
Abstract
This is the first study to review the effectiveness of the Canadian Occupational Performance Measure (COPM) to determine the success of occupational therapy interventions for people with a frozen shoulder.
A frozen shoulder (adhesive capsulitis) is characterized by inflammation and contraction of the shoulder joint capsule, causing pain, stiffness, and restricted joint movement (Neviaser & Neviaser, 2011). Its incidence ranges from 2% to 5%, with a higher occurrence among women and those ages 40 to 60 yr (Ramirez, 2019). The incidence of frozen shoulder increases for patients with conditions that limit arm movement, such as breast resection, diabetes, hypothyroidism, trauma, or surgery (Jain & Sharma, 2014; Ramirez, 2019). A frozen shoulder progresses through freezing, frozen, and thawing stages (Jain & Sharma, 2014; Ramirez, 2019), lasts for 12 to 42 mo, and potentially causes long-term disability (Jones et al., 2013).
Medical professionals may have underestimated the impact of frozen shoulder, leading to delayed diagnosis and inadequate treatment. A patient’s suffering and limitations in daily activities, work, and social participation are often overlooked (Jones et al., 2013; Lyne et al., 2022). However, the pain and disability significantly affect the patient’s quality of life (QOL; Le et al., 2017). Frozen shoulder can disrupt sleep and affect activities of daily living, such as grooming, driving, and doing household chores, potentially forcing occupational modifications and job loss (Bouaicha et al., 2020; Jones et al., 2013). Consequently, it is important to understand a patient’s experiences and treatment priorities (Jones et al., 2013).
The Canadian Occupational Performance Measure (COPM) identifies occupational priorities and tracks changes in patients’ perceptions of performance and satisfaction (Law et al., 1998). Through individualized goals, therapists engage patients and strengthen their therapeutic relationships (Roe et al., 2020).
The COPM manual, initially established in a mental health environmental program study involving 49 adults (Mirkopolous & Butler, 1994), specifies that a change of 2 points or more in COPM Performance and COPM Satisfaction scores is clinically important (Law et al., 2014). However, its clinical significance has not been validated. Moreover, the validity of a consistent minimal clinically important difference (MCID) across diagnoses, disability severity, age, and various dimensions of COPM Performance and Satisfaction has been debated (McColl et al., 2023; Tuntland et al., 2016).
The MCID represents the score change in the health domain that patients consider significant. This difference is significant for altering the course of treatment and can provide a basis for assessing the clinical importance of test results and clinical decision-making (Jaeschke et al., 1989). The methods for establishing an MCID usually involve anchor- and distribution-based approaches (Hays & Woolley, 2000). In this study, we aimed to estimate the MCID and responsiveness of patients with frozen shoulder using anchor- and distribution-based methods.
Method
Participants
This study, a subset of a prospective randomized controlled trial, enrolled patients from two physical medicine and rehabilitation clinics from March 2020 to December 2021 (Yeo et al., 2021). The inclusion criteria were (1) age ≥19 yr and (2) a difference of ≥30° between the affected and unaffected shoulders in two or more movements when measured passively in the supine position during forward flexion, abduction, and external rotation at 90° shoulder abduction (Chan et al., 2013). The exclusion criteria were (1) bilateral frozen shoulder (Kelley et al., 2013), (2) secondary frozen shoulder caused by trauma (shoulder fracture or dislocation) or inflammatory disease (rheumatoid arthritis; Chan et al., 2013; Kelley et al., 2013), (3) inability to exercise because of deconditioning, and (4) communication difficulties as assessed by the researcher (Ji Hye Hwang, Ji Young Lim). The study was approved by the institutional review boards at Samsung Medical Center and Seoul St. Mary’s Hospital (SMC-2019–05–021 and KC20ENDI0154), and all participants provided signed informed consent.
During the study intervention, the participants received hospital-based therapy and a home exercise program for 3 mo. The distinction between the groups lies solely in the method of performing the exercises at home, with no differences in the content or type–duration of the prescribed exercises. The exercise regimen was structured into three stages, corresponding to the different phases of frozen shoulder. The exercise content at each stage was determined from existing literature (Kelley et al., 2013).
