
Abstract
This review evaluated evidence addressing the ability of youth with persistent postconcussion symptoms (PPCS) to complete everyday activities.
Concussion (also referred to as mild traumatic brain injury [mTBI]) among youth is a significant public health concern that is gaining increased attention (Centers for Disease Control and Prevention [CDC], 2022). Compared with other age groups, youth have one of the highest rates of emergency department visits related to TBI (CDC, 2022). This is concerning because youth are especially vulnerable to chemical and metabolic changes after concussion because of ongoing myelination of axons in the brain (CDC, 2022). According to the CDC (2022), youth made 640,000 TBI-related emergency department visits, with mTBI accounting for 70% to 90% of them. Thirty percent of all individuals with mTBI have persistent symptoms 1 mo after their injury (CDC, 2022). These symptoms may include mental health issues, learning and attention difficulties, visual and oculomotor changes, vestibular problems, sleep disturbances, and pain (Patricios et al., 2023).
The most recent consensus statement on concussion in sport recommends that a rehabilitation referral be considered for individuals with postconcussive symptoms that are not improving 2 to 4 wk after injury (Patricios et al., 2023). Youth with concussion may experience disruption in occupational engagement, including school, social participation, leisure activities (Moen et al., 2022), activities of daily living (ADLs), rest and sleep, and instrumental ADLs (Sinnett & Franzsen, 2020). These areas fall within the scope of occupational therapy (American Occupational Therapy Association [AOTA], 2020). The consensus statement heavily focuses on recommendations for returning to sport and school after a sport-related concussion (Patricios et al., 2023), but it lacks guidelines for return to other activities (Moen et al., 2022). To our knowledge, there is limited literature addressing return to other occupations and roles important to youth, such as social participation, leisure activities, ADLs, and sleep. Additionally, evidence related to specific therapeutic interventions for youth with persistent postconcussion symptoms (PPCS) is limited. Haarbauer-Krupa et al. (2018) encouraged practitioners and researchers to acknowledge youth with non–sport- and recreation-related injuries in concussion management and to “provide age-related guidance for return to activities of daily life for all children who sustain a concussion” (p. 247).
Occupational therapy practitioners have the knowledge and skills to consider the interaction between occupational demands and the client’s contexts, performance patterns, and performance skills to maximize occupational performance (AOTA, 2020). With these fundamental skills, occupational therapists can play a unique role in addressing the occupational needs of youth with PPCS; however, occupational therapy is one of the professions least referred to by physicians (Vargo et al., 2016).
Therefore, the purpose of this systematic review is to provide occupational therapists with current evidence related to interventions for youth with PPCS and, specifically, to answer the following question: What is the evidence for interventions within the scope of occupational therapy to improve occupational performance in ADLs, education, play and leisure, social participation, and rest and sleep among youth with PPCS?
Method
Search Strategies and Databases
Embase, PubMed, SportDiscus, CINAHL, and Web of Science were searched from their date of inception through February 7, 2023. A health sciences librarian (Melissa Previtera) created all database-specific searches using a combination of keywords and controlled vocabulary (see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot), with the latter being generated by the Yale Mesh Analyzer (https://mesh.med.yale.edu/). Keyword alternatives and variations were developed from the terms pediatric, concussion, activities of daily living (specifically, school, play, and sleep), and prolonged recovery. Records were added to and deduplicated through EndNote, and a secondary deduplication was then completed through Rayyan (https://www.rayyan.ai/), which was chosen because it was recommended by a medical librarian (Melissa Previtera). Once deduplication was completed, 1,432 unique results were assessed with the inclusion and exclusion criteria. The full search strategy can be found in Table A.2.
