
Abstract
The study results highlight the importance of considering the nutritive sucking ability of infants who were born preterm when evaluating their potential to achieve independent oral feedings.
Approximately 8% of Canadian pregnancies result in preterm birth, defined as a birth before 37 wk of gestation (StatsCan, 2016). Roughly one-half of all premature infants are admitted to a Level 2 or Level 3 neonatal intensive care unit (NICU) for medical care (Lui et al., 2019). Up to 40% of premature infants necessitating neonatal intensive care may experience oral (breast or bottle) feeding difficulties during their hospital stay (Jadcherla et al., 2010, 2017). The most common oral feeding difficulties encountered include disorganized sucking pattern, uncoordinated sucking, swallowing and breathing processes leading to episodes of apnea, as well as bradycardia and oxygen desaturations and fatigue (Viswanathan & Jadcherla, 2020).
Infants with such oral feeding difficulties often experience a prolonged transition from full tube to independent oral feeds, lengthy hospitalization (because attainment of independent oral feeds is a criteria for hospital discharge), and long-term feeding issues into childhood—all of which are associated with increased caregiver stress (Kwon et al., 2020; Sanchez et al., 2018; Silverman et al., 2021; Viswanathan & Jadcherla, 2020). It is therefore important for premature infants who are in the NICU to achieve the critical milestone of independent oral feeding for adequate growth and development (Pineda, 2016; Viswanathan & Jadcherla, 2020).
Independent oral feeding is a complex, multisystem process that requires coordination of suck–swallow– breathe (SSB) functions (Lau, 2016). Specifically, SSB is a highly coordinated process that infants use to extract milk from the breast or bottle, form a bolus by peristaltic movements of the tongue, and propel the bolus from the oral to pharyngeal area to trigger the swallow reflex, which projects the bolus into the digestive tract while maintaining respiration (Lau, 2016; Mizuno & Ueda, 2003). The coordination of this complex process is required for safe, independent oral feeding (Lau, 2016). Typically, full-term infants (>37 wk gestational age) have established this coordinated action, enabling them to reach safe independent oral feeds (Lau, 2016). However, for infants who are born premature, the maturation of SSB occurs between 32 and 34 wk gestation; thus, they receive tube feedings until they are deemed ready to initiate oral feeds by the neonatal team (Lau, 2016; Viswanathan & Jadcherla, 2020).
Previous studies have demonstrated that oral feeding performance is related to the maturation of the SSB mechanism (Amaizu et al., 2008; Lau, 2016; Lau & Smith, 2012; Mizuno & Ueda, 2003). These studies focused on various SSB parameters and their relationship to oral feeding performance (Amaizu et al., 2008; Lau, 2016; Lau & Smith, 2012; Mizuno & Ueda, 2003). Mizuno and Ueda’s (2003) study demonstrated that bolus size improves because suction amplitude is increased (millimeters of mercury, suck strength) over time. They noted that the transition to oral feeds was mediated by increased suck strength and increased coordination within SSB. Moreover, underdeveloped oral skills can also defer the transition to oral feeds (Mizuno & Ueda, 2003). In another study, Amaizu et al. (2008) observed that rate of milk transfer (milliliters per second) increases because of a rise in sucking and swallowing frequency that occurs early on in the transition from full tube to full oral feeds (also see Lau, 2016; Lau & Smith, 2012).
Hence, oral feeding performance increases as sucking skills mature, identifying a possible link between attainment of independent oral feeds and nutritive sucking (Amaizu et al., 2008; Lau, 2016; Lau & Smith, 2012; Mizuno & Ueda, 2003). Despite the research pertaining to SSB, a gap remains in the ability to identify infants who may have difficulty attaining independent oral feeds using nutritive sucking measures. In response to this issue, the objective of this study was to identify nutritive sucking measures associated with the length of time to attain independent oral feeds in preterm infants. Given that nutritive sucking is a fundamental skill needed for adequate oral feeding performances among infants, we hypothesized that specific nutritive suck measures—including average suck strength, average suck burst duration, average suck count, and average pause duration—would be associated with time to independent oral feeds (days).
Method
Study Design
An observational cohort pilot study was performed to determine specific nutritive sucking measures that may be associated with independent oral feeds. This study was approved by Queen’s University Health Sciences research ethics board and the human research ethics board of affiliate hospitals.
