
Abstract
This pilot study offers promising evidence that supports the use of modified single joystick–operated ride-on toys for children with hemiplegic cerebral palsy.
Children with hemiplegic cerebral palsy (HCP) have difficulties using their affected upper extremity (UE) for self-care, recreation, and academic tasks (Arner et al., 2008; Arnould et al., 2007). These limitations may impair children’s participation in activities of daily living and quality of life, compared with neurotypical peers (Bingol et al., 2023; Russo et al., 2008; Tonmukayakul et al., 2020). To address these challenges, children frequently receive long-term services (Novak et al., 2020). Current evidence suggests that task-oriented approaches that are based on motor-learning principles and that encourage repetitive, goal-directed practice of UE activities within real-world situations are most effective in producing meaningful functional improvements in children with HCP (Demers et al., 2021; Novak et al., 2020; Taghizadeh et al., 2023). One commonly used evidence-based approach is constraint-induced movement therapy (CIMT; Hoare et al., 2019). Approaches that are based on CIMT involve constraining the child’s unaffected UE and engaging them in tasks that promote intensive unimanual practice with the affected UE (Eliasson et al., 2005; Gordon et al., 2005). The crucial factor associated with improvements in UE function after CIMT is training intensity (Ramey et al., 2021; Sakzewski et al., 2016). There is growing consensus that around 40 to 60 hr or more of threshold dosing involving task-oriented practice is required to produce clinically meaningful improvements in children’s UE function (Gannotti et al., 2014; Jackman et al., 2020).
It is often challenging to achieve this optimal high intensity of treatment dosing through school- or clinic-based sessions of occupational therapy or physical therapy both of which are typically provided only once or twice a week (Palisano et al., 2012). Moreover, training activities may require extensive therapist handling and expertise, and clinicians frequently struggle to sustain child engagement during therapy (Meyns et al., 2018 ; Tatla et al., 2013; Weightman et al., 2011). In fact, the Occupational Therapy Practice Framework recommendation is for services to be motivating and engaging for children to produce meaningful improvements in functional performance (American Occupational Therapy Association, 2020). Low levels of engagement in conventional therapies can negatively influence children’s motivation to practice training activities (Majnemer et al., 2010). In fact, therapists and parents acknowledge that child motivation is strongly associated with functional motor gains among children with cerebral palsy (CP; Bartlett & Palisano, 2002; Majnemer, 2011). Moreover, sole reliance on conventional activities and clinic- or school-based rehabilitation models limits the carryover of training practice into children’s naturalistic environments (Beckers et al., 2020; Novak et al., 2009). Such concerns call for the diversification of current therapy approaches and the exploration of engaging therapy adjuncts to expand children’s opportunities for self-initiated and goal-directed practice with their affected UE across multiple real-world settings, including home, school, clinic, and other community settings.
Our team is investigating the acceptability and efficacy associated with using joystick-operated ride-on toys (ROTs) as motivating and child-preferred adjuncts to conventional therapy to promote motor skills in the affected UE among children with HCP (Amonkar et al., 2022; Srinivasan et al., 2023). Powered ROTs are universally appealing to children and may serve as playful and effective tools to engage young learners. In fact, modified ROTs have been previously used with children with mobility impairments such as CP, spina bifida, Down syndrome, and other complex medical conditions as a means of early mobility (Huang et al., 2014; Logan et al., 2018; Ragonesi & Galloway, 2012). These studies have indicated that the early introduction of powered mobility can enhance children’s mobility skills, accelerate their cognitive and social communication development, and increase community participation (Bray et al., 2020; Casey et al., 2013; Guerette et al., 2013; Jones et al., 2012). We are evaluating the use of ROTs for a different application: to boost spontaneous affected UE use and motor function in children with HCP. We propose that joystick-operated ROTs are easy to use and cost-effective adjuncts that can be used by clinicians and caregivers to incentivize and augment school- and clinic-based UE therapy by encouraging children to use their affected UE for purposeful navigation within their physical environments. We hypothesize that the versatility provided by the ROT training paradigm allows spontaneous active child engagement across a variety of natural and built environments (e.g., playground, driveway, parking lot, school, home). The intrinsically motivating nature of such an activity makes it a valuable and effective therapeutic tool that boosts treatment adherence, engagement, and dosing to ultimately produce significant improvements in affected UE function in children with HCP.