Eligibility Criteria
Peer-reviewed journal articles published in English from January 1, 2013, to February 7, 2023, were included. Presentations, conference proceedings, non–peer-reviewed literature, and dissertations were excluded. Additional exclusion criteria included articles on assessment techniques, articles on interventions not within the scope of occupational therapy, studies with participants outside of the targeted age range or who had a diagnosis other than mTBI or concussion, and studies that used outcome measures that were symptom based or were otherwise unrelated to the targeted areas of occupation. All levels of evidence (1–5) were included in the review because we did not expect the search to yield a large number of studies and wanted to be as exhaustive as possible. Systematic reviews that included our population of interest and focused on intervention were hand-searched to identify any studies that were not found in the preliminary search. Ultimately, all systematic reviews were excluded from the search because none of them precisely addressed the question for this review.
The population included individuals ages 3 to 18 yr diagnosed with mTBI or concussion and persistent symptoms beyond the acute phase of injury who received occupational therapy or another rehabilitation service for PPCS. Because there is discrepancy within the literature on the transitional timeline from acute concussion to PPCS, we used the shorter time frame of 2 wk to capture as many appropriate participants as possible. Last, studies were considered for inclusion if they used interventions that fell within the scope of occupational therapy and reported at least one functional outcome related to targeted areas of occupation: ADLs, education, play and leisure, social participation, and rest and sleep.
Study Selection
Two researchers (Alison Heinekamp and Natalie Molnar) independently examined the articles generated by the electronic search. Abstracts and titles were screened using Rayyan software. A third author (Anne Lennon) was responsible for resolving conflicts between researchers. Full text was obtained for articles included after the first round of screening. The full-text articles were uploaded and organized using Zotero software. Using Rayyan, Heinekamp and Molnar then repeated the process to include or exclude full-text articles on the basis of the established criteria. A third researcher, Lennon, resolved conflicts regarding full-text inclusion and exclusion.
Level of Evidence and Quality Appraisal
Levels of evidence were assigned using the Oxford Centre for Evidence-Based Medicine (2009) guidelines. According to this classification system, research is ranked from 1 to 5, with Level 1 indicating the highest level of evidence and Level 5 indicating the lowest. In addition, Level 1a indicates a systematic review and Level 1b indicates a nonsystematic review.
We used the Cochrane Database of Systematic Reviews tool to guide the risk-of-bias assessment for all included studies (Higgins et al., 2016; see Table A.3). Each article was surveyed and rated as having a low risk of bias, high risk of bias, or unclear bias for each bias category. An overall risk-of-bias rating (low, moderate, or high) was given on the basis of the number of categories with a high risk-of-bias rating.
Results
Search Results
The electronic search yielded 1,432 articles for the abstract screening. A total of 1,220 articles were excluded, leaving 212 for full-text screening. We were unable to locate 10 of the 212 articles. This left 202 articles to be included or excluded on the basis of researcher consensus. After full-text screening, 20 articles met the inclusion criteria and were included in the analysis completed independently by two researchers (Heinekamp and Molnar). Figure 1 displays the results of each step of the screening process.