Participants and Setting
A total of 14 infants (7 male and 7 female) from the NICU at Kingston Health Sciences Centre (KHSC) were enrolled from 2019 to 2020 (prepandemic). The NICU at KHSC is a Level 2 to Level 3 unit with a maximum capacity of 24 beds. In this unit, a cue-based feeding approach is used to initiate and advance oral feeds; it is managed by the neonatal team consisting of a neonatologist, nurse, dietician, and an occupational therapy practitioner. Infants with the following inclusion criteria were enrolled: (1) born at ≤34 wk gestational age as determined by obstetric ultrasonogram and clinical examination, (2) were of appropriate size for their gestational age, and (3) were receiving only tube feeds (orogastric or nasogastric). Exclusion criteria were infants with (1) bronchopulmonary dysplasia, (2) necrotizing enterocolitis, (3) intraventricular hemorrhage Grades 3 and 4, (4) periventricular leukomalacia, (5) genetic and metabolic syndromes, and (6) congenital anomalies.
Procedure
A research assistant reviewed the participant’s medical charts to ensure that they met the qualifications for the study and obtained informed written consent from the participants’ parents before entry into the study. For this study, oral feeding management was left to the neonatal team, who was blinded to the objective of the study to minimize biases. A nipple monitoring device was used to record nutritive sucking measures (Fucile & Dow, 2023). This system uses standard nipples to monitor nutritive sucking skills. For this study, only standard yellow nipples were used for consistency in milk flow rates across participants. The intraoral pressure generated (suction amplitude) during sucking was monitored via a small tube inserted to the tip of the nipple and connected to a pressure transducer. The transducer was connected to a Biopac MP 100 WSP system (Biopac Systems, Inc.; Laval, Quebec, Canada) that was linked to a laptop computer. Nutritive sucking measures were monitored directly on the computer screen, and data were stored for later analyses with the Acqknowledge software program. Further details on this device can be found in Fucile and Dow’s (2023) study.
Nutritive sucking measures were monitored once when infants were receiving an average of three to four oral feeds per day. This time period was selected because we observed in our previous study that it was a pivotal period where infants often present with oral feeding difficulties and struggle through the transition from complete tube to independent oral feeds. Nutritive sucking outcomes were measured in the first 5 min of the feed to ensure that the infant’s true potential sucking skills were recorded and not affected by fatigue. For this study, breastfeeds were not recorded because maternal factors such as milk supply or speed of flow from the breast may affect the infant’s sucking skills. Parents were invited to feed their infant at the bedside. If parents were not available, the assigned nurse performed the oral feeding. Parents or nurses were encouraged to feed their infant in their customary manner but with no chin cheek support or pacing because both interventions may influence milk flow. A trained research assistant performed the recorded oral feedings and reported on oral feeding performance, adverse events, behavioral state, and any interruptions during the oral feed.
Outcome Measures
The infant baseline characteristics monitored included birth weight (grams), gestational age (weeks), sex, firstborn, twin, Apgar scores at 1 and 5 min, as well as number of days receiving endotracheal tube (ETT) and nasal continuous positive airway pressure (NCPAP) respiratory support (Dodrill et al., 2008; Fucile et al., 2022; Jadcherla et al., 2010). These infant baseline characteristics were abstracted from the medical chart.
The nutritive sucking measures monitored included suck strength (suction amplitude, millimeters of mercury), average suck burst duration (seconds), suck count (average number of sucks), and average pause duration (seconds). These nutritive sucking measures were extracted from the nutritive sucking record. Specifically, sucking strength was measured through a pressure transducer inserted through the nipple and is expressed as suction amplitude generated. Additionally, suck burst duration was the length of time that the infant could sustain a suck before pausing. Suck count measures the number of sucks performed within a burst, and the average pause duration measures the length of time that the infant must pause.
The clinical measure outcome, attainment to independent oral feeds, was defined as the number of days needed to transition from full tube feed to full oral feeds. This outcome was abstracted from the medical charts.
Data Analysis
We reported participants’ baseline characteristics using descriptive statistics: M (SD) and frequencies (%). Simple univariate linear regression was first performed to assess baseline characteristics (gestational age, number days on ETT and NCPAP respiratory support) and nutritive sucking outcome measures (average suck burst duration, average suck count, average pause duration, and average suction amplitude) for significance with attainment to independent oral feeds. A multivariate regression was then performed with the significant nutritive sucking measures and baseline characteristics as a confounding variable to assess their relation to the number of days to attain independent oral feeds. We performed data analysis using IBM SPSS Statistics (Version 28.0.1.1). Significance was defined as a p value of .05 or lower. Sample size was derived from convenience sampling because this investigative pilot study was attempting to establish potential associations between nutritive sucking measures and attainment to independent oral feeds.
