survivor–caregiver dyads at their homes or in a quiet room at the participating hospitals. Before commencing interventions, the therapist read the intervention manual, watched a training video, and received an average of 4 hr of standardized training from two experienced occupational therapists from the research team.
Dyad-focused strategy training is a therapist-facilitated, client-directed approach by which dyads can identify their own goals and solve problems in various contexts. During the first two sessions, the therapist introduced dyad-focused strategy training to a participating dyad, noted their background information, and clarified their expectations for the intervention. Next, the therapist assisted the dyad in identifying and prioritizing three to five shared goals using Goal Attainment Scaling (GAS; Turner-Stokes, 2009). In the subsequent sessions, the therapist helped the dyad engage in activities aimed at achieving their established goals and identifying any barriers hindering their achievement. The therapist then provided the dyad with a guided discovery strategy that included (1) setting a goal to address the identified barriers, (2) formulating a plan to address the identified goal, (3) carrying out the devised plan, (4) evaluating whether the executed plan was successful or required adjustment, and (5) generalizing the strategy to other activities. The dyad repeated this process iteratively in subsequent sessions until all the goals were achieved. An outline of the intervention is presented in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Measures
All data were collected in interviews conducted by licensed occupational therapists who received 8 hr of training in data collection by means of standardized training modules. The therapists learned how to administer several standardized assessment tools, such as GAS, the Trail Making Test (TMT), and the Montreal Cognitive Assessment (MoCA), and how to review medical charts, collect self-report data through questionnaires, and conduct qualitative interviews.
Feasibility Indicators
The feasibility indicators used were as follows: ▪ number of dyads recruited and retained ▪ number of intervention sessions attended ▪ participant engagement in the intervention sessions, which was evaluated by the interviewer using the Pittsburgh Rehabilitation Participation Scale, a 6-point Likert-type scale ranging from 1 (no engagement) to 6 (excellent engagement;
Lenze et al., 2004) ▪ participant comprehension of the intervention content, which was evaluated by the interviewer using a 3-point Likert-type scale ranging from 1 (minimal understanding) to 3 (good understanding; Skidmore et al., 2014) ▪ participant satisfaction with the intervention, which was reported by the dyad on the Client Satisfaction Questionnaire (CSQ), an eight-item questionnaire on which 0 to 23 total points indicates poor to fair satisfaction and 24 to 32 total points indicates moderate to high satisfaction (Attkisson & Greenfield, 1994).
Efficacy Measures: Dyadic Outcome Measures
GAS.
The therapist used GAS, a 5-point self-rated scale, to assist the dyads in establishing shared goals and self-assessing the degree of goal achievement from the first to the final intervention session. The dyads assigned scores for goal achievement on a Likert-type scale ranging from −2 (much worse than expected) to 2 (somewhat better than expected). These scores were then weighted by perceived importance and difficulty rating values, which ranged from 0 (not at all important/difficult) to 3 (very important/difficult), with means derived from the ratings provided by both the survivor and the caregiver. GAS scores are reliable, valid measures of goal attainment in rehabilitation contexts (Turner-Stokes, 2009).
Survivor–caregiver relationships.
The Dyadic Relationship Scale (DRS) was used to evaluate the relationship perceptions of survivors and their caregivers. The DRS is a self-report scale with established psychometric properties for both patients and family caregivers (Sebern & Whitlatch, 2007). It has two subscales: Positive Interactions (six items) and Dyadic Strain (five items for caregivers and four items for stroke survivors). Items are rated on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree), with survivors and their caregivers rating the items. The higher the score on each dimension, the more positive the interaction or the higher the level of strain in the dyadic relationship.
Participation.
The Participation Measure–3 Domains, 4 Dimensions (PM–3D4D; Chang et al., 2017) is a self- report instrument used to assess participation performance across Productivity, Social, and Community domains. Both the survivors and their caregivers report the frequency (measured on 5-point and 7-point scales ranging from never to every day or almost every day) and difficulty (measured on a 4-point scale ranging from very difficult to not difficult at all) of their participation. The PM–3D4D scale has demonstrated robust psychometric properties in rehabilitation populations (Chang, 2017; Chang et al., 2017). The higher the score, the higher the increased participation frequency but the lower the perceived difficulty in each domain of participation.