Previously, we reported that implementation of ROT training in a summer camp was feasible and was well received by children, caregivers, and clinicians as reported on exit questionnaires (Amonkar et al., 2022). Moreover, in combination with other camp-based activities, ROT training led to an increase in all-day habitual activity in the affected UE, measured using accelerometers (Srinivasan et al., 2023). In this article, we report on acceptability-related outcomes that are associated with incorporation of ROT training into a CIMT-based camp’s existing structure. We use session adherence and child engagement during training sessions as metrics to assess child acceptance of ROT training. Moreover, we also report preliminary data on the effects of ROT training in combination with camp activities on children’s affected UE motor function, which we assessed using a standardized test and training-specific measures of navigation accuracy. Our hypotheses were as follows: ▪ Children will demonstrate high rates of adherence, high levels of positive behavior and affect, and high task-oriented attention during ROT training sessions. ▪ Children will demonstrate improvements in manual dexterity during navigation across training weeks, and these motor performance variables will be positively correlated with child engagement measures, suggesting that high levels of task engagement during ROT sessions will be associated with improvements in manual dexterity and/or maneuvering skill during ROT navigation. ▪ Children will demonstrate improvements in affected UE motor function on a standardized measure after completing the combined program (ROT training plus other camp activities).
Method
Participants
Eleven children (6 male, 5 female) participated in the single-group, pretest-posttest study: Ages were 3 to 14 yr (M = 6.54, SD = 2.76); 8 had right-sided weakness, and 3 had left-sided weakness (Srinivasan et al., 2023), with a diagnosis of HCP and clear asymmetry in UE strength and/or control. All children had hypertonia in their affected extremities. Children were included if they had no history of physical trauma or surgery in the past 3 mo, had no visual impairments, were able to sustain supported sitting for at least 20 min, were able to use their arm and/or body to activate a joystick within reaching distance, and were within device weight limits (100 lbs.). Six children were born full term, 4 were preterm, and information was missing for 1 child who was adopted. Four children had underlying conditions such as epilepsy, tuberous sclerosis, or infantile spasms. At baseline, scores on the Manual Ability Classification System (Eliasson et al., 2006) indicated that children had a mild to moderate level of impairment (5 children at Level II, 5 children at Level III, and 1 child at Level IV of the MACS, where higher scores indicate greater level of impairment). Children’s functional skills on the Pediatric Evaluation of Disability Inventory (Haley, 1992) were as follows: self-care, M = 57.24 (SE = 8.4); mobility, M = 63.74 (SE = 5.3); and social function, M = 65.82 (SE = 4.2). All children fell within 2 SD from the mean expected for their age. The study was approved by the Institutional Review Board at the University of Connecticut. Participants were recruited through convenience sampling from an annually held summer camp for children with HCP. Parental permission and written or oral child assent were obtained before study commencement. Pretests were conducted in the week before camp, and posttests were conducted within a week of camp completion. All testing and training sessions were videotaped for later scoring.
Procedures
Camp Structure
The structure of the 3-wk camp was based on principles of modified CIMT, in which the child’s unaffected UE was restrained in a removable thermoplastic cast for 6 hr/day while children were encouraged to use the affected UE for goal-oriented, gross motor, and fine motor activities, as well as functional activities of daily living such as eating and toileting (for details, see Amonkar et al., 2022; Srinivasan et al., 2023). Children received a total of 90 hr of CIMT.
ROT Navigation Training
The ROT training was incorporated as part of the camp routine for 3 wk, 5 days/wk, at 20 to 30 min per session—a total dose of approximately 8 hr. We used a commercially available dual joystick–operated ROT (Wild ThingTM; Figure 1) that was modified to allow operation in a single-joystick mode provided on the child’s affected side while they wore a cast on their less affected UE (Srinivasan et al., 2023). Children wore helmets and seatbelts while driving. In addition to changing the ROT controls, the research team made modifications to:

Ride-on toy (Power Wheels® Wild Thing) used in the study.
▪ improve access to the joystick by adding a foam ball on top of the joystick to aid grasp,
▪ provide external support through a built-up support structure created through PVC pipes, and
▪ improve comfort and postural support by providing additional trunk support (with pool noodles, kickboards) as needed by the child.
The sessions were consistent with the camp’s thematic activities. Each session included navigational challenges and UE activities. Two researchers conducted the training sessions for all children across training weeks and following a manualized progressively challenging protocol. Navigational activities required the use of proximal and distal UE muscles to push and pull the joystick to move the ROT along progressively challenging paths (e.g., straight, roundabout, slalom, and obstacle courses). The UE tasks that were completed at intermediate stations during navigation required reaching, grasping, manipulation, and release of toys and/or props and were progressed in terms of movement excursion, forces, and manual dexterity required. The progression of training activities was based on the success achieved in 80% of trials or tasks (three of five times that the tasks or paths were repeated). Trainers provided manual assistance as needed and weaned assistance across training weeks. The training session duration was split into fairly equal time for navigation and UE manipulation activities.
Our program was based on principles of motor learning that recommend that training be aligned with the goals and interests of the learner to facilitate longer, more intensive, and frequent active engagement that, in turn, promotes long-term functional gains (Demers et al., 2021; Meyer-Heim & van Hedel, 2013; Rameckers et al., 2019; Taghizadeh et al., 2023). We incorporated evidence-based strategies to maximize child engagement, including the use of child-preferred activities that promoted simultaneous motor, perceptual, cognitive, and emotional engagement. Such activities that provide the ‘just-right’ challenge through gradually progressive tasks are known to foster autonomy through self-initiated exploration and provide active problem-solving opportunities, along with multimodal feedback (Demers et al., 2021; El-Shamy, 2018; Levin et al., 2015).