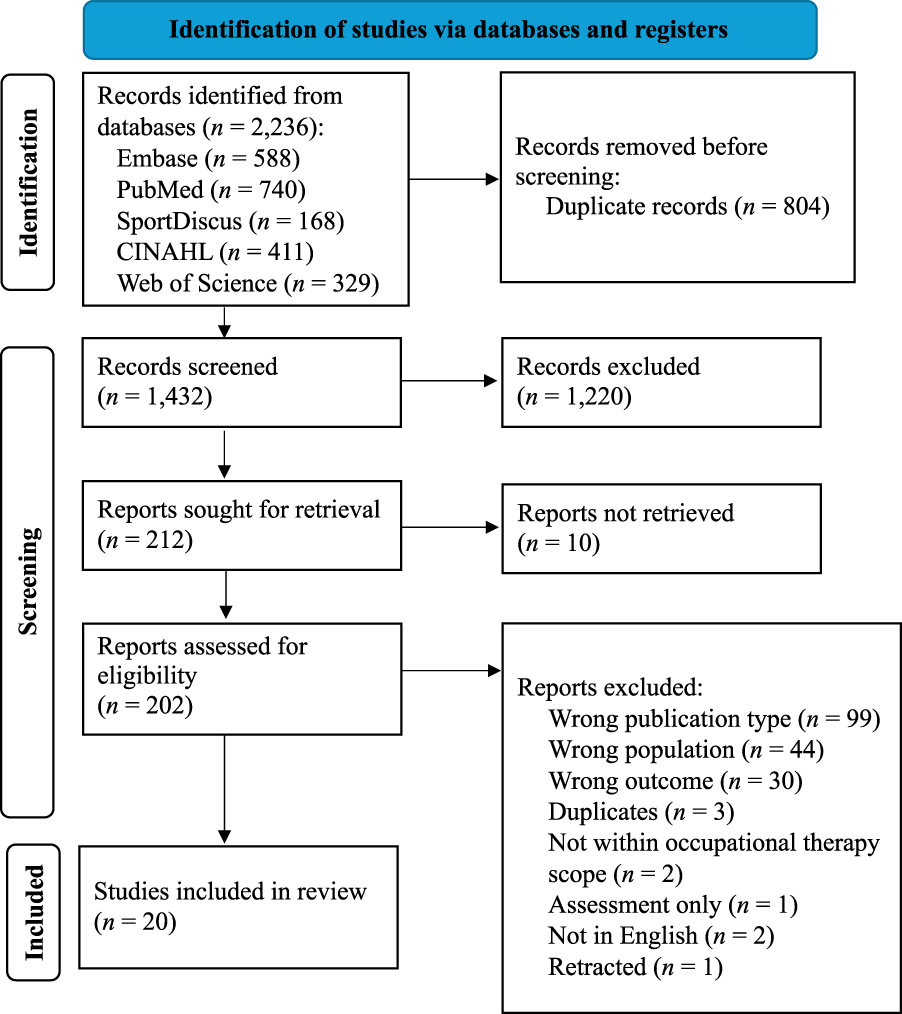
Flow of studies through the systematic review.
Included Studies
The 20 articles included were quantitative and varied in level of evidence and study design. Although we did not exclude qualitative studies, none met the inclusion criteria. Of the 20 articles, 7 were randomized controlled trials (RCTs), 4 had a quasi-experimental design, 3 were case reports, 5 were case series, and 1 had a repeated-measures design. The studies varied in sample size, ranging from 1 to 200 participants. Results from 865 participants between ages 3 and 18 yr who experienced PCCS were analyzed in this systematic review. See Table A.4 in the Supplemental Material for detailed information on each study.
Outcomes Measured
Functional outcomes were of interest to ensure relevance to the field of occupational therapy. Specifically, outcomes measures must have addressed at least one of the following areas of occupation: ADLs, education, play and leisure, social participation, and rest and sleep. Most of the studies used multiple outcome measures to assess functional outcomes, which were largely participant- or parent-report measures. Although slightly more than one-quarter of the studies used symptom-specific report measures such as the Post-Concussion Symptom Inventory and the Post-Concussion Symptom Scale (Gauvin-Lepage et al., 2020; Gunter et al., 2018; Hugentobler et al., 2015; Hunt et al., 2019; Paniccia et al., 2019; Sang et al., 2020), data from these measures were considered only as they related to other functional outcomes. Ultimately, data extraction and synthesis focused on relevant functional outcomes for which data were available in the studies at each assessment time point. Given the variety of assessment measures used across studies, the literature did not identify a gold standard for measuring outcomes.
