
Abstract
This article adds to the literature on administrative supports for clinical and quality improvement research by illustrating a specific example of how documentation of dose can be shared from one institution to another.
Documentation of therapy services serves several purposes, including tracking a client’s progress and obtaining reimbursement from insurance companies (Davidson et al., 2004). Despite the importance of documenting services, therapists often report dissatisfaction with documentation requirements (Blau et al., 2002; Lau et al., 2016; Quinn & Gordon, 2015). Experts in the field of rehabilitation have stressed the need for data from the point of care to advance care to inform policy and practice (Bettger et al., 2018; Graham et al., 2018; U.S. Department of Health and Human Services, 2021). In addition, standardizing the way practitioners document would support the collection of data to study the effects of rehabilitation intervention (American Physical Therapy Association, 2022). The lack of standardized documentation across settings to describe what happens in a treatment session creates a barrier to utilizing data to improve care and inform policy and practice (Bettger et al., 2018).
More specifically, it is important to document the ingredients or dose delivered at each session in a consistent manner (Kolobe et al., 2014). The American College of Sports Medicine defines dose as frequency, intensity, time, and type (FITT; Liguori & American College of Sports Medicine, 2020). A research summit on the topic was held in 2014, resulting in a published path model to study the effects of dose on outcome (Gannotti et al., 2014). In 2021, Cincinnati Children’s Hospital Medical Center (henceforth referred to as the original institution) set out to standardize how therapy practitioners document dose elements at each session. Utilizing quality improvement methods, this institution successfully increased documentation of dose elements starting with physical therapists in the pediatric outpatient hospital-based clinic by using standardized dose documentation built in a flowsheet in the electronic health record (EHR) system Epic (FITT® Epic Flowsheet; Bailes et al., 2019). Since the initial efforts, this system has spread across the original institution to all physical and occupational therapists and to patients with all conditions and seen in all settings (e.g., inpatient, home health). Data mined from EHR systems are being used to characterize details of interventions delivered to children with various conditions, including cerebral palsy (Bailes et al., 2021), and to children with low back pain at the site (Hobart et al., 2023). Although successful at the initial institution, spreading the FITT Epic Flowsheet to other centers has not yet been described.
Use of the FITT Epic Flowsheet can build capacity for examining clinical care in pediatric rehabilitation. Previous trials using practice-based evidence methodology have yielded information on the care delivered in real-world settings for specific diagnoses. For example, Horn and colleagues (Beaulieu et al., 2015 ; Horn et al., 2015) captured the variation in physical, occupational, and speech language pathology treatment delivered to patients with traumatic brain injury at 10 different sites across the United States. A similarly designed study (Effgen et al., 2016; Jeffries et al., 2019; Mccoy et al., 2018) of school-based physical therapy practice linked dosage of physical therapy to child outcomes. In both studies, clinicians used paper point-of-care forms (in addition to their regular documentation) to document the details of the intervention provided. One limitation to conducting this type of work on a larger scale is the lack of discrete and standardized documentation of pediatric occupational and physical therapy services incorporated into the regular workflow and documentation practice across various institutions. As other authors have stated, improving interoperability of clinical data can optimize the impact of health care by enabling sharing of information between entities (Doll et al., 2021). In addition, the use of common data elements and Fast Healthcare Interoperability Resources data standards in EHR systems can help bolster the ability to share data and draw broader conclusions from data collected during clinical care (Ayaz et al., 2021). Although these data standards are captured in many areas of the EHR, Epic flowsheets provide additional ways to customize documentation to collect supplemental data specific to pediatric rehabilitation that may not be tied to other standard vocabularies but can be used for data sharing between institutions. Shared documentation systems would build capacity for future pragmatic trials, which are urgently needed to study dose in various populations of children treated by pediatric occupational and physical therapy practitioners and determine which interventions result in best outcomes.
The purpose of this quality improvement study was to spread discrete documentation of dose of therapy services (i.e., using the FITT Epic Flowsheet) in usual care from the original institution to a second institution (henceforth referred to as the spread institution) using the spread framework described by Langley et al. (2009). The rationale was that by having similar documentation between institutions, there would be increased capacity to build reports and combine data for clinical, quality improvement, and research applications. This can facilitate larger multisite projects in the future, leading to better outcomes for more patients. In addition, clinician experience from the original institution suggested that this type of documentation of dose of therapy using discrete data elements was more efficient than a traditional narrative progress note.