Measures and Materials
The first author (Sudha Srinivasan) trained graduate and undergraduate students to assess changes in child behavior (affect, attention, motor skills, and navigational accuracy) on the basis of video data. For each measure, two coders coded 15% of total videos to establish inter- and intra-rater reliabilities of over 90%. Discrepancies between coders were resolved through consensus coding with the first author. Following reliability procedures, for each scheme, a single coder coded the remaining dataset.
Measures of Training Adherence and Satisfaction
We tracked the number of ROT sessions completed as a measure of training adherence. To track children’s acceptance of training sessions, we coded the child’s behavior and affect as well as attention through video data at three time points: early (Week 1), midpoint (Week 2), and late (Week 3) sessions. For each time point, two sessions within that week (from the early and late parts of each week) were coded using Datavyu video-coding software. The sessions chosen were kept consistent across all children in the study (except if a child was unwell or absent for the day). We averaged the child’s performance across two sessions per week to obtain a single representative estimate of the child’s performance each week (i.e., total of three time points across the 3 wk of training). We scored measures of behavioral–affective states and attention to assess acceptability of the training.
Behavioral–Affective States
We coded child behavior as a proxy of acceptance or engagement during training sessions. We observed children’s facial expressions, behavior, and body language and coded the percent duration of time spent in positive or interested behavior (i.e., smiling, cooperating) and negative behavior (i.e., fussing, angry, crying, noncompliance) across weeks.
Attention
We coded children’s attentional targets during training sessions as another measure of engagement. We classified attention as being directed toward device handling (i.e., looking at the joystick or hand), task oriented (i.e., looking at the path, obstacles, or props), socially directed (i.e., looking at trainers), or directed elsewhere (i.e., distracted or looking at task-unrelated objects). We analyzed training-related changes in the percent duration of attention toward different targets across training weeks.
Training-Specific Measures of Affected Upper Extremity Movement Control During Sessions
Navigational Bouts
We coded the amount of assistance required during ROT navigation. Movement bouts were classified as being unassisted (child controlled the joystick independently) or assisted (child required partial or total assistance from the trainer). We analyzed changes in the average percent duration of time of unassisted navigation across sessions.
Stationary Bouts
We also coded the times when the ROT was not in motion and classified them as being either unintentional (child was unable to maintain sustained joystick pushing or pulling to maneuver the ROT because of poor UE muscle control or fatigue) or intentional (child stopped intentionally to complete a task or talk to the trainers). We analyzed changes in the average percent duration of time spent in unintentional stops across sessions.
Unintentional Contact With Objects
We also coded the frequency of unintentional contacts or bumps against stationary (e.g., walls or doors) or movable (e.g., cones, cups, chairs) objects or obstacles during navigation. Unintentional contacts were only coded at two time points (midpoint and late sessions) because early sessions had few obstacles along the navigational path. We report changes in the rates per minute of unintentional contacts with objects across training weeks.
Standardized Test of Upper Extremity Motor Function
We assessed the effects of ROT training in combination with camp activities on affected UE function of children using a standardized test administered at pretest and posttest. The Quality of Upper Extremity Skills Test (QUEST; DeMatteo et al., 1992) is a 36-item, criterion-referenced test that assesses UE movement quality and range of motion using unimanual items scored on a dichotomous scale. The four domains assessed include dissociated movements, grasps, protective extension, and weight bearing. The scale has been validated for children up to age 12 yr and has excellent reliability (Thorley et al., 2012a, 2012b). We analyzed changes in the total and domain scores of the QUEST from pretest to posttest. Note that all QUEST scores are calculated as percentages and have a maximum score of 100, with higher scores representing better quality of movement (DeMatteo et al., 1992). One child in our study was over age 12 yr. We conducted our preliminary analyses with and without this child included, and our trends remained the same. Therefore, we decided to report on data from all 11 children in the study.
Statistical Analysis
All data satisfied assumptions of parametric statistics. Therefore, we used repeated measures analyses of variance (ANOVAs) to analyze training-specific variables of child engagement (behavioral–affective states and attention) and motor performance (navigational and stationary bouts) across the three time points (early, midpoint, and late sessions). We also conducted a repeated-measures ANOVA to assess the combined effects of the camp-based program on total and domain QUEST scores with time (pretest and posttest) and QUEST scores (total and four domain scores) as within-subject factors. If the ANOVAs indicated a significant main effect and an interaction involving the same factor, then we conducted post hoc t tests to evaluate the significant interactions only. We also conducted a dependent t test to assess training-related changes in the rates of unintentional contact with objects (from midpoint to late sessions). Statistical significance was set at p ≤ .05. Effect sizes (ESs) are reported using standardized mean difference (SMD) values, with Hedges’s g (Hedges, 1981), along with the 95% confidence intervals (CIs) around the SMD. ESs were calculated as posttest–pretest or late–early session differences (except for stationary bouts and unintentional contact with objects for which we calculated early or mid-late session differences), so that positive values indicate improvements in assessed outcomes. The SMD values were classified as small (.2–.5), medium (.5–.8), or large (≥.8; Cohen, 1988). Pairwise Pearson’s product–moment correlation coefficients were calculated to evaluate the magnitude and direction of association between training-specific motor and behavioral variables. Correlations were classified as small (<.2), medium (.2–.5), or large (≥.5; Cohen, 1988). There were no missing data for any of our behavioral measures.