Results
All 14 infants completed the study. Table 1 illustrates that participants had a mean birth weight of 2,096 g (SD = 568), a mean gestational age of 33 wk (SD = 2), and an even distribution of sex. Overall, participants took an average of 11 days (SD = 6) to attain independent oral feeds, and they were on average 35.7 wk corrected gestational age (SD = 1.25) at the time of the oral feeding recording. The univariate regression analysis revealed that average suck count, average suck burst duration, gestational age, as well as number of days on ETT and NCPAP emerged as variables associated with days until independent oral feeds (Table 2; for all tests, p < .001). We then performed the multivariate regression using the identified significant predictors (average suck count and average suck burst duration) and gestational age as the confounding variable. Gestational age was only included in the model because of the collinearity between gestational age and respiratory support. Table 3 depicts that average suck burst duration (p = .04) and gestational age (p = .03) were inversely associated with number of days to attain independent oral feeds. Figure 1 illustrates the inverse relation between average sucking burst duration and days to attain independent oral feeds.
Note. ETT = endotracheal tube; NCPAP = nasal continuous positive airway pressure.
Univariate Analysis
Note. Boldface indicates significance at p < .05. ETT = endotracheal tube; NCPAP = nasal continuous positive airway pressure.
Multivariate Analysis
Note. The dependent variable is the number of days until full oral feeds. Boldface indicates significant at p < .05.
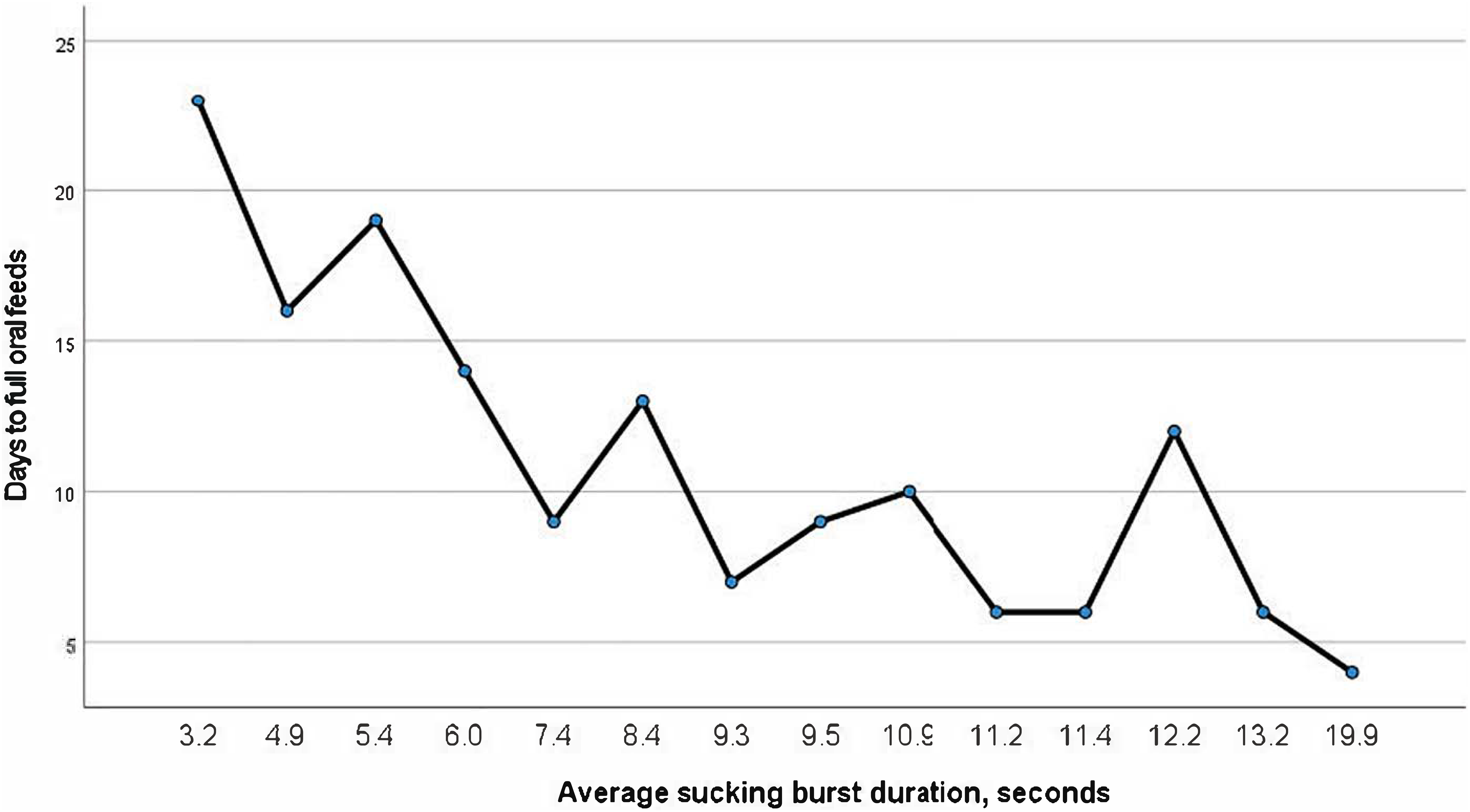
Association between average sucking burst duration (seconds) and days to full oral feeds.