Survivor Outcome Measures
Functional independence.
Survivors’ functional independence was assessed using the Chinese version of the Activity Measure for Post-Acute Care (AM–PAC; Jette et al., 2008). This instrument evaluates difficulty on a 4-point scale across three activity domains: Basic Mobility, Daily Activity, and Applied Cognition. The higher the score, the greater the functional independence. The Chinese version of the AM–PAC has satisfactory reliability and validity (Chang et al., 2018).
Cognitive function.
Survivors’ general cognitive functions were assessed using MoCA (Burton & Tyson, 2015), a 30-point assessment tool. In addition to evaluating global cognitive functions, we measured executive functions because they potentially benefit from strategy training (Skidmore et al., 2015). The TMT (Parts A and B [Trails A and Trails B, respectively]; Koss et al., 1984; Ridley et al., 1978) and the Stroop Color and Word Test (Stroop, 1935) were used to measure executive functions. In particular, we used the TMT (Koss et al., 1984; Ridley et al., 1978) to assess sustained attention, sequencing, mental flexibility, and visual tracking. The time taken to complete the TMT was calculated, with longer completion times indicating poorer outcomes. We used the Stroop test (Stroop, 1935) to measure inhibition, set shifting, and selective attention. The participants were asked to determine whether a word on a colored background indicated the same color as the background as quickly and accurately as possible, and the correction rate was calculated and recorded (Koss et al., 1984; Ridley et al., 1978). These assessments have demonstrated adequate psychometric properties in stroke survivors (Bowie & Harvey, 2006; Burton & Tyson, 2015; Wang et al., 2018).
Caregiver Outcome Measures
Preparedness for caregiving.
The Preparedness for Caregiving Scale (PCS; Archbold et al., 1990) was used to measure caregiver preparedness. The PCS is a self-report questionnaire with eight items, each rated on a 5-point Likert-type scale ranging from 0 (not at all prepared) to 4 (very well prepared). The higher the PCS score, the higher the preparedness for caregiving. The psychometric properties of the PCS have been validated with caregivers of stroke survivors (Pucciarelli et al., 2014).
Caregiver burden.
We used the Zarit Burden Interview (ZBI) to assess caregiver burden across multiple domains. This self-report questionnaire consists of 22 items rated on a 5-point Likert-type scale ranging from 0 (never) to 4 (nearly always). The higher the score, the greater the caregiver burden. The ZBI has demonstrated reliability and validity in a caregiver population (Bachner & O’Rourke, 2007).
Observational Data
Observational data and field notes from the therapists, assessors, and research team meetings were collected and reviewed by the research team throughout the study period.
Statistical Analysis
Quantitative data were analyzed using SAS (Version 9.3). To examine the feasibility of dyad-focused strategy training, we used descriptive analyses to present feasibility outcomes, such as adherence, retention, and engagement. To determine preliminary efficacy, we compared treatment effects between T1 and T2 and between T2 and T3 using the paired t test or the Wilcoxon signed-rank test if the data were not normally distributed, as indicated by the Shapiro–Wilk test. Because each outcome variable was tested twice, statistical significance after Bonferroni correction was set at p < .025 (García-Pérez, 2023). Cohen’s drm was used as an indicator of effect size to account for within-subject repeated measures (Lakens, 2013). Effect sizes of 0.20, 0.50, and 0.80 indicated small, moderate, and large effects, respectively (Cohen, 1988). Given the exploratory nature of the current study, no sample size calculation was performed.
Observational data were analyzed using conventional content analysis, aligning with an inductive approach for describing phenomena (Hsieh & Shannon, 2005). Initially, two coders (Yen-Nun Ling and Te-Hsun Hung) with a background in occupational therapy reviewed the collected data and noted ideas and terms reflecting the content of the data. The two coders then created codes and grouped them into themes. The codes and themes were reviewed by a third researcher (Feng-Hang Chang), and consensus on the codes and themes was reached through discussion among the researchers.
Results
A flowchart of the study process is given in Figure 1. From 2021 to 2022, 16 eligible dyads were recruited and completed baseline assessment; of them, 15 completed the intervention, and 14 completed the follow-up assessments for final analysis. Participants’ demographic and clinical characteristics are provided in Table 1.