Results
Measures of Training Adherence and Child Engagement
Adherence With Training
The average adherence rate with training was 93.33%. Three children missed one session each, because of sickness, scheduling conflicts, or holiday plans; and 1 child missed three sessions in total because of sickness. Children drove the toy for 15 to 20 min/d (M = 15.5, SD = 2.8, range = 11–35 min). The wide range for session duration was because a few children were initially reluctant to use their affected UE to drive the toy but eventually engaged in longer sessions as their ability to control the joystick improved with repeated practice. None of the children refused to participate in training sessions.
Behavioral–Affective States
The ANOVA indicated a significant main effect of behavior–affect type, F(1, 10) = 344.9, p < .001, η2 = 0.972. Across sessions, children spent greater time in positive compared with negative behavior (Figure 2), with all 11 children following group trends: positive, M = 93.96 (SD = 9.49); negative, M = 6.03 (SD = 9.49); t(32) = 26.60, p ≤ .001; SMD (95% CI) = −8.55 (−13.23, −3.87).
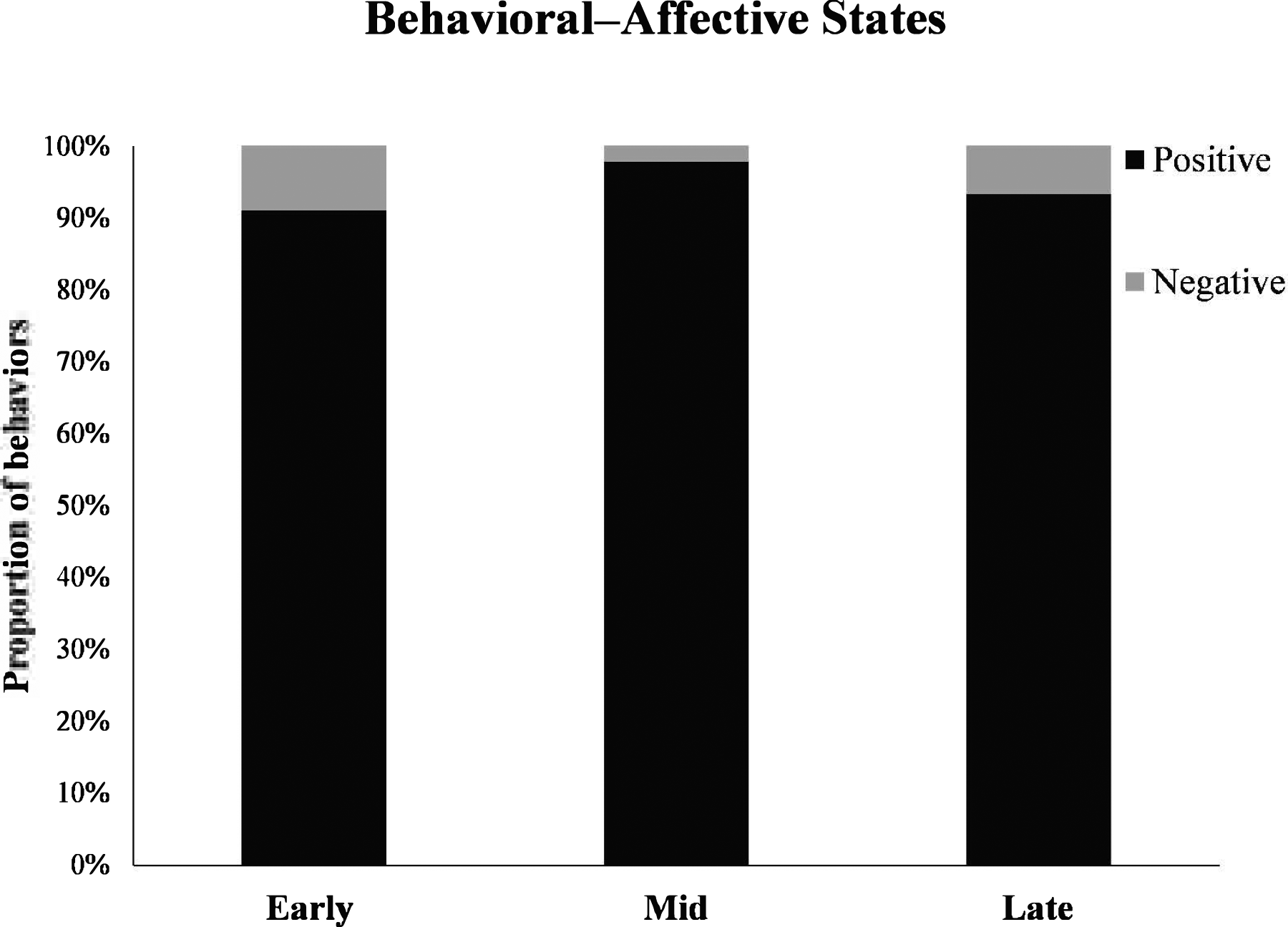
Group data on children’s behavioral–affective states during the 3-wk ride-on toy navigation training program. Mid = midpoint.
