
Abstract
This is the first study to examine disparities in access to inpatient psychiatric occupational therapy in the Veterans Health Administration.
The Veterans Health Administration (VHA) has embraced a recovery-oriented approach to inpatient psychiatric care, shifting the focus of intervention from symptom reduction to empowering veterans to fully participate in society (Substance Abuse and Mental Health Services Administration [SAMHSA], 2012; VHA, 2023). Fundamental to achieving such recovery is the independent completion of life activities, including activities of daily living (ADLs), or self-care tasks such as bathing and dressing (American Occupational Therapy Association, 2020; SAMHSA, 2012). Occupational therapy practitioners are mental health providers who are squarely focused on facilitating the independent completion of daily activities and are, therefore, uniquely equipped to contribute to this aspect of recovery-oriented care by promoting independence in performing ADLs and other life activities (e.g., leisure activities; Burson et al., 2017; Synovec, 2015). Indeed, occupational therapy services have been shown to improve performance of ADLs and other activities among those with psychiatric conditions (D’Amico et al., 2018; Lipskaya-Velikovsky et al., 2016, 2020). As such, it is crucial that veterans receive equitable access to inpatient psychiatric occupational therapy services in the VHA.
Little is known regarding whether occupational therapy services are provided equitably within VHA inpatient psychiatric settings. Equitable care access occurs when patient need (e.g., ADL limitations) dictates health care delivery (e.g., occupational therapy services). Disparities in access occur when patient-level (e.g., sociodemographic characteristics) or organization-level (e.g., facility staffing) factors unrelated to clinical need drive access (Anderson et al., 2014). Research in other settings and populations indicates a tendency for people who are in need of occupational therapy to receive such care, yet evidence of access disparities exists (Kinney et al., 2022, 2023). For example, people from minoritized racial and ethnic groups who are hospitalized for medical conditions are less likely to receive occupational therapy relative to White, non-Hispanic people, even while accounting for the performance of ADLs, a direct indicator of need for occupational therapy (Kinney et al., 2022). Furthermore, in a study of veterans with traumatic brain injury (TBI), the relationship between activity limitations and occupational therapy utilization was weaker among those who accessed care at facilities with lower complexity (e.g., facilities with fewer clinical specialties), suggesting that VHA settings with fewer resources were less responsive to veterans’ needs related to occupational therapy (Kinney et al., 2023). There is a need to understand whether similar disparities in access to occupational therapy services exist within VHA inpatient psychiatric settings.
The present study is the initial phase of an explanatory-sequential mixed-methods design. Specifically, we investigate potential disparities in access to inpatient psychiatric occupational therapy using quantitative methods, which we follow with an in-depth qualitative exploration of mechanisms underlying observed findings that will be reported separately (Creswell & Plano Clark, 2018). Here, we sought to investigate whether a direct measure of need for occupational therapy, ADL limitations, was associated with inpatient psychiatric occupational therapy utilization in the VHA. Although we recognize the breadth of potential targets of occupational therapy intervention in the inpatient psychiatric setting (e.g., social participation), we focused on ADL limitations because it is the only direct indicator of need for occupational therapy that is routinely collected in the inpatient psychiatric setting. Additionally, we examined whether patient-level (e.g., sociodemographic factors) and facility-level (e.g., facility complexity) characteristics were associated with occupational therapy utilization while accounting for ADL limitations, indicating potential disparities in access. Last, we examined whether the relationship between ADL limitation and occupational therapy utilization differed according to facility-level characteristics.
Method
Participants and Procedures
This was a secondary analysis of administrative data for veterans who were admitted to a VHA inpatient psychiatric unit between January 1, 2015, and January 1, 2020. This study was approved by the local regulatory Veterans Affairs (VA) committee and institutional review board. Data were gathered from the Corporate Data Warehouse (CDW), which stores VHA electronic medical record data.