In this article, we describe the steps taken to spread the FITT Epic Flowsheet to another large pediatric tertiary care center to improve documentation of what happens in a session. This study was determined to be not human subjects research by the spread institution’s institutional review board.
Method
Context
Both the original institution (i.e., where the FITT Epic Flowsheet was developed) and the spread institution (i.e., where the FITT Epic Flowsheet was later implemented) were pediatric tertiary care facilities located in the midwestern United States. The institutions were of similar size and patient volume, comprising multiple outpatient care centers located around their respective metropolitan areas. Both institutions used the same EHR Epic system. Epic has a community library that medical centers can use to share their EHR build specifications with each other, which allowed the spread institution’s Epic specialist (Amy Brunelle) to create a similar flowsheet (the FITT Epic Flowsheet) for both the occupational and physical therapy departments in a new environment.
The FITT Epic Flowsheet captured each of the elements of therapy dose: frequency, intensity, time, and type. Frequency of therapy was selected at each visit using a preset list of common frequencies (e.g., weekly, every other week, monthly). Intensity was captured using the Child Effort Rating Scale (adapted from Beaulieu et al., 2015). Time was captured using minutes of therapy spent on each focus area (original institution) or times billing codes (spread institution). Type was captured through a list of interventions that were categorized by subtype. The occupational therapy FITT Epic Flowsheet is shown in Figure 1, whereas the original institution’s physical therapy FITT Epic Flowsheet is available in a previous publication (Bailes et al., 2019). The flowsheet contained discrete fields that can be built into a report in Epic. Each field of the flowsheet had a unique identifying number in Epic that allowed a data analyst to retrieve documented fields of interest, such as a patient’s level of effort. In contrast, other types of fields (such as free text) in Epic were not as easily quantified and were therefore not able to be queried easily to gather data for research or quality improvement purposes.