Of the initial 100 participants, 1 participant withdrew, 3 participants dropped out because of an inability to perform the exercise according to the predetermined criteria, and 2 participants were lost to follow-up. Therefore, data from 94 participants were analyzed.
Outcome Measures
We measured outcomes at baseline, three times during the intervention (at 1, 2, and 3 mo), and twice postintervention (at 4.5 and 6 mo), with 7- to 15-day deviations allowed for each assessment. A physician evaluated frozen shoulder stage at each follow-up visit and prescribed stage-appropriate exercises. Assessments were conducted by the same evaluators who were blinded. For data analysis, we used data from all assessments conducted at baseline and at the conclusion of the intervention (3 mo).
The COPM involved patients identifying priority issues, selecting three to five occupations, and assessing their performance and satisfaction before and after the intervention. Scores between 1 and 10 were given to each item (Law et al., 1990), and item scores were averaged for performance and satisfaction.
Criterion Measures
We conducted measurements on the same day as the COPM assessment. All assessments were conducted using tools translated into Korean after acquiring usage permissions and official licenses.
We obtained supine measurements of the passive and active ranges of motion of the affected shoulder with the participants in the supine position. We measured shoulder forward flexion, abduction, and external and internal rotations at 90° of shoulder abduction using an electronic goniometer (Kelley et al., 2013). We evaluated the pain intensity at rest and during activity for the previous week using an 11-point rating scale, ranging from 0 = no pain to 10 = the worst possible pain (Hartrick et al., 2003).
The Shoulder Pain and Disability Index (SPADI) is a self-reported questionnaire measuring pain and disability associated with shoulder pathology. It comprises two subscales with a total of 13 items (5 items for Pain subscale and 8 items for Disability subscale), scored from 0 = no pain at all, no difficulty to 10 = worst pain imaginable, so difficult that I required help. The scores range from 0 to 130, with 0 indicating absence of shoulder disability (Roach et al., 1991). Notably, the SPADI demonstrated substantial discriminatory capacity, as evidenced by area under the curve (AUC) values ranging from 0.74 to 0.85, underscoring its significance in frozen shoulder and rotator cuff disease (Furtado et al., 2022; Thoomes-de Graaf et al., 2016). Given the availability of the Korean version and robust evidence supporting its high-quality psychometric properties, the SPADI is recommended for monitoring shoulder diseases in Korean clinical practice (Kim, 2023; Seo et al., 2012).
We assessed the patients’ current health status using the EuroQol 5-Dimension 5-Level (EQ–5D–5L) questionnaire. The EQ–5D–5L consists of five questions on mobility, personal care, daily activities, pain–discomfort, and anxiety–depression. Each question was rated from 1 = no problems to 5 = extreme problems (Kim et al., 2016).
We used the Short Form 36 Health Survey (SF–36) to assess health-related QOL. Raw scores on eight scales (Physical Functioning, Physical Role, Body Pain, General Health, Vitality, Social Functioning, Emotional Role, and Mental Health) were computed and transformed into a 0-to-100 scale, with higher scores representing better health-related QOL (Ware & Sherbourne, 1992).
Data Analysis
Responsiveness
We examined responsiveness using effect size (ES) and standardized response mean (SRM). ES was defined as the change in the COPM pre–post score divided by the standard deviation of the baseline score. The SRM was defined as the COPM pre–post score change divided by the standard deviation of the score change (Husted et al., 2000). To classify the magnitude of the responsiveness, we used the Cohen criterion. Responsiveness was interpreted as small (<0.5), moderate (0.5 to 0.8), large (>0.8; Cohen, 1992), very large (>1.2), and huge (>2.0; Sawilowsky, 2009).
MCID
To determine the MCID for the COPM, we analyzed the data from baseline and 3-mo postintervention using anchor-based and distribution-based methods (Ousmen et al., 2018). The distribution-based MCID equation was derived as follows: (1) 0.5 SD method: MCID = 0.5 SD of the change score, (2) effect-size method: MCID = (0.2, 0.5, or 0.8) × baseline SD. For ES, values of 0.2, 0.5, and 0.8 defined small, moderate, and large changes, respectively (Wright et al., 2012).