Inclusion criteria included ▪ admission to a VHA inpatient psychiatric unit with occupational therapy services available, ▪ documented performance of ADLs within an admission nursing assessment, and ▪ survival of hospitalization.
In the event of multiple admissions for a single veteran during the study timeframe, the first admission was used. Inpatient psychiatric units with available occupational therapy services were identified by the presence of at least one occupational therapy encounter (see operational definition provided later) in the inpatient psychiatric setting at the time of admission. Among the 134,663 veterans who met inclusion criteria, 819 (0.6%) were removed because of missing predictors, leaving 133,844 eligible for analyses. See Figure 1 for details regarding the application of inclusion criteria.
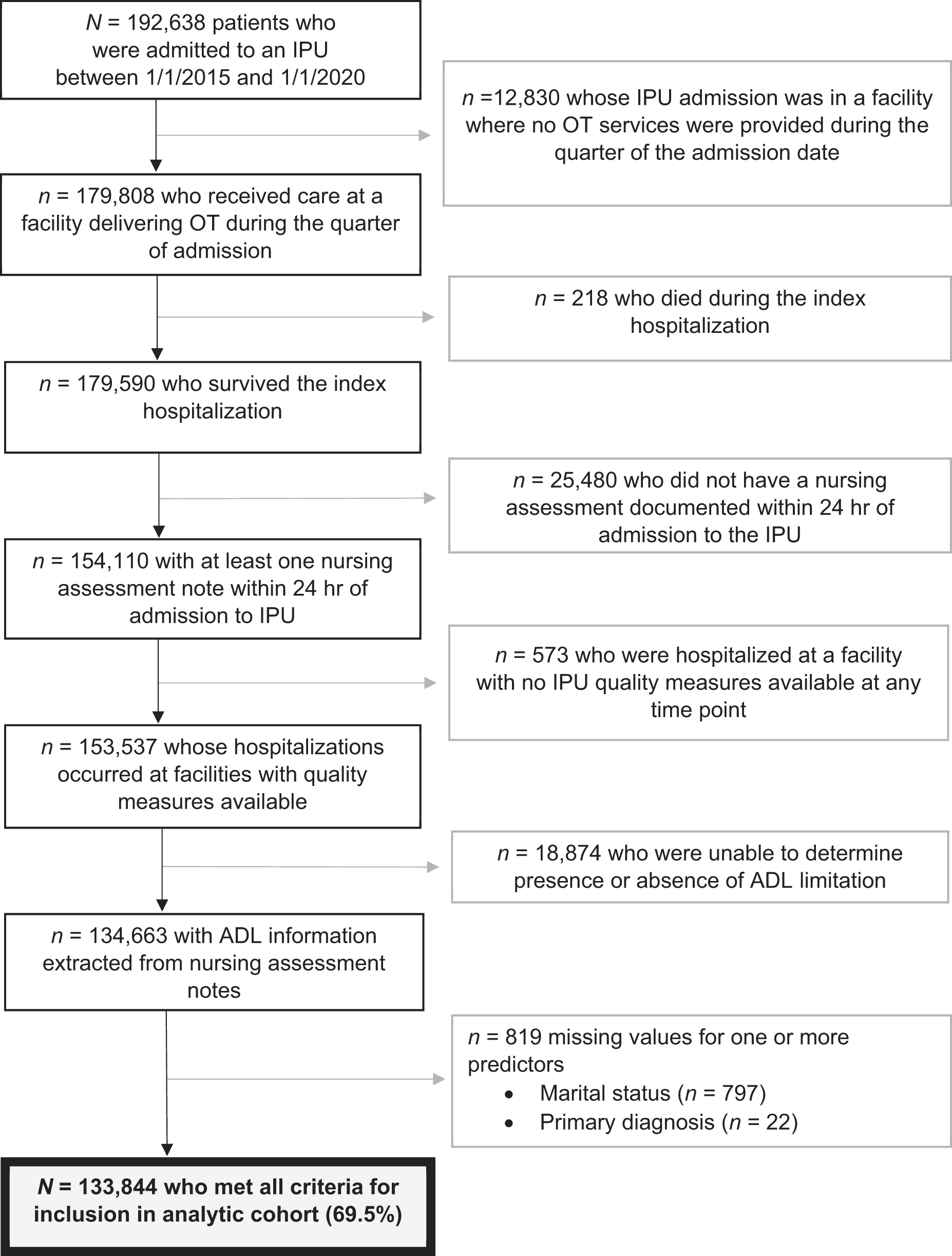
Detailed summary of the application of inclusion criteria.