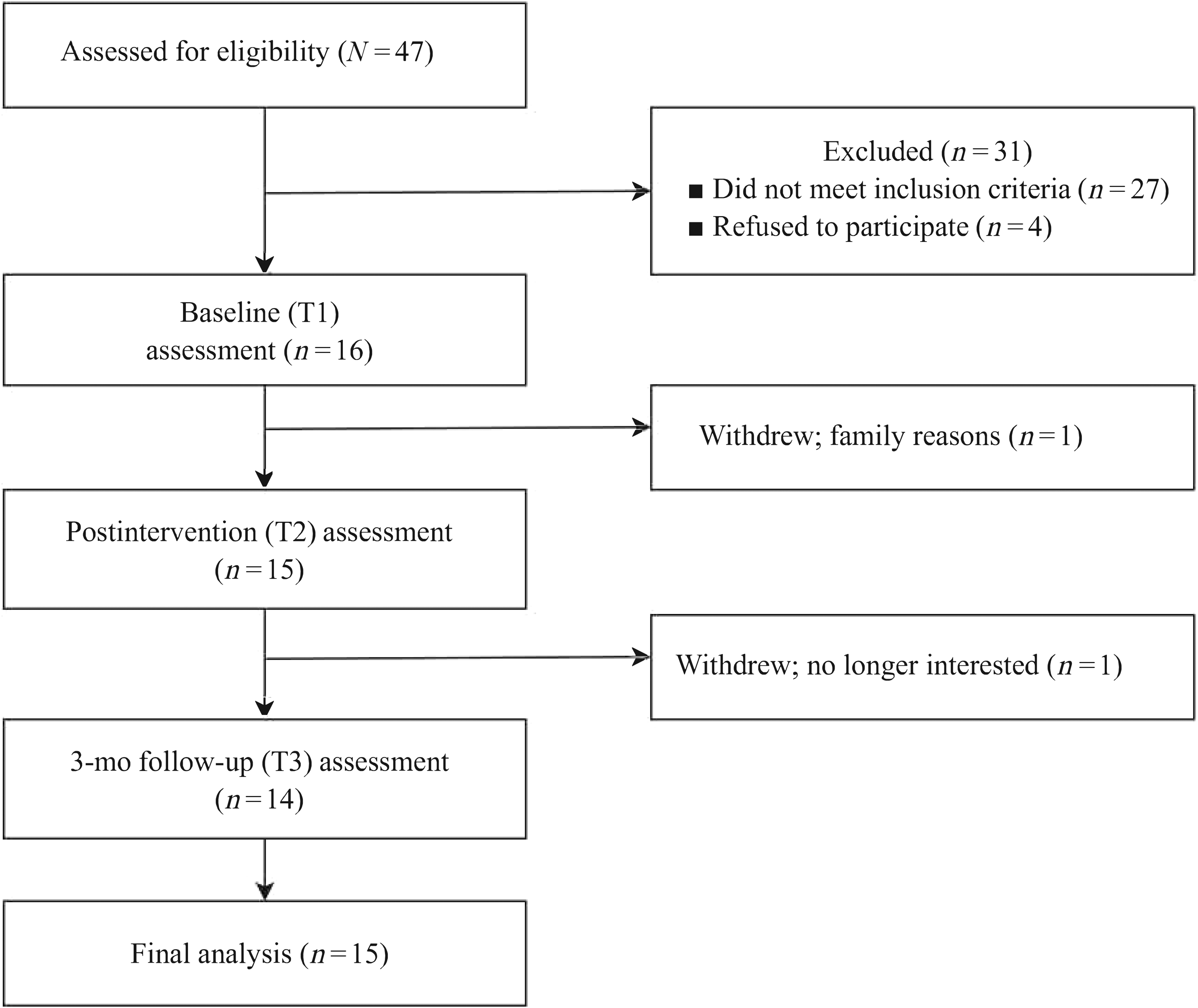
Study flowchart.
Demographic and Clinical Characteristics of Study Participants
Note. MoCA = Montreal Cognitive Assessment; MRS = Modified Rankin Scale; NIHSS = National Institutes of Health Stroke Scale.