Six studies used outcome measures to assess general activity participation and function (Gunter et al., 2018; Hugentobler et al., 2015; Paniccia et al., 2019; Renaud et al., 2020; Smith & Layman, 2022; Wright et al., 2020). Although these outcome measures were primarily self-report, Hugentobler et al. (2015) used objective measures, such as the Balance Error Scoring System (BESS). Two studies used various self-report measures to determine whether improvements in education participation had occurred (Rivara et al., 2022; Wright et al., 2020), although Rivara et al. (2022) also used objective measures of grade point average and return-to-school date. Eleven studies used self-report measures to assess participants’ perceived performance in activity (Chrisman et al., 2019; Gagnon et al., 2009; Hunt et al., 2019; Hussey, 2017; Lynch et al., 2015; McCarty et al., 2016, 2021; McNally et al., 2018; Sang et al., 2020; Simpson et al., 2021; Tomfohr-Madsen et al., 2020). The Pediatric Quality of Life Inventory (PedsQL) was the most common standardized assessment used in the included studies; it was used to measure outcomes in 8 of them (Chrisman et al., 2019; Gauvin-Lepage et al., 2020; Gladstone et al., 2019; McCarty et al., 2016, 2021; McNally et al., 2018; Renaud et al., 2020; Simpson et al., 2021). The PedsQL is a patient-reported outcome measure with subsets specific to physical, social, and educational performance. Three studies used other self-reported outcome measures (Adolescent Sleep Wake Scale, Insomnia Severity Index, 24-Hour Sleep Patterns Interview, Dysfunctional Beliefs and Attitudes about Sleep Scale) to specifically assess rest and sleep (McCarty et al., 2021; Smith & Layman, 2022; Tomfohr-Madsen et al., 2020). One study measured self-perceived activity tolerance using the Post-Concussion Symptom Inventory and activity participation using the Physical Activity Questionnaire for Older Children (Gauvin-Lepage et al., 2020), and 1 study measured self-perception of social and educational skill using the Self-Efficacy Questionnaire for Children and physical activity using the Godin Leisure-Time Exercise Questionnaire (Paniccia et al., 2019).
Intervention Type
We organized the results into six intervention categories: active rehabilitation, vision-related interventions, psychoeducation, cognitive–behavioral therapy (CBT), the Cognitive Orientation to daily Occupational Performance (CO-OP), and music therapy. Similar interventions were grouped together on the basis of our knowledge of occupational therapy practice and experience with pediatrics and mTBI and concussion. The authors include Alison Heinekamp, an occupational therapist who is a certified brain injury specialist with 11 yr of pediatric brain injury experience; Natalie Molnar, a student occupational therapist; and three physical therapists (Amy Bailes, with 39 yr of pediatric experience; Jason Hugentobler, with 14 yr of experience working with youth with concussion; and Anne Lennon, with 7 yr experience working with youth with concussion). U.S. Preventive Services Task Force (2018) guidelines were used to rate the strength of the evidence for each intervention category.
Active Rehabilitation
Eight articles provided moderate strength of evidence to support the use of active rehabilitation, which centers on interventions targeted to help resolve PPCS through physical movement. Early work by Gagnon et al. (2009) identified an active rehabilitation approach as counter to the standard treatment at the time, which was resting until the adolescent became asymptomatic. This includes interventions such as aerobic exercise, coordination-specific activity, mental imagery, yoga, and vestibular therapy. Three studies implemented 6 wk of active rehabilitation as an intervention (Chrisman et al., 2019; Gladstone et al., 2019; Sang et al., 2020). In a Level 2b study with low risk of bias, Chrisman et al. (2019) found that parent-reported health-related quality of life was significantly improved in the intervention group (n = 19; M age = 15.5 yr) compared with the control group (n = 11; M age = 15.5 yr), who received a home stretching program, yet scores on the child-reported PedsQL were not significantly affected by the intervention. In a Level 2b study with low risk of bias, Gladstone et al. (2019) showed that scores on the PedsQL increased significantly for the treatment group (n = 12; M age = 15.22 yr), who received subsymptom exacerbation aerobic training, and the control group (n = 14; M age = 15.50), who received 6 wk of stretching. In a Level 2b study with moderate risk of bias, Sang et al. (2020) used the Canadian Occupational Performance Measure to evaluate functional outcomes among 52 youth (M age = 14.42 yr) with postconcussion symptoms. Researchers found clinically significant changes in performance of occupations and satisfaction with occupational performance from pre- to postintervention.