Measures
Activities of Daily Living Performance Status
Inpatient psychiatric nursing assessments include an evaluation of performance of ADLs, but results are not abstracted in a structured format. Thus, we developed and validated an automated process by which ADL performance status (independent vs. limited) was extracted from such assessments. Eligible ADLs consisted of bathing or showering, dressing, personal hygiene and grooming (e.g., brushing teeth), toileting, and feeding. ADL performance status was considered limited if the veteran required physical assistance, supervision, or setup from another person to complete one or more activities.
To develop the algorithm, we first identified inpatient psychiatric nursing assessments documented within 24 hr of admission. A licensed occupational therapy practitioner (Adam R. Kinney) with clinical experience in inpatient psychiatric settings developed initial phrases that indicated assessment of ADL performance. Guided by a rule-based approach, we developed a library of regular expressions using Python 3 to classify note content as independent, limited, or unknown ADL performance (Hunt, 2019; Mande et al., 2018). Regular expressions were iteratively refined by applying the algorithm to random samples of nursing assessments, using manual chart review to identify improvements until no further refinements were identified. (For exemplar text extractions and corresponding regular expressions, see the Supplemental Appendix, available online with this article at https://research.aota.org/ajot). Additional information regarding the algorithm is available from Adam R. Kinney on request.
Validation consisted of comparing algorithm performance against blinded manual chart review. A power analysis indicated that to obtain a 95% confidence interval (CI) that rules out a sensitivity and specificity of .90, at least 362 notes reflecting positive and negative cases (≥724) were required to obtain statistical power of ≥.80. Notes were randomly sampled and evenly distributed across facilities to account for local variation in documentation practices.
Validation proceeded in two phases. First, because not all notes included an ADL performance assessment, we applied the algorithm to distinguish notes with ADL performance information from those without such information. Algorithm performance during this phase was excellent, identifying the presence of ADL performance information with a sensitivity of .90 (95% CI [0.86, 0.93]) and a specificity of .98 (95% CI [.96, .99]). In the second phase, the algorithm was applied to notes that it identified as containing ADL information, further distinguishing veterans whose ADL performance status was limited versus independent. Algorithm performance in this phase was similarly excellent, identifying ADL limitations with a sensitivity of .93 (95% CI [.90, .96]) and a specificity of .91 (95% CI [.89, .94]).
Occupational Therapy Utilization
Occupational therapy utilization (yes vs. no) was defined as at least one of the following conditions associated with inpatient psychiatric care: ▪ occupational therapy–specific Current Procedural Terminology codes (97003, 97165, 97166, 97167, 97004, and 97168) ▪ occupational therapy–specific, 500-series Decision Support System Identifier in the primary or secondary position ▪ provider information reflecting an occupational therapy practitioner.