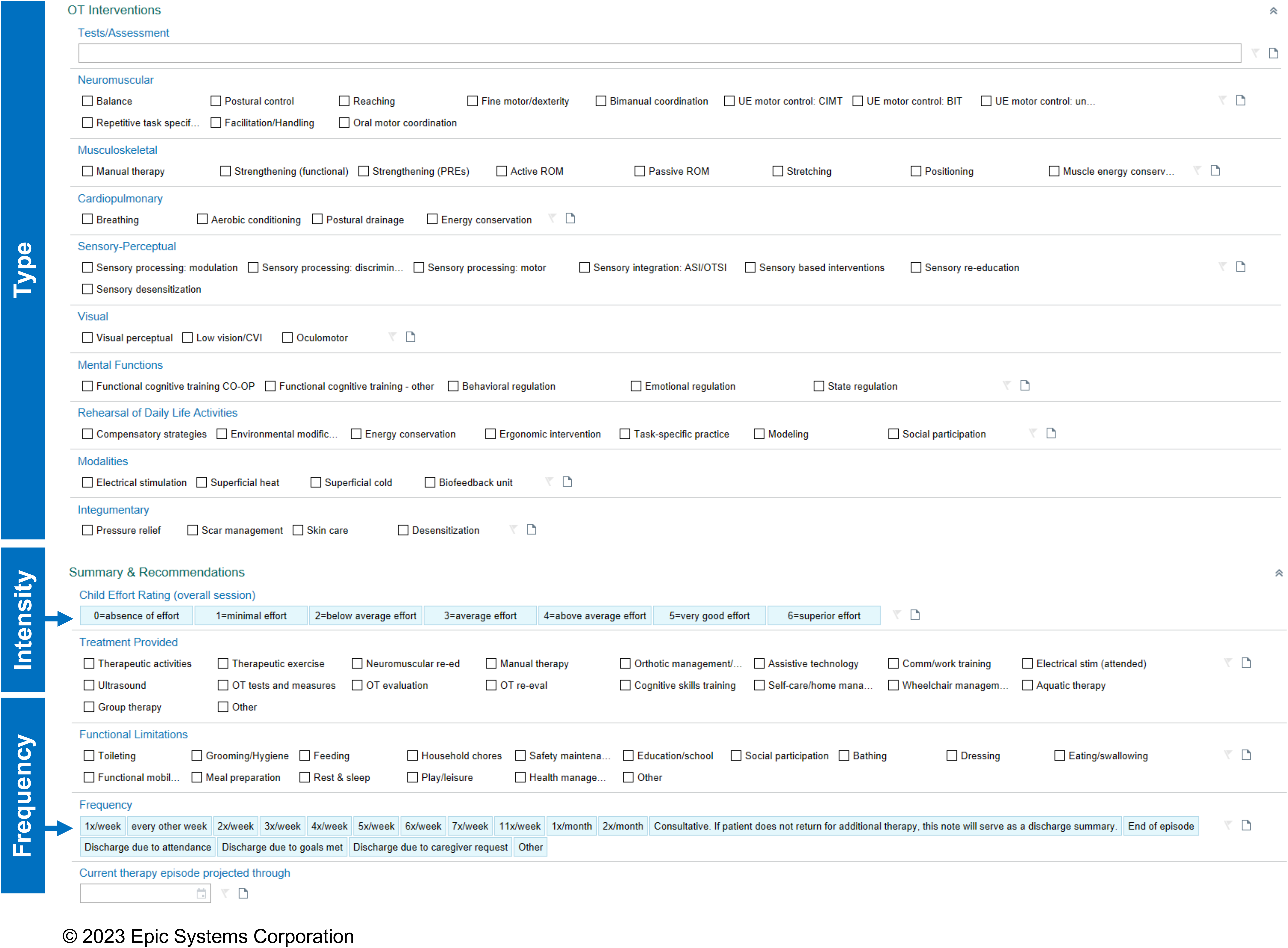
Occupational therapy FITT Epic Flowsheet dose elements (frequency, intensity, type, and time captured via billing codes).
Importantly, both institutions also had a strong culture of engagement in knowledge translation and research activities. The spread institution had eight sites delivering developmental outpatient occupational and physical therapy services. At the time that the implementation process started, there were 47 occupational therapy practitioners and 37 physical therapists in the outpatient developmental staff, including those in formal leadership positions and those working on a contingent basis.
Interventions
Interventions for the spread institution were adapted from those at the original institution (Bailes et al., 2019). Spread interventions are outlined in Figure 2, using the framework developed by Langley et al. (2009). Both institutions used the same EHR; therefore, some of the initial interventions described at the original institution (such as development of the FITT Epic Flowsheet) were not necessary at the spread institution. We made some minor changes to the FITT Epic Flowsheet to accommodate the needs of the spread institution. For example, time spent in each focus area was captured differently, and lists of equipment were changed to match the pieces available at the spread institution. The spread institution modified the FITT Epic Flowsheet training manuals (for occupational and physical therapy) from the original institution to reflect these changes. Key interventions included communication of awareness, identification of early adopters, knowledge transfer and application, feedback loops, and maintaining the gain (see Figure 2).
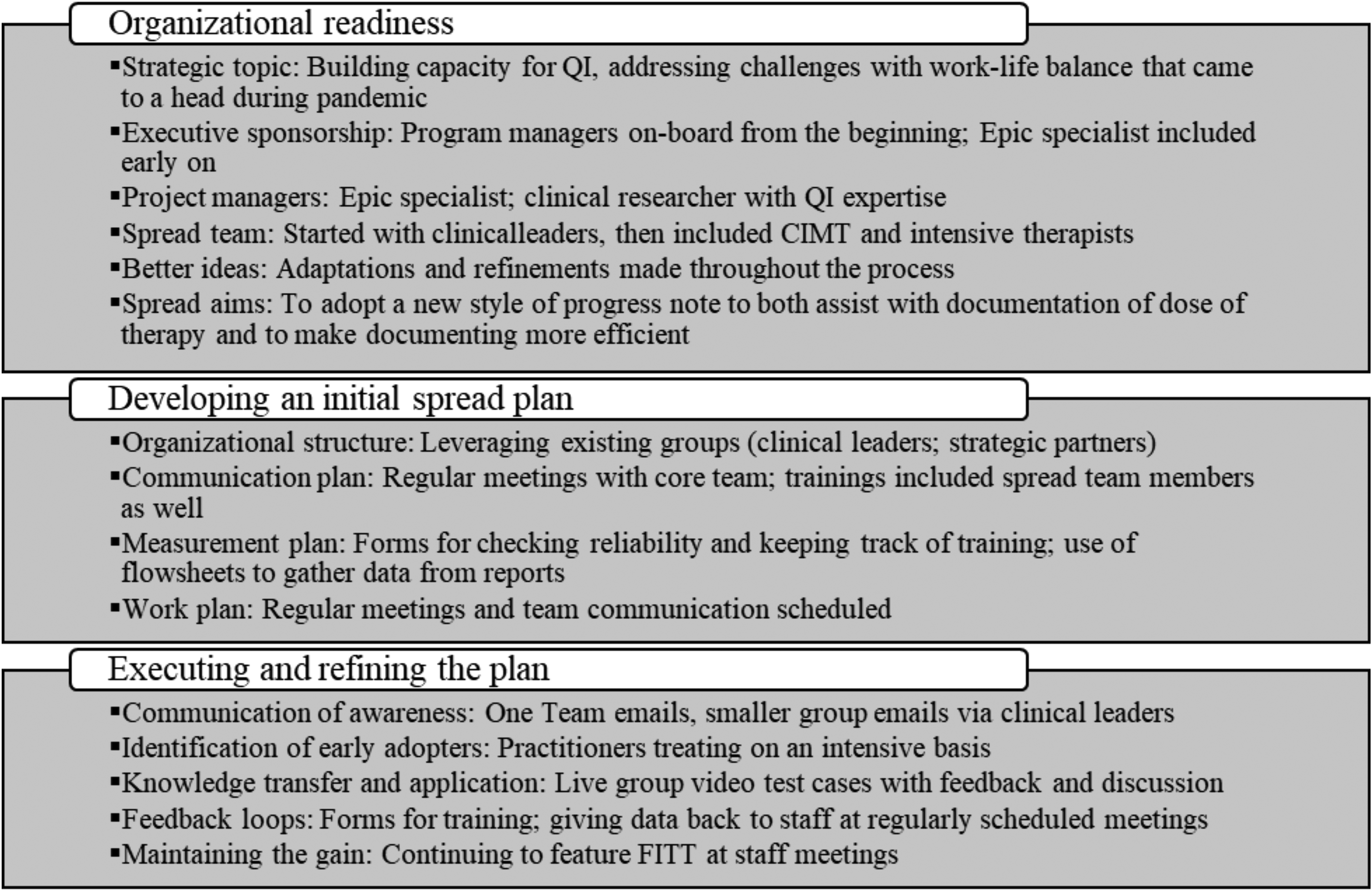
Spread framework for FITT implementation project.
Communication of Awareness
The FITT Epic Flowsheet concept was first introduced to those on the operational leadership team (i.e., program managers and clinical leaders). As the core team made changes to the initial EHR build and committed to adopting this style of documentation, additional staff members were made aware through small cycles of change. The evidence-based practice team, consisting of two evidence-based practice coordinators, was also included early in the process to ensure that the FITT Epic Flowsheet would meet their needs.