Attentional States
The ANOVA indicated a significant main effect of attention type, F(1.4, 14.8) = 44.0, p < .001, η2 = 0.815; and an Attention Type × Time interaction, F(2.2, 22.2) = 12.6, p < .001, η2 = 0.558. Children showed a decrease in attention toward device handling and elsewhere, with a concurrent increase in task-appropriate and socially directed attention across training weeks. Specifically, post hoc t tests indicated a significant decrease of small-to-large size in the percent duration of attention directed toward device handling (Figure 3) from early to midpoint sessions, t(10) = 5.42, p < .001, SMD = −0.676, 95% CI [−1.43, 0.07]; midpoint to late sessions, t(10) = 2.25, p = .048, SMD = −0.179, 95% CI [−0.84, 0.48]; and early to late sessions, t(10) = 5.30, p < .001, SMD = −0.813, 95% CI [−1.60, −0.01]; with 10 to 11 children following group trends. There was also a significant decrease in attention toward elsewhere (Figure 3) from early to midpoint sessions in 9 out of 11 children, t(10) = 2.28, p = .046, SMD = −0.338, 95% CI [−1.02, 0.34]. In contrast, there was a significant increase in task-oriented and socially directed attention across sessions (Figure 3). Specifically, 10 out of 11 children demonstrated medium-to-large increases in task-oriented attention from early to midpoint sessions, t(10) = 3.77, p = .004, SMD = 0.847, 95% CI [0.04, 1.65]; and from early to late sessions, t(10) = 2.72, p = .021, SMD = 0.691, 95% CI [−0.06, 1.45]. Furthermore, 9 out of 11 children showed a medium-sized increase in socially directed attention from midpoint to late training sessions, t(10) = 2.87, p = .017, SMD = 0.76, 95% CI [−0.01, 1.54]. Overall, from early to late sessions, children reduced attention directed toward the mechanics of driving and instead were able to dedicate more attention toward the course to plan their navigation within the environment.
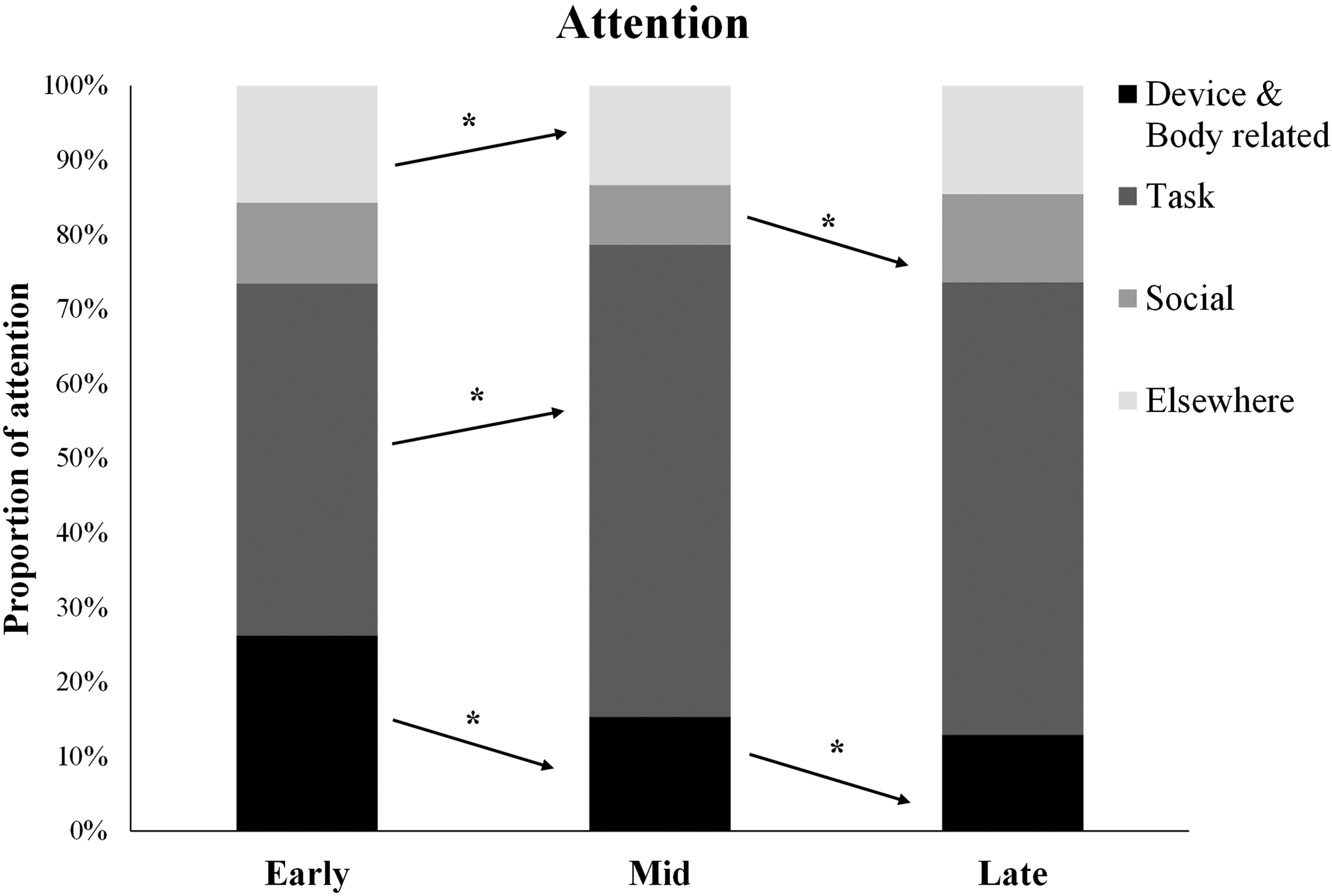
Group data on training-related changes in children’s attentional patterns during the 3-wk ride-on toy navigation training program.
Training-Specific Measures of Navigational Control
Navigational Bouts
The ANOVA indicated a significant main effect of the amount of assistance required, F(1, 10) = 13.512, p = .004, η2 = 0.0575; and an interaction effect of Navigational Bouts × Time, F(1.3, 13.1) = 9.831, p = .005, η2 = 0.496. Post hoc analyses suggested that children showed small increases in the percent time of unassisted navigation (early, M = 63.73, SD = 20.1; midpoint, M = 70.73, SD = 23.7; and late, M = 73.91, SD = 24.1) from early to midpoint sessions (SMD = 0.293, 95% CI [−0.38, 0.97]) and from early to late sessions (SMD = 0.451, 95% CI [−0.25, 1.15]), with 10 children following the group trends.