In a Level 4 study with moderate risk of bias, Paniccia et al. (2019) used a case-series design to analyze the effects of mindfulness-based yoga for 6 youth who had concussion symptoms for longer than 4 wk. The intervention included mindfulness meditation approaches and physical yoga postures once per week for 8 wk. Researchers found trends of increased self-efficacy across academic, social, and emotional domains.
A case report (Level 5) with moderate risk of bias described the effects of a return-to-riding protocol for a 14-yr-old female equestrian athlete with a history of concussion (Gunter et al., 2018). A seven-step return-to-riding protocol guided physical therapy intervention strategies (e.g., stability exercises, aerobic activity). The participant completed the full protocol in 8 wk and successfully returned to competition.
The three remaining articles (Gagnon et al., 2009; Gauvin-Lepage et al., 2020; Hugentobler et al., 2015) included coordination exercises, home programming, and vestibular therapy in conjunction with aerobic rehabilitation. In a case series (Level 4) with moderate risk of bias, Gagnon et al. (2009) used the Montreal Children’s Hospital Rehabilitation After Concussion program with 16 youth slow to recover from a concussion. This program acknowledges that the effects of a concussion can be physical, cognitive, emotional, and social, and it is designed to help children recover from concussions through exercise. They found that all youth were able to resume their normal participation in physical activity at the end of the program. In a Level 2b study with moderate risk of bias, Gauvin-Lepage et al. (2020) used intervention (n = 36; M age = 14 yr) and control (n = 13; M age = 13.2 yr) groups to determine the effectiveness of active rehabilitation in improving activity participation, including physical, social, and academic function. Participants in the control group received standard care, which followed the usual rest- and symptom-limited activity-based recommendations and return-to-learn strategies. Youth in the experimental group demonstrated significant improvement in emotional and social functioning domains compared with those in the control group, but no significant differences were found between groups on school and physical functioning domains. A case series (Level 4) with moderate risk of bias investigated the use of active rehabilitation performed with 5 youth with prolonged concussion symptoms (Hugentobler et al., 2015). Three of the five patients had returned to preinjury leisure participation levels 3 to 6 mo after discharge from physical therapy.
Vision-Related Interventions
Two case reports highlighted visual interventions to address oculomotor impairment (Hussey, 2017) and photophobia (Lynch et al., 2015). Although intervention focused on visual symptoms, self-perceived function and return to activity were used as outcome measures. In a Level 5 case report with moderate risk of bias, Hussey (2017) provided vision therapy, including pursuits, saccadic exercises, and hand-directed eye movements, to a 16-yr-old boy who sustained a concussion while trail riding. Thirty-seven vision therapy sessions resulted in improved engagement in leisure activities, including reading and bike riding. In another case report (Level 5) with a low risk of bias, Lynch et al. (2015) described the use of computer gaming glasses to relieve photophobia symptoms for two adolescents who had sustained sports-related concussions with ongoing vision complaints. After the intervention, participants reported improved participation in education and leisure activities. Despite the improvements in functional outcomes in these case reports, the small sample size means that there is low strength of evidence to support the use of vision interventions to improve functional outcomes.
Psychoeducation
Psychoeducation is a strategy used to help individuals better understand and cope with illness. Three studies provide moderate strength of evidence to support the use of psychoeducation as a primary intervention to educate clients on self-management strategies after a concussion. In a Level 3 study with moderate risk of bias, McNally et al. (2018) asked participants (n = 31; M age = 15.9 yr) to attend two to five sessions that addressed ongoing concussion symptoms and their impact on activity participation through psychoeducation, activity and sleep scheduling, relaxation training, and cognitive restructuring. Objective and subjective measures demonstrated clinically significant improvements in participants’ physical, social, emotional, and school performance. In a Level 4 study with moderate risk of bias, Wright et al. (2020) performed a retrospective case review to analyze the effectiveness of speech-language pathology. Psychoeducation was used to address somatic and psychological symptoms among participants (n = 15; M age = 15.7 yr) with the goal of improving education participation. Of the 15 participants, 11 were discharged from services after significant improvements in education participation, as evidenced by an increase in grades, assignment completion, or school attendance.