Objective 1: Feasibility
In total, 16 dyads completed the baseline assessment; 15 dyads completed all 12 intervention sessions, and 1 dyad dropped out at the fourth session because of family issues (adherence = 93.8%). One dyad was lost to follow-up at T3 (retention = 93.3%). The mean scores for engagement in intervention sessions were 4.6 (SD = 0.9) among the survivors and 4.2 (SD = 1.0) among the caregivers, indicating that the dyads participated in all intervention sessions with adequate effort. The mean scores for intervention comprehension were 2.5 (SD = 0.5) among the survivors and 2.8 (SD = 0.4) among the caregivers, indicating that the dyads had a strong understanding of the intervention. All dyads reported moderate to high satisfaction with the intervention (mean CSQ scores = 26.3, SD = 3.8, for survivors and 27.8, SD = 2.6, for caregivers).
Objective 2: Preliminary Efficacy
Dyadic Outcomes
The changes in outcome scores are presented in Tables 2 and 3. From T1 to T2, significant score changes were observed in several dyadic outcomes: GAS scores improved (M = 38.4, SD = 12.5, drm = 2.0). All goals set by the dyads focused on activities and participation. Survivor community participation also improved significantly, with a mean increase in participation frequency of 0.5 (SD = 0.6, drm = 0.9) and a mean decrease in participation difficulty of 14.6 (SD = 19.9, drm = 0.9). Scores for survivor productive participation frequency (M = 0.2, SD = 0.4, drm = 0.7) and caregiver community participation difficulty (M = 4.3, SD = 18, drm = 0.5) changed with a medium effect size, but the changes were not significant.
Change in Scores Between T1 and T2 (N = 15)
Note. AM–PAC = Activity Measure for Post-Acute Care; DRS = Dyadic Relationship Scale; MoCA = Montreal Cognitive Assessment; PCS = Preparedness for Caregiving Scale; PM–3D4D = Participation Measure–3 Domains, 4 Dimensions; T1 = preintervention assessment; T2 = postintervention assessment; T3 = 3-mo follow-up assessment; TMT = Trail Making Test; ZBI = Zarit Burden Interview.
*p < .025.
Changes in Scores Between T2 (N = 15) and T3 (N = 14)
Note. AM–PAC = Activity Measure for Post-Acute Care; DRS = Dyadic Relationship Scale; MoCA = Montreal Cognitive Assessment; PCS = Preparedness for Caregiving Scale; PM–3D4D = Participation Measure–3 Domains, 4 Dimensions; T1 = preintervention assessment; T2 = postintervention assessment; T3 = 3-mo follow-up assessment; TMT = Trail Making Test; ZBI = Zarit Burden Interview.
*p < .025.
From T2 to T3, most dyadic outcomes remained stable, indicating the sustained effectiveness of the intervention over time; however, a significant increase in scores for difficulty participating in productivity-related tasks was observed among caregivers (M = −15.2, SD = 17.8, drm = 1.1; see Figure A.1 in the Supplemental Material for details).
Survivor Outcomes
From T1 to T2, several variables demonstrated significant improvement, including Trails A completion time (M = −36.0, SD = 57.8, drm = 1.0), Trails B completion time (M = −32.0, SD = 41.3, drm = 1.8), the Stroop test (incongruent) correction rate (M = 0.2, SD = 0.2, drm = 1.1), and the AM–PAC (Basic Mobility dimension; M = 7.6, SD = 9.4, drm = 1.3). From T2 to T3, Trails A completion time (M = −12.7, SD = 16.5, drm = 1.6) continued to exhibit significant improvement, whereas other survivor outcome variables remained stable.
Caregiver Outcomes
From T1 to T2, preparedness for the caregiving role improved significantly, with a mean increase on the PCS of 4.9 (SD = 5.2, drm = 1.1). Both PCS and ZBI scores remained stable from T2 to T3.
Observations
In the content analysis of the observational data, two themes emerged: (1) changes in the dyads and (2) challenges implementing the intervention. An overview of the key themes and representative quotes identified through the interviews is available in Table A.2 in the Supplemental Material.