Stationary Bouts
We found a significant main effect of stationary bouts, F(1, 10) = 840.37, p <.001, η2 = 0.988; and a Stationary Bout × Time interaction, F(1.3, 13.3) = 10.50, p < .001, η2 = 0.512. There was a significant small to large decrease in time spent in unintentional stops (early, M = 19.6, SD = 6.5; midpoint, M = 14.74, SD = 5.2; and late, M = 12.39, SD = 4.3) from early to midpoint sessions (SMD = −0.624, 95% CI [−1.36, 0.11]), midpoint to late sessions (SMD = −0.416, 95% CI [−1.11, 0.28]), and early to late sessions (SMD = −0.958, 95% CI [−1.79, −0.11]), with 9 of 10 to 11 children following the group trends.
Unintentional Contact With Objects
Children showed a significantly large reduction in the rates of unintentional object contacts during navigation (midpoint, M = 1.10, SD = 0.47; late, M = 0.69, SD = 0.40) from midpoint to late sessions (SMD = −0.79, 95% CI [−1.57, −0.003]), with 9 out of 11 children following group trends.
Associations Between Task Engagement and Motor Performance Measures During ROT Navigation
Correlations between child engagement and motor performance variables suggested that positive behavior was positively correlated with unassisted navigation (Table 1). Children who enjoyed the training were more likely to drive the ROT independently. Children who engaged in high levels of task-appropriate attention also engaged in a greater duration of unassisted navigation and lower bouts of unintentional stops during ROT sessions. Conversely, children who directed greater attention toward device handling showed lower levels of unassisted navigation and, instead, engaged in greater unintentional stops (Table 1). As the children’s need to look at the joystick–hand interface reduced, they were able to direct greater attention to the paths and also showed greater unassisted navigation during sessions. Finally, positive behavior–affect was positively correlated with task-appropriate attention and negatively correlated with attention directed elsewhere.
Correlations Between Child Engagement and Motor Performance Variables During Ride-On Toy Training Sessions
Note. p values are in parentheses.
*Correlation is significant at p ≤ .05 (two-tailed).
**Correlation is significant at p ≤ .001 (two-tailed).
Standardized Measure of Upper Extremity Motor Function
The ANOVA indicated a significant main effect of time, F(1, 10) = 43.701, p < .001, η2 = 0.814. Further post hoc analysis suggested that children improved their motor performance from pretest (M = 64.23, SE = 1.84) to posttest (M = 73.34, SE = 1.94, p < .001). Children’s standardized tests scores improved significantly over the 3-wk training period. Changes in total QUEST scores and individual domains of the QUEST are reported in Table 2.
