
Abstract
This systematic review highlights occupational therapy’s distinct value and role in the rehabilitation of adults with low vision.
Before the late 1990s, few occupational therapy practitioners worked in the field of low vision. At the turn of the century, changes in access to reimbursement from Medicare, the federally funded program for older Americans, opened the door for occupational therapy to the rehabilitation of adults with a primary diagnosis of low vision (Centers for Medicare and Medicaid Services, 2002). Around the same time, the American Occupational Therapy Association (AOTA) developed a specialty certification for practitioners seeking to demonstrate competencies in this field (Warren et al., 2006).
Low vision therapists, vision rehabilitation therapists, and orientation and mobility specialists are professionals who provide rehabilitation services to adults with low vision. Additionally, many state agencies provide training to personnel for state-sponsored programs (e.g., vocational rehabilitation and independent living). These personnel provide rehabilitative services to adults and older adults with low vision at training centers or in their homes. Although occupational therapy is relatively new to the arena of service providers for adults with low vision in the United States, only occupational therapy practitioners are recognized by Medicare and other commercial health insurers as approved health care providers. However, legislative efforts over the past two decades to recognize low vision therapists, vision rehabilitation therapists, and orientation and mobility specialists as health care providers have the potential to threaten occupational therapy practitioners’ role in the health care system (Gerritsen, 2007).
Generation of Evidence for Occupational Therapy Interventions
As the profession of occupational therapy has matured, practitioners have become responsible for applying theories to generate evidence to support its practice (Mosey, 1993). In general, occupational therapy theories describe occupational function, occupational dysfunction, and methods to create change (Ikiugu, 2012). Theories are used to explain and predict outcomes of the occupational therapy process and therefore to guide the selection of interventions (Ikiugu & Smallfield, 2015). The Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020) repeatedly emphasizes that occupational therapy practitioners should use theories to guide professional reasoning throughout the occupational therapy process.
The outcomes of interventions can confirm or refute theoretical hypotheses, thereby testing the validity of the theory and contributing to the profession’s body of evidence. Ikiugu et al. (2009) suggested that theory-driven practice enabled practitioners to “rightfully call themselves professionals” (p. 162). Theories provide hypotheses for change, whereas practice guidelines can be thought of as the methods to achieve outcomes—inputs that yield outputs—otherwise known as postulates for change (Brazil et al., 2005 ; Cole & Tufano, 2020; Kramer et al., 2019). Theory-driven practice and evidence-based practice guidelines are complementary and synergistic (Brazil et al., 2005; Vanderplasschen & Maeyer, 2014) and should be used together. The danger of atheoretical occupational therapy practice is that evidence-based guidelines can be mechanistically applied without professional reasoning, resulting in the occupational therapy practitioner not understanding why interventions did or did not work. Even when desired outcomes are achieved through application of evidence-based practice guidelines alone, the profession runs the risk of losing its distinct value and scope of practice. If practitioners do not use theories to guide interventions, are they professionals or merely technicians? Technicians follow a script or select from a checklist (Nash & Mitchell, 2017). Occupational therapy practitioners are expected to demonstrate their expertise and distinct value and distinguish themselves from others by using theory to think about clients’ situations and develop a plan of care (AOTA, 2020; Kielhofner, 2009).
Recent calls to action to promote the distinct value of occupational therapy offered strategies for implementing knowledge translation to promote value-based care (Arbesman et al., 2014; Juckett et al., 2021). The term distinct value appears to relate to the economic benefit of occupational therapy rather than its ideological view of well-being through engagement in occupation. Neither touches on application of theories to distinguish the occupational therapy profession from others providing similar interventions.
To meet AOTA’s Vision 2025 (AOTA, 2017), occupational therapy practitioners in the United States have increasingly been engaged in the generation of evidence to support interventions for adults with low vision. In 2020, AOTA published the third edition of its Practice Guidelines for Adults With Low Vision. These guidelines are meant, among other things, to “justify occupational therapy services to external stakeholders” (Kaldenberg & Smallfield, 2020, p. 1).