Facility Characteristics
We obtained the following characteristics of facilities at which each veteran was admitted: facility complexity, psychiatric bed supply, and psychiatric care quality. These characteristics corresponded to facility conditions at the time of admission. Facility complexity (low, medium, high) is a composite index reflecting factors such as patient mix (e.g., clinical risk) and diversity of services provided (VHA Office of Productivity, Efficiency, and Staffing, 2020). Psychiatric bed supply was defined as the number of operational inpatient psychiatric beds at the time of admission. Tertile values for the distribution of bed supply were used to identify low, moderate, and high bed supply. Psychiatric care quality was measured using the Hospital-Based Inpatient Psychiatric Services indicator, a VHA composite measure of two rates, calculated from the proportion of veterans (1) who were screened for risk to self or others, substance use disorder, trauma, and strengths and (2) who were discharged with two or more antipsychotic drugs using appropriate justification (Joint Commission, 2016). Tertile values were used to identify low, moderate, and high care quality.
Sociodemographic Characteristics
The following sociodemographic characteristics were abstracted from the CDW for each veteran at the time of admission: age in years, sex assigned in the medical record (male vs. female), race–ethnicity (White, non-Hispanic; Black, non-Hispanic; American Indian/ Alaskan Native, non-Hispanic; Asian American, non-Hispanic; Native Hawaiian or Pacific Islander, non-Hispanic; Hispanic; and unknown), and marital status (married vs. unmarried).
Covariates
Primary diagnosis, history of TBI, comorbidity burden, and length of stay were gathered from the CDW. Primary diagnosis was defined as the diagnosis documented as the reason for admission, identified using the International Classification of Diseases, Ninth Revision (ICD–9) and International Classification of Diseases, Tenth Revision (ICD–10) codes for major depressive disorder, posttraumatic stress disorder (PTSD), alcohol use disorder, schizophrenia or schizoaffective disorder, bipolar disorder, other substance use disorder, and other disorder. History of TBI (no vs. yes) was identified by ICD–9 or ICD–10 codes indicating a TBI documented at any time before admission (Adams et al., 2022). Comorbidity burden was measured using the Charlson Comorbidity Index, calculated in the year before admission (Quan et al., 2005). Length of stay was the total number of days spent on the inpatient psychiatric unit.
Data Analysis
A descriptive analysis in the total sample and stratified by occupational therapy utilization was conducted. To examine whether ADL performance status was associated with occupational therapy utilization, we used modified Poisson regression to model occupational therapy utilization (yes vs. no) as a function of ADL performance status, facility characteristics, sociodemographic characteristics, and other covariates. Modified Poisson regression was used because it derives reliable estimates of relative risk despite the relatively frequent occurrence (>10%) of occupational therapy utilization (Zou, 2004). A clustered sandwich estimator was used to adjust estimates for the clustering of observations within VHA facilities (Zeileis et al., 2019). To investigate whether the relationship between ADL performance status and occupational therapy utilization differed across facility characteristics, we tested statistical interactions between ADL performance status and each facility characteristic separately. We visually probed statistically significant interactions, and we used R (Version 4.3.1) to conduct all analyses (R Core Team, 2023). Statistical significance was evaluated at α = .05.
Results
Most veterans were White, non-Hispanic (60%), and 88% were male. The most common reason for admission was major depressive disorder (25%). One-quarter (25%) received inpatient psychiatric occupational therapy services. Approximately 8% had a documented ADL limitation; a similar proportion was observed among those who did not receive occupational therapy services (7%), suggesting unmet need. See Table 1.
Characteristics of Veterans Receiving Inpatient Psychiatric Care (N = 133,844)
Note. Percentages are based on the column sample size. ADL = activity of daily living; OT = occupational therapy; PTSD = posttraumatic stress disorder; TBI = traumatic brain injury.
Model Explaining Occupational Therapy Utilization Without Interactions
Those with an ADL limitation were more likely to receive inpatient psychiatric occupational therapy. Veterans who received care at facilities with higher complexity (medium and high vs. low complexity) and facilities with higher inpatient psychiatric care quality (moderate and high vs. low) were more likely to receive occupational therapy. Conversely, veterans who received care at facilities with a high number of psychiatric beds (vs. low) were less likely to receive occupational therapy. Black veterans (vs. White, non-Hispanic) were less likely to receive occupational therapy services, whereas Hispanic veterans were more likely to receive occupational therapy relative to White, non-Hispanic, veterans. Other factors associated with an increased likelihood of receiving occupational therapy were older age, primary diagnosis of major depressive disorder (vs. PTSD, alcohol use disorder, other substance use disorder, and other disorder), history of TBI, greater comorbidity burden, and longer length of stay. See Table 2.