Anchor-based measures require an independent standard or anchor that is interpretable and moderately correlated with the instrument being explored (Guyatt et al., 2002). We used Spearman’s correlation analysis for anchor selection (Zhang et al., 2023). Correlations with the COPM were interpreted as small (|r| = .1), moderate (|r| = .3), or large (|r| = 0.5; Cohen, 2013). The correlation coefficient should ideally exceed .3 to .35, ensuring a meaningful association between the anchor and the measurement instrument (Revicki et al., 2008). The anchor-based MCID was determined using the receiver operating characteristic (ROC) curve method. ROC curve analysis was used to measure the AUC to determine the cutoff point. The AUC was interpreted as excellent (90–100), good (80–90), fair (70–80), poor (60–70), or fail (50–60; Hosmer et al., 2013; Safari et al., 2016).
Results
Table 1 summarizes the demographic and clinical characteristics of the patients with frozen shoulder at baseline. Most participants (92.6%) were female, with a mean age of 52.3 yr (SD = 7.0). Among the patients with frozen shoulder, 50.0% and 48.9% were in Stages 1 and 2, respectively. Mean COPM Performance score was 5.3 (SD = 1.5), whereas mean COPM Satisfaction score was 4.8 (SD = 1.8).
Participant Characteristics and Outcome Measure Scores (N = 94)
Responsiveness
Significant changes in ES and SRM were observed in the COPM. The ES and SRM results showed that the COPM Performance had values of 2.02 and 1.84, respectively, and the COPM Satisfaction had values of 1.82 and 1.93, respectively. The COPM indicated very large to huge responsiveness in terms of both performance and satisfaction.
MCID
The distribution-based MCID calculated using the ES method resulted in COPM Performance and COPM Satisfaction scores of 0.29 and 0.36 (for an ES of 0.2), 0.73 and 0.90 (for an ES of 0.5), 1.17 and 1.44 (for an ES of 0.8), respectively. The 0.5 SD method yielded. The 0.5 SD method yielded COPM Performance and COPM Satisfaction scores of 0.8 and 0.84 (Table 2).
Area Under the Receiver Operating Characteristic Curves for Each Outcome at 3 Mo
Note. SPADI = Shoulder Pain and Disability Index; COPM = Canadian Occupational Performance Measure; AUC = area under the curve; CI = confidence interval.
The correlations between the COPM score at baseline, scores of each assessment tool at baseline, the COPM score changes at 3-mo postintervention, and the score changes of each assessment tool at 3-mo postintervention are presented in Table 3. As anchor, we chose SPADI, which demonstrated a significant correlation of ≥0.3 across all subdomains and time points. An anchor value of 8 was selected from the SPADI cutoffs of 8 (Paul et al., 2004; Roy et al., 2009) and 13.2 (Roy et al., 2009; Schmitt & Di Fabio, 2004), considering its higher sensitivity and specificity. Using the Youden criterion (Ware & Sherbourne, 1992; Willke et al., 2004), the optimal ROC cutoff values for COPM Performance and COPM Satisfaction were fair, at 0.78 (95% confidence interval [CI] [0.64, 0.91]) and 0.76 (95% CI [0.60, 0.91]), respectively, with cutoff values of 2.5 and 2.1 (see Table 2 and Figure 1).
Correlations With COPM at Baseline and 3-Mo Change Score
Note. COPM_P = Canadian Occupational Performance Measure Performance; COPM_S = Canadian Occupational Performance Measure Satisfaction; ADL = activities of daily living; SF = social functioning; RE = role emotional.
p < .05.
p < .01.