Identification of Early Adopters
Once the operational and evidence-based practice teams were able to provide feedback on the initial EHR build, we selected early adopters from the staff to trial the FITT Epic Flowsheet. This group consisted of the constraint-induced movement team (occupational therapy) and the intensive treatment team (physical therapy). We selected those teams because of the high burden of documentation for their programs and a desire among those staff members for a more streamlined documentation style.
Knowledge Transfer and Application
All staff were educated on use of the FITT Epic Flowsheet via interactive virtual presentations, including observation and group scoring of example videos. Once the FITT Epic Flowsheet went live in the EHR, all staff members were able to start using this style of documentation for all patients but were not required to do so. We provided the staff with a list of commonly used definitions from the FITT Epic Flowsheet manuals to post at their desks for easy access.
Feedback Loops
We offered additional education sessions to gain feedback from staff. In addition, we made changes in an iterative manner based on this feedback.
Maintaining the Gain
As with the original institution, the spread institution continued to engage in group review of case study videos and scoring of the FITT Epic Flowsheet at regularly scheduled staff meetings. Staff were continually redirected to the FITT Epic Flowsheet manuals to continue to work toward consistency of application.
Study of the Interventions
We used a time-series design to measure the implementation of the FITT Epic Flowsheet at the spread institution. This approach allowed us to determine whether the observed outcome was due to the intervention and to measure progress toward the aim over time.
Measures
Process Measure
The process measure for this project was the percentage of available staff trained and using the FITT Epic Flowsheet over time. We selected this as the process measure because it captured clinician experience of the intervention. The goal was to formally train 80% of regular staff in FITT Epic Flowsheet documentation.