Training-Related Changes in Motor Performance on a Standardized Test After the Ride-On Toy Navigation Program
Note. CI = confidence interval; QUEST = Quality of Upper Extremity Skills Test.
*p < .001 (two-tailed); Bonferroni correction was applied for multiple comparisons.
Discussion
This paper discusses the acceptability and utility of joystick-operated ROT training when incorporated into a 3-wk CIMT camp program focused on improving affected UE motor function in children with HCP. The ROT training was well accepted in the existing camp structure, as indicated by high rates of child adherence. Children sustained engagement with ROT training activities across weeks. More than 80% of the children improved independent and skilled navigation using their affected UE. Significant correlations between motor and child engagement variables suggest that the level of engagement during ROT training was associated with the extent of independent and skilled use of their affected UE for maneuvering the ROT.
Moreover, QUEST data, which measured overall motor changes as a result of the entire camp (inclusive of ROT training), suggested that 100% of the children demonstrated medium-to-large improvements in manual function on the standardized test.
Child Engagement During ROT Navigation Training
It was encouraging to see sustained task engagement (high positive behavior and affect and task-appropriate attention) across sessions. While learning to drive, children initially directed greater attention toward the hand–joystick interface, but as their manual abilities improved, they began to rely more on kinesthetic feedback and were instead able to focus on the driving courses. We propose that, as children progressed from novice to advanced learning stages, they began to use sensory input in an anticipatory fashion, reduced reliance on cognitive resources, and improved the skillful and adaptive use of their affected UE during ROT navigation (Fitts & Posner, 1967; Shumway-Cook et al., 2023).
We hypothesize that the training may have affected children’s mastery motivation. Mastery motivation is defined as the individual’s intrinsic desire to explore and control their environment and influences their persistent engagement with moderately challenging tasks (Jennings et al., 1988; Miller et al., 2016). In fact, mastery motivation is critical for determining the success of interventions (Damiano, 2006; Palisano et al., 2012). Children with CP tend to have lower levels of mastery motivation and task persistence, with more negative responses to failure compared with neurotypical peers (Majnemer et al., 2010; Morgan et al., 2009). Despite the ROT training being challenging, it evoked positive engagement in children. Past research suggests that training environments similar to ours that are fun and innovative, offer choices, provide autonomy, and optimally scaffold skill development help enhance mastery and sustain participant engagement (Gilmore et al., 2010; Morgan et al., 2016). In fact, more than 90% of children requested that the ROT program be repeated (Amonkar et al., 2022). On the basis of our findings, we propose that ROTs can be used as engaging therapeutic adjuncts to boost motivation and adherence with conventional therapy to maximize active UE use in children with HCP.
Motor Performance Is Linked to Child Engagement During Navigation
Motor performance during navigation was linked to the behavior–affective and attentional states of children. Children with greater positive behavior or affect and task-appropriate attention navigated more independently, with fewer stops associated with poor muscle control and fatigue. Conversely, greater fatigue and unintentional stops, as well as the need for more assistance, was associated with greater attention directed toward the mechanics of driving. These trends align with the principles of motor development that suggest a shift from the reliance on vision to using kinesthetic–proprioceptive input as children become proficient in specific motor skills (Shumway-Cook et al., 2023). Other studies with ROTs have also suggested increased visual attention toward switch controls when children initially learn to drive powered ROTs (Chen et al., 2021). Children’s perception of the ROT activity as being “fun” may have contributed to high levels of positive engagement during ROT sessions. This positive perception may have motivated children to persist with the training, which, over time, in conjunction with other camp activities, may have contributed to practice-induced, plasticity-mediated improvements in motor function (Levin et al., 2015; Majnemer et al., 2010; Morgan et al., 2009).
Improvements in Affected Upper Extremity Motor Function After Intensive Task-Oriented Training
ROT navigation training, in combination with CIMT-based camp activities, led to improvements in motor function in the affected arm in children with HCP. These positive findings may be tied to the nature of the camp-based training program. A recent review suggested that the key ingredients of effective evidence-based motor interventions in CP include the promotion of self-generated movements within children’s naturalistic environments, active problem-solving, and repeated practice of goal-oriented tasks that children perceive as being motivating, rewarding, and enjoyable (Jackman et al., 2022; Novak et al., 2020). By incorporating these principles, our ROT navigation program may help boost treatment dosing as well as children’s motivation and adherence with intensive therapy, which may have contributed to functional gains in UE motor outcomes. ROT navigation is a goal-oriented, functional activity that requires ongoing problem-solving as children perceive changing environmental constraints and layouts, plan their path through space, and organize movements of their affected UE to maneuver the ROT skillfully. Along these lines, Levin and colleagues proposed that enriched training environments that engage the cognitive abilities of learners and provide multisensory feedback are likely to encourage learners to work longer, harder, and more often, thereby promoting learning through neuroplastic mechanisms (Levin et al., 2015). The ROT training afforded functional UE movement patterns (pushing and pulling in multiple directions); we observed that, in the presence of distal muscle weakness, children used proximal UE and trunk muscles to move the joystick. Accordingly, prior work suggests that task-oriented approaches that foster active movements and problem solving are more effective in improving UE function compared with interventions with a focus on isolated joint and muscle training through therapist handling (Damiano et al., 2021; Taghizadeh et al., 2023).