We contend that to justify occupational therapy services to all stakeholders, practitioners need to demonstrate their unique contribution among the many service providers to adults with low vision. Interventions in occupational therapy for adults with low vision bear similarities to methods used by low vision therapists, vision rehabilitation therapists, and personnel working for state agencies (Academy for Certification of Vision Rehabilitation and Education Professionals, 2021; Tennessee Department of Human Services, n.d.).
In this article, we use the word theory to denote occupational therapy theories, frameworks, and conceptual models. Alterio (2018) noted that clinicians rarely apply theories to guide intervention choices, warning that without a sound epistemological basis for decision-making, the profession could lose its credibility. Hence, we believe that theories, coupled with evidence-based guidelines, are critical in justifying occupational therapy services to adults with low vision, particularly when other professionals, such as low vision therapists, orientation and mobility specialists, and vision rehabilitation therapists, use similar, if not identical, interventions.
The purpose of our study was to explore published articles to determine (1) whether theories were recommended or used to guide occupational therapy interventions for adults with low vision and (2) the level of evidence of the publication.
Method
We conducted a quantitative, summative content analysis (Christie, 2007) of any type of publication on occupational therapy interventions with adults with low vision. These included recommended theories, results of studies, personal reflections, and case studies. The publications represented all levels of evidence from the past half-century. Peer-reviewed and non– peer-reviewed publications were included.
Search Strategy
Searches were performed in November 2021 in online research databases using relevant terms, yielding a total of 1,318 results (CINAHL = 304, Scopus = 363, PubMed = 207, Embase = 444). After duplicates were removed, 592 unique records were identified. Article abstracts were independently screened by Orli Weisser-Pike and Lauren Woods to determine applicability to the current project. Disagreements were resolved until consensus was reached. Our independent screening of these records resulted in 186 articles on interventions for people with low vision. One hundred eighty-five articles were retrieved; 1 was unavailable through interlibrary loan. See Figure 1.
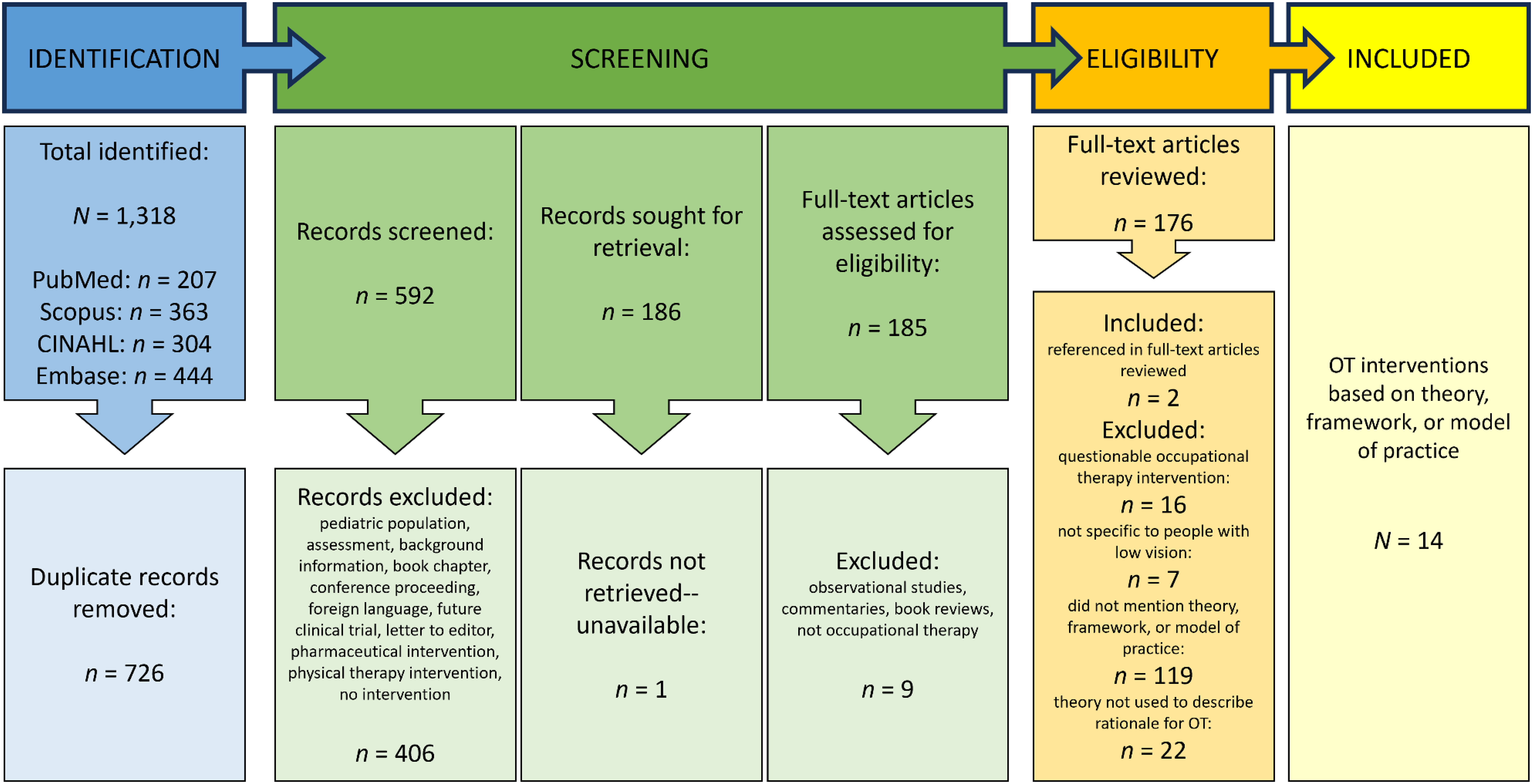
Flow of studies through the systematic review process.
Inclusion and Exclusion Criteria