Changes in the Dyads
Changes were observed in the participating dyads, including improved communication, boosted confidence, improved problem-solving capabilities, enhanced participation, and increased autonomy and empowerment. Both the survivors and their caregivers experienced increased comfort in communication, which facilitated a deeper understanding of each other’s desires. For instance, one survivor initially suggested a goal of relocating to a rural area; however, during the goal-setting process, the caregiver expressed her desire to work in the city. Consequently, the dyad established a mutual goal of regularly taking trips to the rural area. Both the survivors and their caregivers experienced growth in self-confidence throughout the Goal–Plan–Do–Check process. Several dyads discovered that they could accomplish challenging tasks that they did not believe they could perform; this led to a considerable boost in their confidence and belief in their abilities. During this process, both the survivors and their caregivers reported improvements in their problem-solving capabilities; increased participation in work, leisure, and other meaningful activities; and a growing sense of autonomy and empowerment.
Challenges in Implementing the Intervention
Our research therapists noted several challenges during the intervention, including dyadic relationships being conflicting, caregivers focusing on survivors’ needs, and survivors being resistant to change. The dyadic relationship can significantly influence the intervention process, particularly when a power imbalance occurs. Moreover, most caregivers were not used to expressing their needs and expectations. They tended to ignore their own needs and prioritize those of the survivors. The field notes revealed that caregivers had difficulty identifying goals crucial to them. The caregivers frequently had to be encouraged to share their thoughts and express their needs during the intervention so that mutual agreement between caregivers and survivors could be reached.
Discussion
Our dyad-focused strategy training intervention is innovative in that it addresses the needs of both stroke survivors and their caregivers during the hospital-to-community transition. In the current study, the participating dyads demonstrated high attendance, engagement, and retention rate, indicating that our dyadic intervention may be feasible at the postacute stage not only for stroke survivors but also for their caregivers. All participating dyads accomplished their goals over the 12 sessions; these results are similar to those of strategy training for stroke survivors alone. All dyads reported moderate to high satisfaction with the intervention. Several participants anecdotally expressed appreciation for the intervention, which motivated them to discover their capabilities and participate in more activities.
In general, our dyad-focused strategy training intervention demonstrated positive effects on both dyadic and individual outcomes. The improvement in GAS scores indicated that the dyads effectively achieved the goals they set during dyad-focused strategy training. This finding corroborates those of studies investigating the effectiveness of strategy training on stroke survivors, indicating significant improvements in performance of self-selected goals (Ahn et al., 2017; Lin et al., 2020; Poulin et al., 2017). Our results also revealed the effectiveness of strategy training in helping dyads achieve their goals. All goals set by the dyads were related to activities and participation, reflecting the major needs of stroke survivors and their caregivers during the poststroke transitional stage.
Even though our results are preliminary, our intervention led to significant improvements in the cognitive functions, basic mobility, and community participation of survivors and in the preparedness of caregivers; after the intervention, these improvements either persisted or increased. For instance, survivor community participation and basic mobility performance were sustained after the intervention, and survivor executive functions, assessed using the TMT, exhibited continuous improvement even at the final follow-up assessment. These findings, along with those reported previously (Pucciarelli et al., 2021), corroborate the positive effects of dyadic interventions on the outcomes of both stroke survivors and their caregivers. The improvements observed in the survivors’ functional capacities and cognitive abilities support the findings of other studies that have used strategy training with stroke survivors (Lin et al., 2020; Poulin et al., 2017; Skidmore et al., 2015). Our results provide additional evidence supporting the ability of dyad-focused strategy training interventions to increase caregiver preparedness for the transition to community life. However, in the current study, caregivers reported an increase in perceived difficulty in productive participation after the intervention. This result indicates that after the intervention, caregivers may encounter difficulties as they engage in productive activities, such as returning to work or volunteering. Further investigation of these difficulties and identification of the necessary support required by caregivers after the intervention is warranted.
Our research therapists observed that, in addition to improvements in the quantitative outcome measures, the participating dyads demonstrated benefits of the intervention, such as increased comfort in communication and enhanced confidence. Our findings are consistent with those of studies that implemented strategy training with patients with stroke and brain injury (Chang et al., 2022; Chiu et al., 2023). Individuals perceived a boost in confidence and self-efficacy as they gained valuable insights into their strengths and limitations through strategy training. Consequently, they demonstrated improved performance in activities of daily living and increased their participation in the community (Kleitman & Stankov, 2005; Öhrvall et al., 2019). Our findings highlight not only the effects of strategy training but also the interdependent nature of the dyadic relationship through which both stroke survivors and their caregivers foster trust and confidence in each other. Future studies should examine the effects of dyad-focused strategy training interventions on the self-efficacy of survivors and their caregivers.