Our findings are also aligned with results of studies that used novel child-friendly approaches such as virtual reality, gaming, and robotics to incentivize UE movement in children with CP (Chang et al., 2020; Chen et al., 2021; El-Shamy, 2018; Fasoli et al., 2010; Fluet et al., 2010; Gilliaux et al., 2015; Goyal et al., 2022; Kurt & Şimşek, 2021). Although virtual reality and gaming technologies provide children with immersive opportunities for affected UE use to change the virtual or game world, we argue that real-world navigation within three-dimensional environments poses a unique set of tangible challenges with high ecological validity and potential for functional gains in real-world situations. Specifically, navigation through spaces with different dimensions or layouts (narrow corridors, around corners, avoiding obstacles, etc.), involving different surfaces (grass, concrete, gravel, etc.), and at different inclinations (slopes, ramps, etc.) challenges children’s manual dexterity, force modulation, and motor-planning skills. Moreover, children receive immediate multisensory feedback (visual, kinesthetic, auditory, and vestibular) while driving and, over time, may learn to use this feedback to guide real-world actions. In contrast to some technology-based interventions that require expensive equipment and technical expertise, ROTs are relatively low cost and easy to use for families and clinicians within children’s naturalistic settings. Overall, our findings suggest that a ROT navigation program may serve as an effective tool that, in conjunction with conventional therapy, can promote affected UE spontaneous use and motor function in children with HCP.
Limitations and Future Directions
Our study is limited by a small convenience sample, heterogeneity among participants, and the lack of a control group. We recommend that readers interpret our results with caution considering the inherent limitations of a single-group design. Our present design allows us to evaluate the combined effects of ROT training along with other camp activities on children’s motor skills. Our future studies will involve larger sample sizes with matched control groups to compare the adjunctive effects of ROT training plus conventional therapy with those of conventional therapy provided alone. The QUEST measure used in this study has been validated for children up to age 12 yr. One child in our study was over age 12 yr. However, we confirmed that our overall results did not change even after excluding this child from the analysis. In this study, we did not run predictive analyses between motor and task engagement variables due to a small sample size.
Implications for Occupational Therapy Practice
Therapeutic intervention approaches that promote self-initiated and active task-oriented practice at a high intensity are most effective in producing functional improvements in children with CP (Jackman et al., 2020; Novak et al., 2020). Moreover, there is growing emphasis on developing child- and family-centric interventions that are intrinsically motivating, fun, and feasible to implement both within and outside conventional therapy contexts (Beckers et al., 2020; Meyns et al., 2018; Tatla et al., 2013). Our study evaluated the acceptability and utility of a novel training program using joystick-operated ROTs. We envision ROTs as child-friendly adjuncts that can be incorporated into conventional occupational therapy to incentivize goal-oriented UE practice; boost training adherence; and, ultimately, facilitate motor function in children with HCP. Modified commercially available ROTs are accessible, age-appropriate, and easy-to-use devices for both clinicians and families to encourage children to use their affected UEs for goal-oriented navigation within their physical environments. The training can challenge children’s perceptual, motor-planning, problem-solving, and movement-control skills in an enjoyable manner and can help increase hours of self-initiated UE practice within diverse environments. Our pilot study findings suggest the use of joystick-operated ROTs as engaging therapy adjuncts for children with hemiplegia. We are currently conducting a larger clinical trial to replicate and extend our present findings to assess the feasibility and benefits of ROT training when delivered jointly by researchers and caregivers within home or community settings for children with HCP.
Conclusion
Our pilot study assessed the acceptability and utility of incorporating single joystick–operated ROT navigation training as part of an existing constraint-based summer camp program aimed at improving UE motor function in children with HCP. Children showed high levels of adherence and engagement (positive behavior and attention) throughout ROT training and improved their navigational control skills across training weeks. We also found associations between child engagement and motor performance variables during ROT navigation. Finally, after the combined camp program inclusive of ROT training, we found improvements in affected UE functional movement skills on a standardized test. Overall, joystick-operated ROTs may be child preferred, easy to implement, and effective adjuncts that clinicians can use to boost treatment dosing within and outside therapy settings to maximize UE motor development among children with HCP.
Footnotes
Acknowledgments
We thank all the children and families who participated in the study, all the undergraduate and graduate students who helped with data collection and analyses, and the camp director and camp staff for supporting the research.