We included all English-language published materials that mentioned occupational therapy for adults with low vision. Conference proceedings abstracts, book reviews, guest editorials, and commentaries were excluded because of their incomplete nature. We also excluded dissertations, books, and book chapters because we felt they were not as accessible to practitioners as journal-based publications. Articles about occupational therapy with children younger than age 18 yr were excluded because specialty certification in low vision offered by AOTA—and the resulting evidence to support its practice—is focused on adults. Descriptive articles about conditions or the impact of vision loss were also excluded. After a secondary screening of the 185 retrieved articles, 9 additional records were rejected because they did not meet inclusion criteria. The resulting 176 full-text articles formed the basis of our content analysis.
Data Extraction
Three occupational therapy clinician-educators (Weisser-Pike, who has more than two decades of expertise in low vision rehabilitation; Woods; and Pamela Lewis-Kipkulei, who has advanced certification in low vision rehabilitation) and an occupational therapy student, Raegan Avrit, performed the data extraction.
In the first phase of data extraction, all 176 full-text articles were independently examined to answer the following questions: Was the article about occupational therapy interventions? Were the occupational therapy interventions specific to people with low vision? Did the article suggest or mention a theory? Did the theory recommend or guide the selected occupational therapy interventions?
In the second phase of data extraction, Weisser-Pike, Woods, and Lewis-Kipkulei met to answer each question and to achieve consensus on the articles selected.
Of the 176 articles that mentioned occupational therapy, 16 were rejected for a lack of clarity on the specific inclusion of occupational therapy, resulting in 160 articles for further analysis. The second question was asked to ensure that the theory, framework, or conceptual model mentioned was relevant to adults with low vision rather than another primary condition. Seven articles were rejected because they were not specific to adults with low vision. Next, word and partial-word searches were performed on the articles to search for the mention of a theory, framework, or conceptual model. Of 153 articles, 34 met the criteria. The eligible 34 full-text articles were examined in depth to determine whether they provided a rationale for occupational therapy interventions. Two articles that mentioned theories discussed elsewhere and were not found in our original search were retrieved and examined for eligibility on the basis of the previous criteria. In some instances, authors used the word model to illustrate a process rather than a theory and framework to describe a treatment protocol. Several articles mentioned approaches such as rehabilitative, holistic, and client-centered but did not distinguish occupational therapy practice beyond those descriptors. We rejected these articles. Articles that listed theories to guide interventions without explaining why occupational therapy practitioners should use them were also excluded from the analysis. We eliminated 22 articles, leaving 14 for this review.