Our research therapists also reported challenges in implementing the intervention. Several caregivers were accustomed to fulfilling the role of supporter and felt uncomfortable when asked to express their own expectations and needs. In conventional rehabilitation practice, a caregiver is typically considered a resource for the patient rather than a care receiver (Lutz et al., 2011). The caregivers were unfamiliar with the dyad-focused intervention, which mandates active involvement from both survivors and their caregivers. Given the novelty of this approach, the caregivers in this study required a substantial amount of time to acclimate. Nevertheless, this challenge is not unique to dyad-focused behavioral interventions (Lutz et al., 2011). To facilitate the adaptation of a dyad to this approach, therapists must assist dyad members in comprehending the importance of active participation from both individuals and exert additional effort in encouraging their engagement.
Study Limitations
Our study sample consisted of a limited number of participants recruited exclusively from urban areas, limiting the generalizability of our findings. Given the nature of this research as a feasibility study, we adopted a single-group design aimed at estimating effect sizes to inform future clinical trials. As such, the study was not structured to determine the statistical significance of temporal changes. Furthermore, because of the preliminary nature of the study, our analysis did not control for confounding variables; cautious interpretation of the results is necessary. Notably, false-positive results may arise as a consequence of conducting multiple comparisons. Nevertheless, our preliminary findings afford additional insight into the favorable effects of a strategy training intervention on both stroke survivors and their caregivers and may be useful for refining future interventions. Consequently, large-scale randomized controlled trials assessing the effectiveness of similar interventions, including their optimal lengths and intensities, are required.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ The feasibility and acceptability of dyad-focused strategy training for stroke survivors and their caregivers in Taiwan highlight the potential for its successful implementation in rehabilitation settings. ▪ Dyad-focused strategy training can address the needs of stroke survivors and their caregivers, thus aiding them in achieving shared rehabilitation goals. ▪ The positive effects of dyad-focused strategy training on the cognitive functions, activity performance, and community participation of stroke survivors and on caregiver preparedness emphasize the intervention’s potential benefits for both members of survivor–caregiver dyads. Furthermore, the possibility of persistent effects after the intervention suggests long-term advantages. ▪ Recognizing caregivers as more than just supporting resources for stroke survivors is essential in rehabilitation practice. Acknowledging caregivers’ health and specific needs can lead to more effective, holistic care for both stroke survivors and caregivers.
Conclusion
The results highlight the feasibility of dyad-focused strategy training interventions for stroke survivors and their caregivers. In particular, our intervention improved preliminary dyadic, survivor, and caregiver outcomes. Large-scale randomized controlled trials are necessary to validate our findings.
Supplemental Material
Supplementary material for Development of a Dyad-Focused Intervention for Stroke Survivors and Their Family Caregivers: A Feasibility Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050571.pdf for Development of a Dyad-Focused Intervention for Stroke Survivors and Their Family Caregivers: A Feasibility Study by Yen-Nung Lin, Te-Hsun Hung, Juleen Rodakowski, Jiunn-Horng Kang, Der-Sheng Han, Tsan-Hon Liou, Yi-Hsuan Wu and Feng-Hang Chang in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
Yen-Nung Lin and Te-Hsun Hung contributed equally to this manuscript. We thank the participating hospitals: Taipei Medical University Hospital; Wan Fang Hospital; Shuang Ho Hospital, Taipei Tzu Chi Hospital; National Taiwan University Hospital, Bei-Hu Branch; and National Taiwan University Hospital. We also acknowledge Hong-Wei Lin and Tz-Ting Huang for their help with data collection. This research was funded by grants from the Ministry of Science and Technology, Taiwan (MOST111-2628-B-038-015-MY3) and Taipei Medical University, Wan Fang Hospital (112TMU-WFH-12 and 110TMU-WFH-03112).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.