Outcome Measure
The outcome measure was uptake of FITT Epic Flowsheet for progress notes over time. The goal of 80% adoption was selected to mirror that of the original institution.
Balancing Measure
For the balancing measure, we wanted to ensure that it was a measure that did not change as a result of the intervention. The balancing measure in this case was notes closed by 7 p.m. on the same day as the encounter. We selected this to ensure that FITT Epic Flowsheet implementation did not adversely affect clinician efficiency with documentation. In addition, this was a standing quality metric that was monitored monthly.
Analysis
Process Measure
The process measure of percentage of available staff trained and using the FITT Epic Flowsheet over time was collected using archived results of online survey agreement checks to track first attendance at training. This measure did not capture those trained early in the process (e.g., clinical leaders) who gave valuable input before the FITT Epic Flowsheet was available for clinical documentation. In addition, this measure was limited by the fact that it did not capture those who completed informal training because they missed the formal training opportunities as a result of schedule conflicts. These data were displayed using a statistical process control chart.
Outcome Measure
The outcome measure of FITT Epic Flowsheet uptake over time was defined as the percentage of FITT-eligible notes per month that were documented using the FITT Epic Flowsheet per a departmental report, which was a recurring report published monthly with back data pulled to capture the baseline and early implementation phases. The numerator was total monthly FITT Epic Flowsheets; the denominator was total occupational and physical therapy visits monthly that were “FITT eligible” (i.e., treatment only). The outcome measure was analyzed via a statistical process control chart.
Balancing Measure