Parameter Estimates for Model Explaining OT Utilization Without Statistical Interactions (N = 133,844)
Note. ADL = activity of daily living; CI = confidence interval; OT = occupational therapy; PTSD = posttraumatic stress disorder; RR = risk ratio; TBI = traumatic brain injury.
Models Including Interactions Between Activities of Daily Living Performance Status and Facility Characteristics
Facility Complexity
The interaction between ADL performance status and facility complexity was statistically significant. Specifically, compared with the relationship between ADL performance status and occupational therapy utilization among veterans receiving care in low-complexity facilities, the relationship was weaker among veterans receiving care at medium-complexity (risk ratio [RR] = 0.52; 95% CI [0.400, 0.666]; p < .001) and high-complexity (RR = 0.61; 95% CI [0.507, 0.732]; p < .001) facilities. As depicted in Figure 2A, among veterans receiving care in low-complexity facilities, ADL impairment was associated with substantially increased probability of receiving occupational therapy, suggesting that ADL performance is a primary driver of access to occupational therapy. This was not the case for veterans receiving care in medium-complexity facilities, and the relationship was diminished within high-complexity facilities.
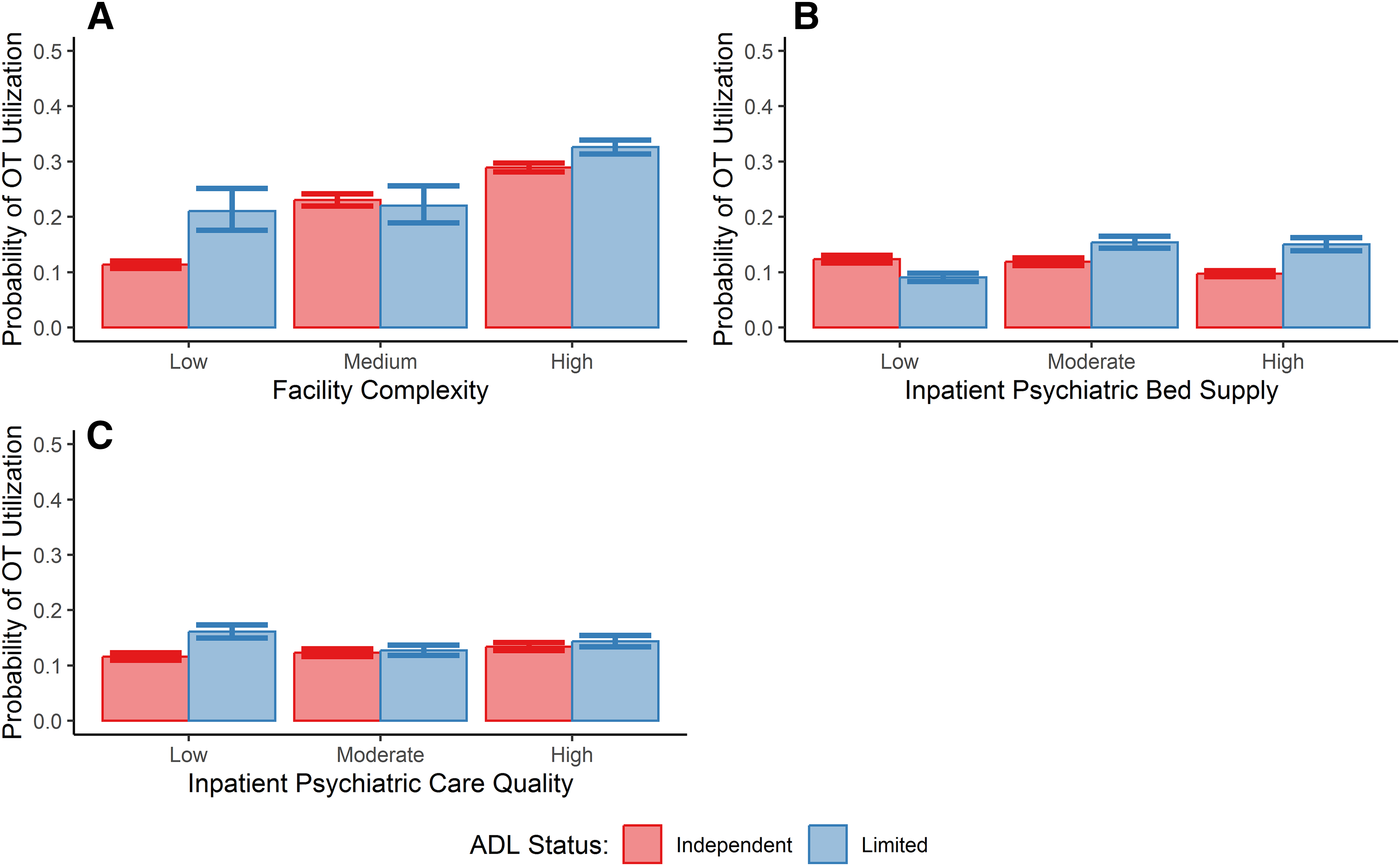
Predicted probability of occupational therapy (OT) utilization versus (A) facility complexity, (B) inpatient psychiatric bed supply, and (C) inpatient psychiatric care quality by status for performing activities of daily living (ADLs).
Inpatient Psychiatric Bed Supply
The interaction between ADL performance status and bed supply was also statistically significant, such that, relative to veterans receiving care in units with a low psychiatric bed supply, the relationship between ADL performance status and occupational therapy utilization differed among veterans receiving care at facilities with a moderate bed supply (RR = 1.76; 95% CI [1.615, 1.928]; p < .001) and a high bed supply (RR = 2.11; 95% CI [1.917, 2.326]; p < .001). Figure 2B illustrates that in facilities with a moderate and high bed supply, veterans with ADL limitations were more likely to receive occupational therapy, suggesting that this indicator of need drives access. Conversely, in facilities with a low bed supply, veterans with ADL limitations were actually less likely to receive occupational therapy.