Determination of Level of Evidence
Using the Evidence Based Practice Toolkit (Winona State University, 2023), each of us independently categorized the resulting 14 articles by level of evidence (for definitions of the levels of evidence, see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot), and consensus was reached regarding each one through discussion.
Results
Our analysis yielded 14 articles about theories to support occupational therapy interventions for adults with low vision (see Table A.2 in the Supplemental Material). Eleven articles reported on interventions guided by a theory, and 3 articles suggested a theory to guide interventions for adults with low vision.
Six of the theories were specific to the practice of occupational therapy (Ecology of Human Performance, Hierarchy of Visual Perception, Model of Human Occupation, Occupational Adaptation model, Person–Environment–Occupation model, and Person–Environment–Occupation–Performance model), two were from other disciplines (Gibson’s Theory of Affordance, Health Belief model), and one merged an occupational therapy theory with a business leadership theory (Occupational Leadership).
One article provided evidence from a well-designed single mixed-methods intervention study (Level 3), 1 provided evidence from a well-designed cohort study (Level 4), 5 provided evidence from single descriptive or qualitative studies (Level 6), and 7 provided evidence from the opinions of experts in the field (Level 7). Eleven of the articles were published in peer-reviewed journals; of these, 7 appeared in occupational therapy publications.
Interventions Guided by Theory
Ecology of Human Performance
One article based on the Ecology of Human Performance focused on interventions for caregivers of people with low vision. Weisser-Pike (2013) demonstrated that caregivers who were provided with specific knowledge and skills reported increased competence in their caregiving role. This Level 7 non–peer- reviewed article was published in an occupational therapy magazine.
Gibson’s Theory of Affordance
In a study of a patient with cortical blindness, Yuen (1993) described a successful intervention based on Gibson’s Theory of Affordance, in which the patient was provided with a tactile template that improved their ability to complete a project. This Level 6 study was published in a peer-reviewed occupational therapy journal.
Health Belief Model
Dahlin-Ivanoff et al. (1998) designed a group intervention for people with vision loss from macular degeneration. The program was based on the Health Belief model, which postulates that when elderly people participate in the design and planning of health-related activities, they achieve better outcomes, such as taking beneficial health-related actions. This Level 6 qualitative study was published in a peer-reviewed counseling journal.
Building on their previous study, Dahlin Ivanoff et al. (2002) compared two groups of people with macular degeneration receiving interventions: One group received usual care (education and training in the use of optical devices), and the other participated in the weekly health education group. The health education group received training in using problem-solving strategies. Significant differences were found between groups, with the latter demonstrating increased perceived security in carrying out health-related occupations. This Level 4 cohort study was published in a peer-reviewed occupational therapy journal.
Continuing their investigations of the two groups, Eklund and Ivanoff (2006) compared the perceptions of group participants in a mixed-methods study. They found that people in the health education group had better acceptance of macular degeneration than those in the group receiving usual care. They also had increased self-efficacy and belief in their ability to carry out activities of daily living. This Level 3 study was published in a peer-reviewed occupational therapy journal.
Hierarchy of Visual Perception
The Hierarchy of Visual Perception formed the theoretical basis for a study by Turton et al. (2015) of a community occupational therapist’s interventions to improve visual scanning among five patients who had visual field losses and spatial neglect from stroke. Interventions were based on principles of the model. This Level 6 peer-reviewed study was published in an occupational therapy journal.