An RCT (Level 1b) with low risk of bias was performed to determine the effects of psychoeducation on activity participation among youth with concussion symptoms (Renaud et al., 2020). The intervention group (n = 60; M age = 11.5 yr) participated in two sessions of the Brains Ahead! intervention. Psychoeducation focused on the causes, incidence, and possible consequences of concussion; information and advice about returning to activities; and participation, sensory sensitivity, and stress tolerance after mTBI. Total score on the Child and Adolescent Scale of Participation improved significantly in both groups over time from 2 wk to 6 mo postconcussion, with the intervention group reporting more significant changes in total level of activities and participation between 3 and 6 mo. Significant changes in PedsQL scores were also seen in the intervention group. Participants who received the Brains Ahead! intervention reported significantly fewer functional symptoms and improved quality of life at 6 mo postconcussion compared with the control group, who received only a concise information brochure.
CBT Techniques
Three studies generated strong evidence to support the use of CBT techniques for youth with PPCS (McCarty et al., 2016, 2021; Rivara et al., 2022). The studies included topics such as sleep hygiene, coping skills, and relaxation strategies when using CBT techniques.
In an RCT (Level 1b) with low risk of bias, McCarty et al. (2021) used a CBT format to address participants’ concerns, such as pain management, sleep hygiene, emotion regulation, mindfulness, and problem solving. They found that the intervention group (n = 101; M age = 14.7 yr) significantly improved in functional status and sleep quality as a result of CBT intervention compared with the control group (n = 99; M age = 14.7), who received standard care for medical settings. Similarly, in an RCT (Level 1b) with low risk of bias, McCarty et al. (2016) concluded that the intervention group (n = 25; M age = 15 yr) significantly improved in health-related quality of life compared with the control group (n = 24; M age = 15 yr), who received standard care for medical settings.
In an RCT (Level 1b) with low risk of bias, Rivara et al. (2022) focused on educational performance as an outcome measure. The intervention group received CBT that addressed topics based on presenting concerns, such as headaches, fatigue, sleep problems, depressive symptoms, and anxiety symptoms. Results showed that the intervention group (n = 101; M age = 14.7 yr) showed a reduction in school absences compared with the control group (n = 99; M age = 14.7), who received nonstandardized usual care inclusive of the use of sports medicine, rehabilitation medicine, physical therapy, primary care, specialty mental health services, emergency departments, and referrals to other specialty providers as needed. No significant differences were found between groups in other areas of academic function assessed.
In a Level 3b study with moderate risk of bias, Simpson et al. (2021) researched the effectiveness of the Concussion Symptom Treatment and Education Program with 30 youth experiencing ongoing concussion symptoms and functional impairments. The program consisted of six CBT-based treatment sessions involving psychoeducation, sleep hygiene, relaxation training, and cognitive errors and restructuring. Significant improvements were seen in school attendance, sleep-onset time, and number of days per week in which participants engaged in physical exercise.
In a Level 2b study with low risk of bias, Tomfohr-Madsen et al. (2020) compared the effects of CBT for insomnia (CBT–I) with those of usual care in improving commonly experienced sleep complications after concussion. This RCT used six weekly sessions of CBT–I with 12 youth experiencing insomnia symptoms after a concussion (M age = 15.2 yr). The sessions included relaxation strategies, stimulus control, sleep hygiene, cognitive restructuring, and mindfulness techniques. Participants demonstrated clinically significant improvements in insomnia ratings after the intervention that were maintained at 4-wk follow-up. Clinically significant improved sleep quality, fewer dysfunctional beliefs about sleep, better sleep efficiency, shorter sleep-onset latency, and longer sleep time were reported in the intervention group compared with the control group (n = 12; M age = 14.9 yr), who received treatment as usual.