Inpatient Psychiatric Care Quality
Last, we observed a statistically significant interaction between ADL performance status and inpatient psychiatric care quality. Relative to veterans receiving care in facilities with low care quality, the relationship between ADL performance status and occupational therapy utilization tended to be weaker among veterans receiving care in facilities with moderate (RR = 0.74; 95% CI [0.681, 0.813]; p < .001) and high (RR = 0.77; 95% CI [0.707, 0.842]; p < .001) care quality. Figure 2C indicates that in facilities with low care quality, those with ADL limitations were substantially more likely to access occupational therapy. This was not evident in facilities with moderate to high care quality.
Discussion
This was, to our knowledge, the first study to investigate disparities in access to inpatient psychiatric occupational therapy services in the VHA. Results indicate a tendency for ADL limitations—an important indicator of need for occupational therapy—to be associated with a greater likelihood of receiving occupational therapy. However, our analysis yielded evidence of disparities in access to occupational therapy that were based on facility-level characteristics and race. This study is a necessary first step in a line of inquiry aimed at thoroughly understanding inpatient psychiatric occupational therapy utilization in the VHA. What remains unclear are the specific mechanisms that underlie observed disparities in access, as well as typical care processes that enable access to inpatient psychiatric occupational therapy, both of which will be the subject of a subsequent qualitative study to be reported elsewhere. This body of work will lay the foundation for the development and evaluation of strategies aimed at promoting equitable access to occupational therapy services among veterans receiving inpatient psychiatric care.