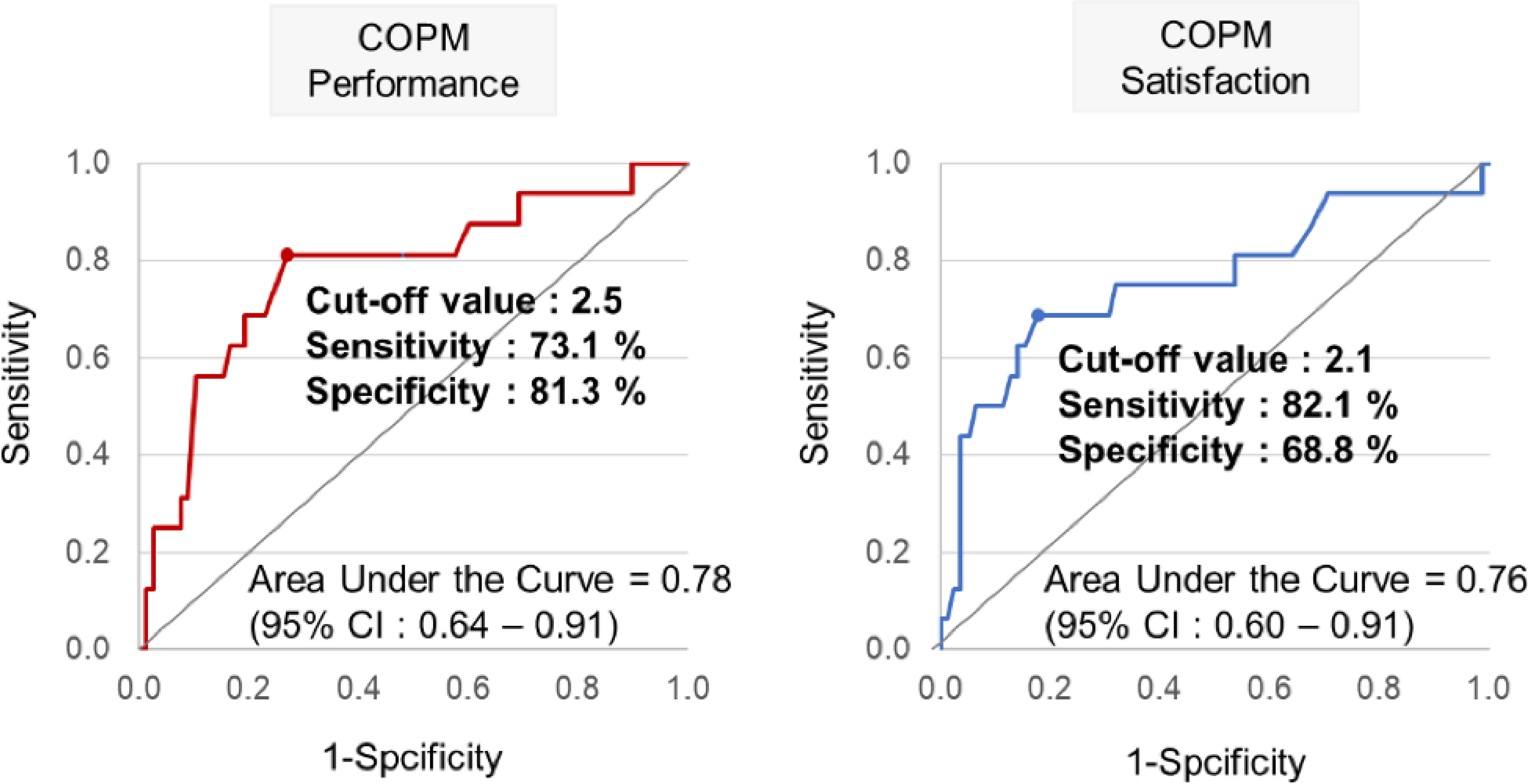
Receiver operating characteristic curve at 3 mo.
Discussion
To the best of our knowledge, this is the first report of COPM responsiveness and MCID for patients with frozen shoulder. Although the COPM is widely used across diverse patient groups, establishing the responsiveness and MCID of the COPM for patients with frozen shoulders is crucial for evidence-based practice, particularly when considering the clinical focus of occupational therapeutic interventions for movement and daily activities. This study aimed to support evidence-based practice by establishing responsiveness and MCID of the COPM for patients with frozen shoulders.