Blanchard et al. (2016) conducted a survey to determine the most common interventions that occupational therapists performed with people who had visual impairments or low vision resulting from brain injuries. They categorized the interventions on the basis of the principles of the Hierarchy of Visual Perception. This Level 6 peer-reviewed study was published in a journal on the topic of vision.
Model of Human Occupation
Du Toit (2008) applied the Model of Human Occupation to empower adults with low vision and blindness who had experienced occupational deprivation. Interventions followed the stages of occupational change as outlined in the model. This Level 7 peer-reviewed article was published in an occupational therapy journal.
Occupational Adaptation
An article by Perea et al. (2018) described interventions for people with vision problems after acquired brain injury with a specific emphasis on interventions that can be carried out in the community. The recommended interventions were intended to assist them in adjusting to vision loss and optimize community engagement. This Level 7 non–peer-reviewed article was published in an occupational therapy magazine.
Person–Environment–Occupation Model
Based on the Person–Environment–Occupation model, Broussard (2019) studied the responses of occupational therapy practitioners to a survey that was then used to develop a tool kit of items to modify the home environment. The Level 6 peer-reviewed study was published in a journal focused on activities in the older adult population.
The Person–Environment–Occupation model guided interventions in all three domains in a case study of a person with low vision reported by Perea and Anise (2019). This non–peer-reviewed Level 7 article was published in an occupational therapy quarterly newsletter.
Theories to Guide Interventions
Hierarchy of Visual Perception
Drawing from the field of neuroplasticity, Warren (1993) described the sequential development of visual skills based on the foundations of visual acuity, visual fields, and oculomotor control. All subsequent visual skills, with the pinnacle being visually guided interaction with the environment, are subservient to the underlying ones. Three principles should guide occupational therapy interventions: (1) Remediate and maximize foundational visual skills, (2) increase the patient’s awareness of the deficit, and (3) compensate for the deficit. Occupational therapy interventions, both remedial and compensatory, need to follow the same sequential hierarchy to achieve occupational performance. The Level 7 peer-reviewed article was published in an occupational therapy journal.
Occupational Leadership
By combining a management model, Situational Leadership, with the Occupational Adaptation model, Nastasi (2015) proposed Occupational Leadership, which is intended to guide health care practitioners— not just occupational therapy practitioners—in promoting occupational engagement by providing the correct level of supervision of older adults with low vision, starting in the home environment and progressing into the community. This Level 7 peer-reviewed article was published in a journal focused on gerontology.
Person–Environment–Occupation–Performance Model
Schoessow (2010) suggested a battery of assessments and interventions for adults with low vision based on the Person–Environment–Occupation–Performance model. This Level 7 peer-reviewed article was published in an occupational therapy journal.
Summary of Findings
Seven of the 14 articles were research studies in which a theory guided intervention, providing evidence for the validity of the theories on which they were based. Three tested two occupational therapy theories: the Hierarchy of Visual Perception and the Person– Environment–Occupation model. The remaining 4 research studies tested two theories from other fields of study. Four of the seven research studies were published in occupational therapy journals.
Of the 7 articles that provided Level 7 evidence for interventions guided by applied theories, 4 were peer-reviewed; however, 3 were published in occupational therapy journals and 1 was published in a gerontology journal. Of the 3 publications suggesting theories to guide interventions, only one theory, the Hierarchy of Visual Perception, was used to guide interventions in 2 studies.
Discussion
The purpose of this systematic review was to explore how theory has been used to structure and guide occupational therapy interventions for adults with low vision. We also assessed the level of evidence. Our results demonstrate that a clearly articulated distinct professional contribution from occupational therapy is lacking in the rehabilitation of adults with low vision. The paucity of information on theory-driven occupational therapy interventions for adults with low vision is alarming. For example, neither of the intervention studies we found were included in the Occupational Therapy Practice Guidelines for Older Adults with Low Vision (Kaldenberg & Smallfield, 2020). The reasons likely include differences in the purposes and search strategies of each study.