The balancing measure of notes closed the same day as the encounter was collected using a data report. We divided the number of charts closed by 7 p.m. on the same calendar day as the encounter by the total number of encounters included to give a percentage for each month. For this measure, we included all encounters regardless of the type of documentation used. The average percentage of charts closed before 7 p.m. was collected for three time periods: before implementation (July 1, 2020–July 31, 2021), during implementation (August 1, 2021–June 30, 2022), and after implementation (July 1, 2022–December 31, 2022).
Results
Process Measure
Occupational and physical therapy staff members were trained in phases starting in August 2021 and ending in July 2022 (Figure 3). A total of 57 staff members attended formal FITT Epic Flowsheet trainings, representing 68% of available staff members at the final time point. Staff who were not able to attend a formal training because of scheduling conflicts or because they were on extended leave reviewed the educational slides and met individually with an early adopter or member of the leadership team to establish competency.
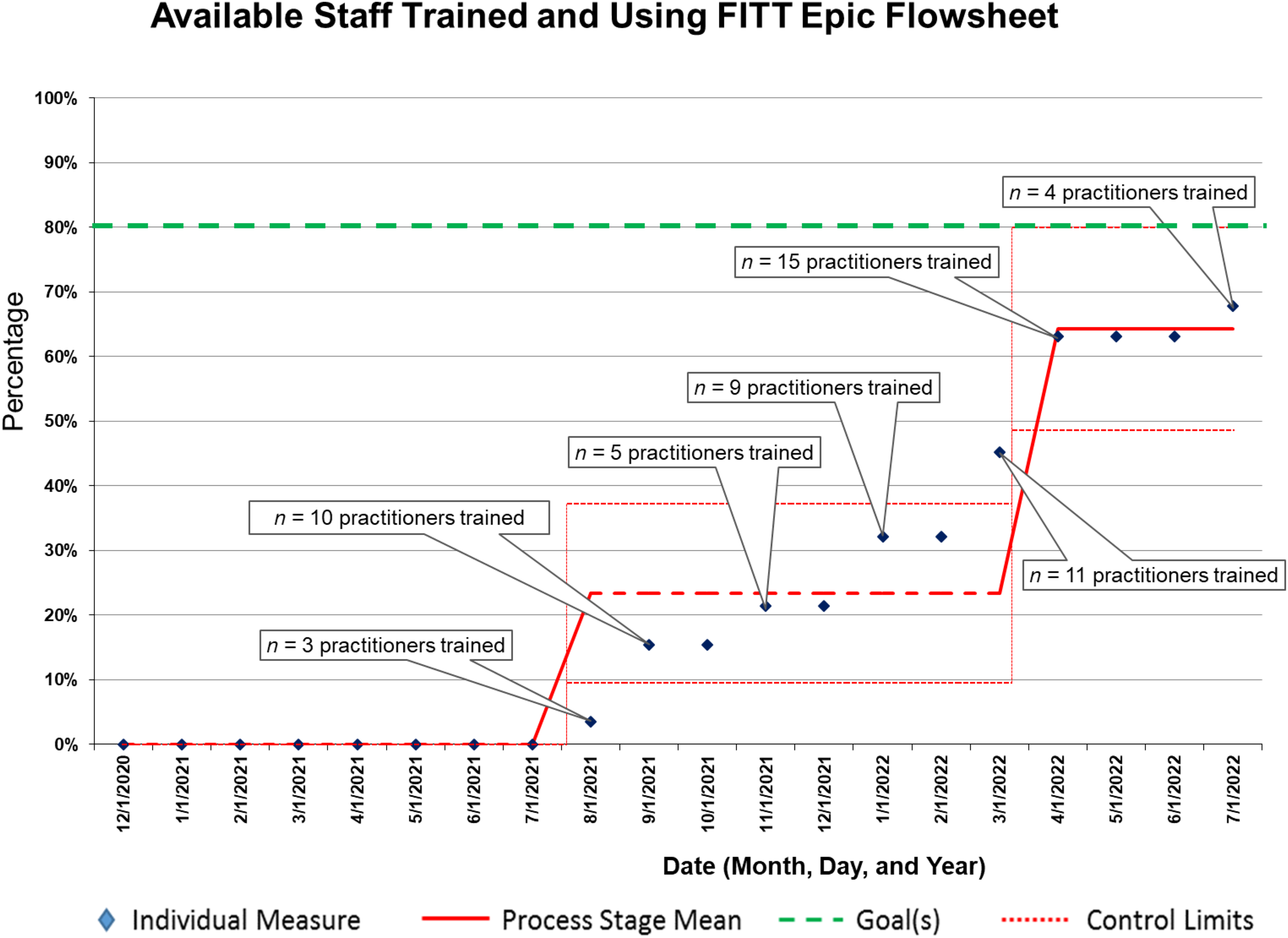
Percentage of occupational and physical therapy staff formally trained and using FITT Epic Flowsheet over time (process measure).
Outcome Measure
The statistical process control chart for the percentage of occupational and physical therapy encounters with a FITT Epic Flowsheet showed two center-line shifts across the duration of the implementation period (Figure 4). At baseline, 0% of progress notes were written using FITT Epic Flowsheet. The center line shifted to 47% in October 2021, 2 mo after training began. In July 2022, when the final training was conducted, the center line shifted to 90%, which exceeded the goal of 80% for this measure, and was maintained within the control limits for 6 mo.
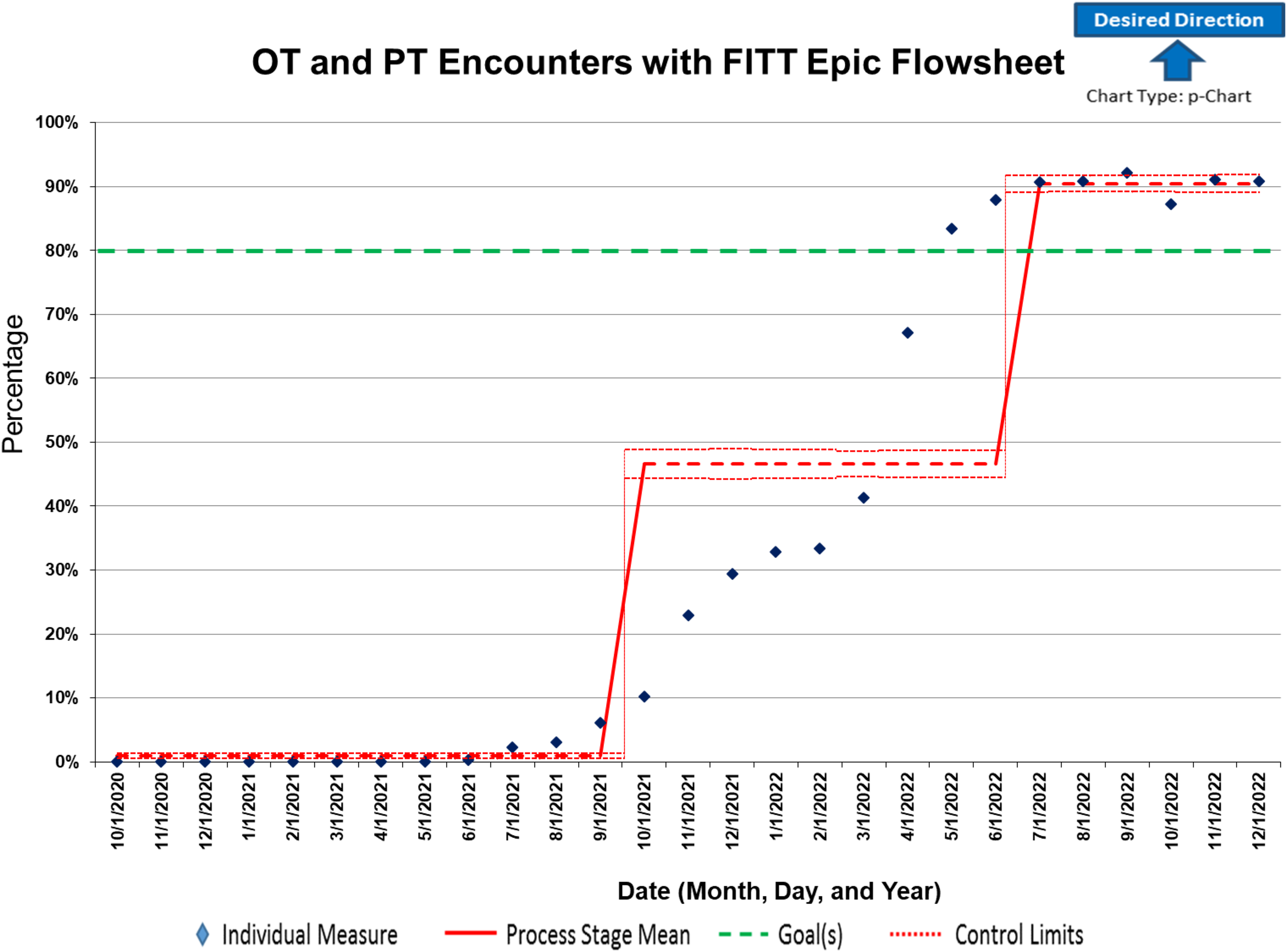
Percentage of visits documented using FITT Epic Flowsheet over time.
Balancing Measure