CO-OP Approach
In a Level 4 case series with moderate risk of bias, Hunt et al. (2019) used the Canadian Occupational Performance Measure to set individualized goals and measure outcomes for youth (n = 3 girls, ages 15–17 yr) with persistent postconcussion symptoms. The participants identified goals related to school, leisure, and health and wellness (e.g., using a sleep routine). Ten sessions were executed over a 7-wk period during which participants worked toward their goals using the CO-OP. Each session began with a review of metacognitive strategies and the progress made toward individualized goals. Clinically significant changes in performance and satisfaction ratings on individualized goals were reported for all participants postintervention. Changes were maintained for all participants at 3-mo follow-up. Despite improvements in performance, the small sample size means there is low strength of evidence to support use of the CO-OP approach with youth with PPCS.
Music Therapy
There is low strength of evidence to support using music therapy as an intervention to improve functional outcomes among youth who are slow to recover from a concussion. One Level 4 study with moderate risk of bias analyzed the effects of using music therapy with preferred music with an 18-yr-old athlete who had a history of concussions and subsequent sleep difficulties (Smith & Layman, 2022). Eleven music therapy sessions were led by a music therapy student. In the sessions, the participant was asked to listen to music with relaxation strategies before bed, including breathing techniques, imagery, and mindfulness. The participant demonstrated an increase in sleep quality on outcome measures after completing the intervention.
Discussion
This review examined the evidence related to interventions that address the occupational needs of youth with PPCS, including ADLs, education, play and leisure, social participation, and rest and sleep. Strong evidence supports the use of CBT and moderate strength of evidence supports the use of psychoeducation and active rehabilitation to improve occupational performance among youth with PPCS. Occupational therapists are qualified to incorporate CBT strategies, psychoeducation, and active rehabilitation into the treatment of PPCS; however, only 3 of the included studies used an occupational therapist to deliver interventions. CBT strategies can be used to address client factors and performance patterns, including higher-level cognition, habits, and routines (AOTA, 2020). Psychoeducation is within the scope of occupational therapy practice and may be used by occupational therapists to target performance patterns through education, which is defined in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020, p. 76) as imparting “knowledge and information about occupation, health, well-being, and participation, resulting in acquisition by the client of helpful behaviors, habits, and routines that may or may not require application at the time of the intervention session.” Active rehabilitation can be used to improve occupational performance and quality of life by addressing performance skills through goal-directed leisure activity.
In the review process, 30 intervention studies within the scope of occupational therapy were excluded because they used only symptom-focused outcome measures. Occupational therapists use an occupation-based approach to focus on occupational performance, rather than focusing solely on symptom resolution as an outcome, which would make them a uniquely important addition to the multidisciplinary team. There is evidence that noninjury factors (e.g., maladaptive coping, premorbid anxiety, symptom exaggeration or feigning) among youth after concussion account for more severe symptomatology and increased disruption to quality of life when symptoms persist for weeks to months (Kirkwood et al., 2021), suggesting that overfocusing on symptoms alone can be detrimental to recovery for these individuals. Kirkwood et al. (2021) suggested that more is not always better and recommended that strategies other than medical management be used for symptom management, such as sleep hygiene, psychoeducation, psychological support, short-term educational supports, and participation in social and leisure activities, all of which are within the scope of occupational therapy. Occupational therapy collaboration with other disciplines, such as psychology, could greatly improve the multidisciplinary care received by youth with PPCS and should be considered for future study.
The CO-OP is an occupation-based intervention included in this review that has promising results but a limited body of evidence. More high-level studies are needed to strengthen the evidence for the use of this intervention. Clinical recommendations related to vision interventions and music therapy cannot be made because of the limited number of high-level studies.
When little evidence exists, single-case experimental designs and practice-based evidence can be useful in the early development of research on specific interventions (Krasny-Pacini & Evans, 2018). Such development can make use of the small-scale research routinely done in rehabilitation centers, hospitals, and private practices by rehabilitation students and professionals and offers an opportunity to conduct high-level research with a limited number of patients (Krasny-Pacini & Evans, 2018). Occupational therapists could consider these study designs to build a greater body of evidence and move the field forward in its rehabilitative role with youth with PPCS.