Veterans with ADL limitations were more likely to access inpatient psychiatric occupational therapy, suggesting that, generally, such services are allocated to veterans in need. However, our findings reveal potential evidence of unmet need. For example, only 25% of veterans in our sample received occupational therapy, a proportion substantially lower than those observed in inpatient medical settings, which tend to range between 44% and 63% (Kinney et al., 2021, 2022; Kumar et al., 2019). The results highlight the need to understand and modify specific barriers to accessing occupational therapy services in VHA inpatient psychiatric settings. Additional study findings indicate facility-level and racial disparities in access to occupational therapy, which can inform future research aimed at clarifying the exact nature of the barriers to accessing these valuable services.
Facility complexity and inpatient psychiatric care quality influenced access to occupational therapy in multiple ways. Veterans who received care in facilities with higher complexity as well as facilities with higher care quality were more likely to receive occupational therapy, suggesting that better resourced facilities and those that were more adherent to recommended procedures may have the infrastructure necessary (e.g., a high supply of occupational therapy practitioners) to allocate occupational therapy services more frequently. Furthermore, interactions indicated that ADL limitations were a weaker driver of access among veterans receiving care in facilities with higher complexity and care quality, suggesting that the conception of need for occupational therapy may differ in these facilities. For example, targets of occupational therapy intervention in psychiatric settings are not restricted to ADL limitations, and they include challenges with performing instrumental ADLs (IADLs; e.g., medication management), recreational activities, and other activities that the client considers meaningful (Burson et al., 2017). Perhaps facilities with fewer resources may prioritize the allocation of scarce occupational therapy resources to those with ADL limitations, guided by the reasonable assumption that independence with self-care is an urgent priority. Conversely, facilities with more resources may have the infrastructure to expand targets of occupational therapy intervention beyond ADL limitations. Future research should investigate the relationship between inpatient psychiatric occupational therapy utilization and other relevant indicators of facility resources (e.g., occupational therapy staffing levels) and care quality (e.g., veteran satisfaction). Our planned qualitative work will shed additional light on potential mechanisms underlying the relationship between facility resources, inpatient psychiatric care quality, and occupational therapy utilization.
Our findings indicate that, regardless of ADL limitations, Black veterans were less likely to receive occupational therapy compared with their White, non-Hispanic, counterparts. This aligns with prior research documenting racial and ethnic disparities in access to occupational therapy among patients hospitalized for medical conditions (Kinney et al., 2022). Furthermore, a prior study found that Black veterans were less likely than White veterans to access VHA inpatient psychiatric services (Bradford et al., 2022), a finding that contradicted results found in non-VHA systems (Snowden et al., 2009). Our study is the first, to our knowledge, to document such racial disparities in access to occupational therapy services within VHA inpatient psychiatric settings. It is important to note that such racial categories are sociocultural constructions and should be considered surrogate indicators of structural marginalization, leaving certain groups at disproportionate exposure to access barriers (e.g., discrimination; Hardeman et al., 2022; National Institute on Minority Health and Health Disparities, 2021). As such, research aimed at understanding the specific mechanisms by which racial disparities in access to inpatient psychiatric occupational therapy occur is urgently needed.
A counterintuitive relationship between inpatient psychiatric bed supply and access to occupational therapy was observed. Findings suggest that access to occupational therapy is relatively higher in smaller inpatient psychiatric units, and such access may be driven by factors other than ADL limitations. Future research is needed to clarify the relationship between bed supply and inpatient psychiatric occupational therapy utilization. For example, we used the absolute number of available beds, and future research should account for occupancy rates, which may have a distinct influence on care processes. Indeed, prior research found that inpatient psychiatric bed occupancy, but not the absolute number of beds, exhibited the hypothesized relation with suicide within the VHA (Kaboli et al., 2022).