Discussion
Independent oral feeding is a main requirement for the discharge of infants from the NICU. Because of immaturity of oral structures, premature infants are at a high risk of presenting with a disorganized sucking pattern and an inefficient or weak suck, all of which affect the SSB mechanism (Lau, 2016). Literature on feeding among premature infants reveals a gap in knowledge surrounding the relationship between nutritive sucking measures and achievement of independent oral feeds. Therefore, in this study, we aimed at identifying a relationship between days until the achievement of independent oral feeds and nutritive sucking measures.
In this preliminary study, we found an inverse relationship between average suck burst duration and days until independent oral feeds, such that increased duration in suck burst was associated with a decrease in number of days to attain independent oral feeds. This result suggests that the longer a premature infant can sustain a suck, the faster they will reach independent oral feeds. These results are supported by similar research that confirmed that infants become more efficient in their feeding through the extension of their suck burst (Sakalidis & Geddes, 2016). A suck burst is defined as 1 or more sucks with less than 2 s in between each suck (Pickler & Reyna, 2004), and longer sucking bursts allow infants to uptake higher volumes of milk before necessitating a pause to swallow and breathe (Sakalidis & Geddes, 2016).
A stronger ability to suck for a longer duration will allow an infant to consume higher volumes of milk, increasing feeding efficiency. Thus, a longer suck burst will increase an infant’s performance during feeding. Moreover, the results also suggest that gestational age is associated with number of days to attain independent oral feeds. This finding is supportive of previous studies that have shown that full-term infants can sustain a longer suck compared with preterm infants, and preterm infants experience partial ventilation recovery with more difficulty maintaining respiratory function because of an immature cardiorespiratory system (Amaizu et al., 2008; Mizuno et al., 2004; Mizuno & Ueda, 2003).
The clinical utility of these findings can enable feeding specialists to better understand the relationship between nutritive sucking skill and attainment to independent oral feeds. The literature suggests that suck burst duration matures with age, thus improving oral feeds (Amaizu et al., 2008; Gewolb & Vice, 2006; Sakalidis & Geddes, 2016). We have identified a more direct relationship between an infant’s ability to successfully feed and independent oral feeds. Therefore, feeding assessments should be inclusive of an infant’s ability to maintain a suck during a feed. An important clinical implication of this study reveals that clinicians may use suck burst duration, which may be done empirically, to estimate time to independent oral feeding. Suck burst duration is a variable that may be measured without the use of additional machinery or specialized training. Thus, in feeding intervention studies, researchers should consider targeting improvements in the infant’s ability to sustain a suck, because an increased suck burst duration is indicative of positive feeding outcomes.
Limitations
Limitations to this pilot study should be considered. The participants included were all clinically stable, consisting of premature infants, and the sample size of participants was small, which limits the clinical generalizability. Further research needs to include a larger and broader sample population to incorporate infants with diverse medical conditions to confirm these preliminary findings and increase the generalizability of the results to a wider population. Further research should also focus on identifying clinical thresholds of sucking burst duration associated with achievement to independent oral feeds. Such thresholds can then be used in clinical practice to identify premature infants at risk of encountering oral feeding difficulties.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
▪ Sucking burst duration is inversely related to achievement of independent oral feeds. ▪ Sucking burst can be used by practitioners as an indicator of oral feeding performance. ▪ Nutritive sucking ability should be considered when evaluating infant’s potential to achieve independent oral feedings.
Conclusion
Attainment to independent oral feeds is a major challenge for premature infants. This study has shown that a suck burst duration during the first 5 min of oral feed is inversely associated with the length of time to achieve independent oral feeding. Sucking burst duration has the potential to become an important clinical indicator because it can be measured through a nipple monitoring device or through empirical observation by clinicians. The results highlight the importance of considering an infant’s nutritive sucking ability when evaluating their potential to achieve independent oral feeds.
Footnotes
Acknowledgments
This study was funded by the University Hospital Kingston Foundation Innovation Fund (Grant 70613). We thank the nurses in the neonatal intensive care unit at the Kingston Health Sciences Centre for their support.