With a limited body of evidence and no formal guidelines for the treatment of PPCS among youth, it is no wonder that decreased knowledge of and confidence in concussion management may be a barrier to occupational therapy involvement in concussion care (Salisbury et al., 2017). This emphasizes the need for occupational therapy education to include PPCS in the general curriculum. Additionally, it is important that continuing education opportunities for occupational therapists are readily available to stay abreast of the most recent research and evidence-based recommendations.
Limitations
Some limitations should be considered when interpreting the results of this review. Of the 20 studies included in the analysis, 9 were considered as providing low-level evidence. Overall, there is a lack of high-level literature pertaining to effective interventions to improve occupational performance among people with PPCS. The included studies used a wide variety of outcome measures, and the synthesis of congruent results is challenging, with minimal overlap of outcome measures. Additionally, authors of the included studies defined PPCS differently. For example, some studies included participants who were 2 wk beyond the initial concussion, and other studies included participants who were up to 2 yr beyond the initial injury. Discrepancies in the definition of PPCS reflect the current literature available on concussion and may limit the analysis of findings. The wide range of sample sizes in the included studies (1–200) may be another limitation of this research. Of the 20 studies, 7 had sample sizes smaller than 10, which significantly limits the generalizability of results. Finally, much of concussion research continues to focus on sports-related concussions, and as a result many of the studies in this analysis were specific to sports. Future research should focus on other areas of occupation and other mechanisms of injury to better generalize results to the pediatric population.
Implications for Occupational Therapy Practice
Youth with PPCS experience disruption in many occupations and could benefit from occupational therapy intervention. The findings of this systematic review have the following implications for occupational therapy practice: ▪ Occupational therapists need to be knowledgeable about PPCS management strategies to better establish their role in working with this population. Concussion education should be included in the general occupational therapy curriculum, and continuing education should be made readily available. ▪ CBT strategies should be considered when working with youth with PPCS, especially if they are having difficulty with education participation or rest and sleep. ▪ Psychoeducation and active rehabilitation could be used by occupational therapists as clinically appropriate to improve functional outcomes and overall quality of life for youth with PPCS. ▪ Occupational therapists have a unique role in PPCS recovery because they prioritize functional outcomes over symptom resolution for youth with persistent symptoms. They should prioritize the use of outcome measures that focus on occupational performance. ▪ Occupational therapists should consider the use of practice-based evidence and single-case experimental designs to build a greater body of evidence that could move the field forward in the rehabilitative care of youth with PPCS.
Implications for Future Research
Although many occupational therapists agree that occupational therapy could play an important role in the rehabilitation of individuals with PPCS, little evidence exists related specifically to occupational therapy intervention. More robust intervention studies with larger sample sizes and consistent functional outcome measures are needed to effectively establish the role of occupational therapy in PPCS management.
Conclusion
The findings of this review support the role of occupational therapy for youth with PPCS in using evidence-based interventions to improve occupational performance. Specifically, evidence supports the use of CBT strategies to improve education participation and rest and sleep, active rehabilitation to facilitate return to activity and improve quality of life after a concussion, and provision of psychoeducation to increase self-management and participation in daily activity. Studies with rigorous designs are needed to evaluate the effectiveness of therapeutic interventions and to further support the role of occupational therapy in the treatment of youth with PPCS.
Supplemental Material
Supplementary material for Interventions to Improve the Occupational Performance of Youth With Persistent Postconcussion Symptoms: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050642.pdf for Interventions to Improve the Occupational Performance of Youth With Persistent Postconcussion Symptoms: A Systematic Review by Alison Heinekamp, Natalie Molnar, Anne Lennon, Amy Bailes, Jason Hugentobler and Melissa Previtera in The American Journal of Occupational Therapy
Footnotes
*Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.