Future research should consider an expanded definition of need for occupational therapy in the inpatient psychiatric setting. Occupational therapy practitioners are uniquely equipped to advance recovery-oriented care for veterans with psychiatric conditions by promoting their full integration into the community upon discharge from the inpatient psychiatric setting (Burson et al., 2017; Synovec, 2015). To be clear, ADL limitations are a significant barrier to such community participation and a primary target of occupational therapy intervention, making such challenges an appropriate indicator of need for occupational therapy in this setting. However, ADL limitations were documented in only 8% of veterans, and, as previously noted, occupational therapy practitioners promote independence in a much wider range of activities reflecting full participation in society (e.g., IADLs; Burson et al., 2017). As such, future research should examine whether engagement in a wider variety of activities drives access to occupational therapy, and whether the disparities in access observed in this study persist. Routine assessment of such activities in the inpatient psychiatric setting (e.g., inclusion in nursing assessments) would facilitate this important line of inquiry while eliciting important targets of intervention for acute and postacute stages of recovery.
Study Limitations
Measuring ADL limitations in this sample required validating an automated process by which such information was extracted from nursing assessments. We were unable to account for the validity and reliability with which ADL performance was evaluated. Furthermore, such ADL information was missing for a notable portion of our sample, and it is unclear whether results generalize to all veterans who receive inpatient psychiatric care. Future research should attempt to examine study relationships in a representative sample using standardized assessments of ADL performance and other activities. We were also unable to account for all potentially confounding variables (e.g., prior living situation), and future research should attempt to collect such information. Last, we excluded veterans who received care at VHA inpatient psychiatric facilities at which occupational therapy services were unavailable. Although these exclusion criteria were appropriate for the present analysis, future research should examine whether the population of veterans at such facilities have a disproportionate exposure to social disadvantage relative to veterans receiving care at facilities with occupational therapy services available. Such research would shed additional light on potential disparities in access to these beneficial services.
Implications for Occupational Therapy Practice
Our findings have the following implications for occupational therapy practice: ▪ Occupational therapy utilization in VHA inpatient psychiatric settings is driven in part by clinical need, but researchers, practitioners, and policymakers must be aware of potential disparities in access to these beneficial services. ▪ Our findings lay the foundation for an in-depth exploration of specific and modifiable determinants of access to occupational therapy in this setting, thereby informing the development of strategies that modify practice and/or policy to promote equitable access to these beneficial services.
Conclusion
Before the present study, veterans’ access to occupational therapy services within VHA inpatient psychiatric settings was poorly understood. In a national sample of veterans receiving inpatient psychiatric care, we found that, although occupational therapy resources are generally allocated to those in need, evidence of potential disparities in access to these services exists. The present findings lay the foundation for a body of work aimed at developing and evaluating strategies that promote the equitable distribution of inpatient psychiatric occupational therapy to veterans in need.
Supplemental Material
Supplementary material for Facility-Level and Racial Disparities in Access to Inpatient Psychiatric Occupational Therapy Services in the Veterans Health Administration
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050583.pdf for Facility-Level and Racial Disparities in Access to Inpatient Psychiatric Occupational Therapy Services in the Veterans Health Administration by Adam R. Kinney, Molly E. Penzenik, Jeri E. Forster, Frederica O’Donnell and Lisa A. Brenner in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This work does not necessarily represent the views of the U.S. Department of Veterans Affairs (VA) or the U.S. Government. Lisa A. Brenner and Jeri E. Forster each report grants from the VA, U.S. Department of Defense, National Institutes of Health, and the State of Colorado. Lisa A. Brenner received editorial remuneration from Wolters Kluwer and the Rand Corporation, as well as royalties from the American Psychological Association and Oxford University Press. In addition, she consults with sports leagues through her university affiliation. This work was supported by a Health Services Research Grant from the American Occupational Therapy Foundation to Adam R. Kinney.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.