Moreover, many, but not all, of the evidence-based interventions recommended in the Practice Guidelines were derived from studies carried out by professionals outside of occupational therapy (e.g., interventions to support reading technologies by using video magnifiers, portable optical character recognition devices, or digital readers or interventions for visual skills training in patients with central visual field impairment). These interventions can be implemented by other professionals in low vision rehabilitation, not just occupational therapy practitioners, further obscuring occupational therapy’s distinct professional contribution. As Alterio (2018) suggested, the lack of theory to drive clinical decision-making in the selection of occupational therapy interventions is dangerous, because deciding on evidence-based interventions without a basis in theory can appear arbitrary and devoid of context—and can be viewed as a cookbook approach. Atheoretical application of interventions can result in failure to identify the reasons why interventions are or are not successful (Brazil et al., 2005). Although the Practice Guidelines clearly instruct occupational therapy practitioners to base interventions on sound clinical reasoning, the general absence from the literature of examples of application of theories to guide such clinical reasoning only serves to erode occupational therapy’s distinct professional identity. Articles we found in our analysis can serve as models for the infusion of theories to direct the occupational therapy process, including the selection of evidence-based interventions. Occupational therapy interventions for adults with low vision should be guided by theory that provides a rationale for occupational therapy clinical decision-making. Application of theories to guide interventions should be used at the beginning of the occupational therapy process. Without theories to guide practice, practitioners function as technicians rather than clinicians.
The fact that 4 of the 14 articles we found were published in journals outside the occupational therapy profession is even more troubling. We believe that evidence for occupational therapy interventions should be published in occupational therapy journals. Furthermore, we recommend that publishers of occupational therapy evidence insist that authors include application of theory before accepting manuscripts for publication.
Limitations
Our analysis was limited to occupational therapy interventions in low vision rehabilitation. We recognize that in our search we may have missed publications on occupational therapy interventions for adults with low vision that included theories.
Implications for Occupational Therapy Practice
On the basis of this systematic review, we believe that all occupational therapy practitioners have an opportunity to highlight the distinct value of the profession. This review has the following implications for occupational therapy practice: ▪ Occupational therapy educators teaching about low vision should articulate the theoretical underpinnings that guide assessments and interventions. ▪ Occupational therapy clinicians working with adults with low vision should articulate to referral sources and relevant others the theoretical basis for interventions. ▪ Occupational therapy researchers should test theories to provide evidence for occupational therapy interventions for adults with low vision.
Conclusion
The future growth of the profession of occupational therapy is contingent on practitioners’ ability to articulate the rationale behind the selection of evidence to support practice (Nash & Mitchell, 2017). Even though much evidence for occupational therapy interventions with adults with low vision has been published over the past few decades, we contend that the evidence is not enough because it does not distinguish occupational therapy from other professions in low vision rehabilitation. We believe that the missing ingredient in much of the available evidence is the application of occupational therapy theories. We propose that the application of theories to guide interventions distinguishes occupational therapy from similar professions in low vision rehabilitation and yields unique outcomes. Theories should be applied at the outset of the occupational therapy process, not as an afterthought. These theories should continue to be tested in research studies to provide further evidence for the uniqueness of occupational therapy outcomes.
Although our research was limited to the area of occupational therapy low vision interventions, we suspect, based on our limited findings, that our results could be replicated in other areas. We therefore urge occupational therapy practitioners to apply theoretical constructs systematically and consistently to the occupational therapy process in all fields of occupational therapy, to grow the body of evidence and help our profession reinforce its unique identity and distinct value. We contend that by integrating theories into evidence-based research and practice, occupational therapy will gain a higher distinctive profile as a mature profession.
Supplemental Material
Supplementary material for Theory Is Essential in Promoting the Distinct Value of Occupational Therapy in Rehabilitation of Adults With Low Vision: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050655.pdf for Theory Is Essential in Promoting the Distinct Value of Occupational Therapy in Rehabilitation of Adults With Low Vision: A Systematic Review by Orli Weisser-Pike, Lauren Woods, Pamela Lewis-Kipkulei and Raegan Avrit in The American Journal of Occupational Therapy
Footnotes
*
Indicates articles included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.