Data on the percentage of charts closed before 7 p.m. on the same day as the encounter showed that there was either no difference or a slight increase for this metric after implementation of the FITT Epic Flowsheet. The average percentage of charts closed on the same day before implementation was 68.5%, the average during implementation was 69.9%, and the average after implementation was 71.3%.
Discussion
Summary
The key findings of this study were that documentation using discrete data elements of pediatric occupational and physical therapy dose spread through education and that implementation in the EHR resulted in an average of 90% of eligible notes written using this style of documentation. Percentage of notes closed on the same day before 7 p.m. seemed to have stayed the same or increased slightly. The strengths of this project included the use of quality improvement methods to spread documentation changes and the resulting strong partnership between the two pediatric institutions going forward to collaborate on quality improvement and research projects.
Interpretation
The statistical process control chart seemed to show that changes to the system for the outcome measure of interest met and exceeded the original goal. This is notable because at no time in the implementation process were clinicians required to use the FITT Epic Flowsheet to document their encounters. This finding was similar to that of the original institution (Bailes et al., 2019) where uptake was also high. This project affected both people and systems. The EHR system at the spread institution was able to support its FITT Epic Flowsheet implementation, with modifications made to meet its needs. Staff could transition to use of the FITT Epic Flowsheet with support from a team of operational and project leaders. Existing systems were leveraged to maximize the impact of the interventions, consistent with the spread framework used in this study.
The anticipated outcomes were observed likely because of the context in which the documentation was spread. As mentioned earlier, both the original institution and the spread institution have a high level of support for knowledge translation and systems change.