In this study, we computed the SRM and ES to compare the baseline with postintervention measures. Cohen (1992) defined ES as 0.8; the SRM and ES (1.82–2.02, respectively) observed in our study exceeded this threshold. Consequently, we used Sawilowsky’s (2009) extended criteria to interpret responsiveness. Although Ohno et al. (2021) analyzed 10 studies for COPM responsiveness in systematic reviews, only 2 studies met the criteria, suggesting that COPM might not detect changes among patients before and after interventions (Ohno et al., 2021). However, our results indicated that the COPM effectively detected changes among patients with frozen shoulder. Additionally, in studies focusing on patients with frozen shoulder, the SPADI SRM (1.62–1.81) showed better responsiveness than the range-of-motion SRM (0.85–1.38; Tveitå et al., 2008). Therefore, it can be concluded that COPM was able to detect changes among patients with frozen shoulder at a significant level (huge responsiveness), akin to the SPADI.
Although the COPM manual suggests a 2-point change as clinically important (Law et al., 2014), various studies have reported the following different thresholds: 0.9 to 1.9 points for outpatient intervention (Roe et al., 2020), 3 points for older adults (Tuntland et al., 2016), and 4.3 to 4.1 points for thumb osteoarthritis (Raquel et al., 2021). These results indicate that MCID values are not constant (Page et al., 2019) and should be assessed across diverse populations.
This study used two methods to determine the MCID of the COPM. Distribution-based approaches rely on sample statistics to calculate the changes beyond random fluctuations. However, relying solely on statistical perspectives does not scientifically explain the MCID (Revicki et al., 2008). Using multiple strategies is likely to enhance the interpretability of any specific instrument (Guyatt et al., 2002; Hays & Woolley, 2000). Consequently, the MCID determined by anchor- and distribution-based approaches were 2.5 and 1.17 for performance change scores, respectively, and 2.1 and 1.44 for satisfaction change scores, respectively. The minor discrepancies between the two approaches can be attributed to the inherent characteristics of each method.
According to recent systematic reviews and meta-analyses (Challoumas et al., 2020), frozen shoulder is assessed in terms of pain, function, range of motion, satisfaction, and QOL. Pain was assessed using a numeric rating scale and visual analog scale, function was assessed using the Shoulder Disabilities Questionnaire and SPADI, and QOL was assessed using the EQ–5D–5L and SF–36. However, areas related to participation in activities of daily living were not evaluated. Phenomenological studies have shown that individuals with frozen shoulders experience a loss of independence in both home and work settings. Disabilities hinder their ability to perform daily activities, engage in sports, and participate in family activities, thereby limiting their previous roles. Moreover, they reported difficulties in driving or using public transportation, thus reducing their scope of activity. Existing assessment tools appear limited in their ability to address these issues. Considering these limitations, COPM appears to be a suitable assessment tool.
Limitations
This study had some limitations. First, the small sample size may have affected the accuracy of MCID estimation. In addition, many patients with frozen shoulder in this study had a history of breast cancer, possibly because this study was conducted at a tertiary hospital. This may affect the generalizability of our findings to other populations. Despite the small sample size, the AUC was acceptable, allowing us to use an anchor-based ROC approach. Although this anchor demonstrates substantial discriminatory ability, it does not directly capture clinically meaningful changes (Wyrwich & Norman, 2023). On the other hand, the distribution-based approach has limitations, because it may vary on the basis of participant variability at baseline and follow-up assessments (Guyatt et al., 2002).
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: ▪ It is important to consider the COPM MCID as an index to determine the success of interventions for patients with frozen shoulders. ▪ The results suggest that a change of score >2.5 for COPM Performance and 2.1 points for COPM Satisfaction may be a measure of meaningful change for people with frozen shoulders. ▪ Clinical practitioners should cautiously interpret the COPM MCID because the MCID estimation can vary according to the method and sample used.
Conclusion
This study investigated the responsiveness of the COPM Performance and COPM Satisfaction scales using anchor- and distribution-based approaches to explore the MCID. The COPM demonstrated sensitivity in detecting changes among patients with frozen shoulders. The MCID values with the COPM scale were determined as 2.5 for Performance and 2.1 for Satisfaction. These findings can inform the interpretation of COPM scores in clinical and research settings, guide interventions, and facilitate research planning for individuals with frozen shoulder.
Footnotes
Acknowledgments
This study was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute funded by the Ministry of Health and Welfare, Republic of Korea (Grant HI19C0781).