Initial concerns raised by clinicians during the course of implementation included a potential loss of detail in the documentation of sessions, a potential increased burden of communication on therapists when sharing a patient, and a potential tradeoff of losing the SOAP (subjective, objective, assessment, plan) note format on which many clinicians were trained. Despite these concerns, however, we observed high uptake when clinicians were given a choice to use the FITT Epic Flowsheet, likely because they were able to problem-solve how to make the documentation change work for them. Some late adopters reported having reservations even after the FITT Epic Flowsheet was implemented, and staff training continued to be refined to maximize uptake. This feedback may be seen in parallel with research on the Activity Measure for Post-Acute Care (AM-PAC) “6 Clicks” tool, which had been successfully implemented in practice, and previous studies have used the data to explore the tool’s utility for predicting discharge (Jette et al., 2014; Whitlock et al., 2022). AM-PAC 6 Clicks can also be used to quantify the value of therapy services delivered in inpatient setting (Hull & Thut, 2018). However, the utility of a tool such as the AM-PAC for these purposes relies on individual clinicians’ uptake of the tool. A qualitative study of physical and occupational therapists’ experience implementing the AM-PAC 6 Clicks found that they considered multiple factors when deciding whether to use a tool; they were less likely to use a tool if they were not confident in their own reliability when assigning scores or felt the tool simplified their clinical reasoning too much (Dewhirst et al., 2016). Similar feedback was observed initially with the present project, but as uptake of the FITT Epic Flowsheet increased, clinicians began to use the tool for more patients and to informally spread the notes to each other.
Some additional costs and strategic trade-offs were observed with the spread of the FITT Epic Flowsheet. Specifically, not only a lack of change, but an increase in the balancing measure demonstrating more efficient documentation by clinicians would have been ideal. Previous work has shown that the EHR can be leveraged to help implement standardized protocols to improve care, such as by helping to prevent central line–associated bloodstream infections (Thate et al., 2020) or reducing spine surgery infections (Ryan et al., 2014). However, medical team members spend a significant portion of their day documenting care in the EHR, with many notes never being viewed by another professional (Hripcsak et al., 2011). For EHR documentation to be highly valued by health professionals, it needs to maximize efficiency by meeting multiple needs while also fitting into the existing workflow (Ho et al., 2014). As demonstrated in the primary outcome measure of this study, the FITT Epic Flowsheet had a high level of uptake despite there being no change in the selected measure of efficiency of documentation (i.e., notes closed on the same day as the encounter). It is possible that this balancing measure was not sensitive to the amount of time saved by clinicians, or that the time spent documenting was similar for clinicians, but they found other aspects of the FITT Epic Flowsheet to be more valuable than a traditional progress note. For example, the FITT Epic Flowsheet was intentionally implemented alongside point-of-care documentation (i.e., practitioner bringing their laptop computer into the treatment room and documenting during the session) in the original institution. While point-of-care documentation was not explicitly implemented at the spread institution, clinicians reported anecdotally that the FITT Epic Flowsheet made it easier for them to document care during a session. Thus, the ability to more easily engage in point-of-care documentation may have also increased uptake of the FITT Epic Flowsheet at the spread institution.
Limitations
The ability to extrapolate results of this study was limited because both the original institution and the spread institution had many similarities, including using the same EHR system, being of similar size and organizational structure, and having many of the same support positions available to facilitate this work. Organizations with different structures, cultures, sizes, and EHR usage may not have the same results observed in this study. One factor that might have affected the outcome measure could have been unintended spread of the FITT Epic Flowsheet to staff who had not yet completed formal training. We minimized this by ensuring that all staff had access to the manual and training materials and ensuring participation in ongoing group scoring activities. Conversely, unintended spread (i.e., spread of the FITT Epic Flowsheet prior to completion of staff training) also may be considered a strength in this case, because it demonstrates that staff members wanted to start using the FITT Epic Flowsheet as soon as possible. Inaccurate documentation of interventions may also be a limitation.
Implications for Occupational Therapy Practice
Occupational therapy practitioners, administrators, and leaders should consider implementing clinical documentation that can be shared and agreed upon between institutions (such as the FITT Epic Flowsheet) so that researchers can combine data to study how dose of therapy affects outcomes and improves practice. Although significant effort may be required to change a documentation process, the return on investment for both individual institutions and the profession can be quite high. Using systems of documentation that include shared data elements will allow the profession to leverage clinical data collected during usual care for research and quality improvement purposes. Ultimately, this will help demonstrate the distinct value of the services that practitioners provide.
Conclusion
Discrete documentation of pediatric occupational and physical therapy dose can be spread from one institution to another if both institutions share some characteristics, including an EHR system. Clinicians and researchers should consider sharing documentation strategies between organizations to maximize the opportunity to share data.