
Abstract
This is the first study to use an occupational lens to examine how adolescents share their responsibility for managing their Type 1 diabetes in secondary school.
Type 1 diabetes (T1D) is an autoimmune disorder, with the peak age of diagnosis being ages 12–14 yr (Katsarou et al., 2017). The global incidence of T1D is predicted to double by 2040 (Gregory et al., 2022). Poorly managed T1D is associated with increased morbidity and mortality relating to complications such as neuropathy, renal disease, and cardiovascular disease (Katsarou et al., 2017). Most adolescents are not meeting the metabolic targets associated with better long-term outcomes (Hannon et al., 2018). Adolescents with T1D also have an increased risk of concomitant mental health disorders and are less likely to finish school and to maintain employment (Fletcher & Richards, 2012; Gregory et al., 2022). There is therefore an increasing need for health professionals to develop responsive services for adolescents.
T1D is managed within the overall paradigm of self-management, which is defined as having responsibility for diabetes care, including emotional, role, and medical management (Keddy et al., 2021; Strand et al., 2019). An occupational analysis of diabetes self-management (DSM) has found it to be complex and composed of multiple activities (e.g., medication administration; monitoring of blood glucose, diet, and activity; arrangement of support) that require integration into activities of daily living (Youngson, 2019). Occupational therapists are uniquely situated to understand the impact of this kind of intricate regimen on the roles, habits, and routines of adolescents and their families (Epley et al., 2021).
In the context of families, sharing responsibilities for T1D management is associated with better outcomes and has been described as a flexible process wherein parents are constantly responsive to fluctuating adolescent needs (Gardener et al., 2022). This aligns with the occupational therapy definition of co-occupation as mutual engagement in occupation whereby one participant influences the other’s actions (Pizur-Barnekow & Pickens, 2019). A scoping review determined that better outcomes are associated with responsibility-sharing that is driven by clear, autonomy-supportive, team-based negotiation of responsibilities, to enable mutually agreeable allocation of task ownership (Gardener et al., 2022).
Minimal attention has been given to how this kind of cooperation, or sharing of responsibilities, functions in the school environment. Adolescents spend 6–8 hr/day at school and perform a greater number of diabetes care tasks independently in that environment, compared with diabetes care tasks that are performed at home (Aalders et al., 2021). A large population study of Welsh schoolchildren found that academic disadvantages secondary to T1D were mitigated through better metabolic control (French et al., 2022). Students with the poorest metabolic control evidenced a lower level of educational attainment on completion of their schooling compared with their nondiabetic peers, and those with optimal metabolic control outperformed their nondiabetic peers. These findings suggest that there may be important advantages to improving school-based support for diabetes management.
In this article, we report on the second phase of a mixed-methods sequential explanatory investigation into school-based responsibility for diabetes management. The first phase, a cross-sectional survey of 60 Australian adolescents and their parents, revealed a fundamental lack of inclusion of adolescents in processes central to the management of responsibility at school and discordant parent–adolescent perceptions of relative involvement (Gardener et al., 2023). Although an individualized school diabetes plan is widely recommended as key to the negotiation of school responsibilities and management of environmental barriers (Edwards et al., 2014; Lawrence et al., 2022), more than one-third of the adolescents surveyed in the first phase reported not having a school plan. Most reported never having been to a school meeting, and more than one in three had no communication with health care providers or school staff about their diabetes care. In addition, in contrast to expectations of increasing adolescent responsibility across the school years (Saxby et al., 2020), the survey revealed a lack of expanding adolescent involvement in the determination of school-based diabetes management. These findings are congruent with those of an Irish cross-sectional study that reported a lack of school plan use and limited involvement of older adolescents in school diabetes management processes (McCollum & O’Grady, 2020).
In this qualitative study, we aimed to further explore these issues in relation to the management of T1D responsibility in secondary schools; specifically, we focused on four research questions: What do adolescents perceive the tasks involved in DSM at school to be? How do adolescents understand responsibility for DSM to be arranged for school? How do adolescents experience the sharing of their own responsibility for school-based DSM? What impact do adolescents perceive DSM has on school participation?
Method
Research Design and Procedure
This qualitative study rests on a pragmatic worldview (Creswell, 2014) and is the second phase of a mixed-methods study with a sequential explanatory design. It received ethics approval from the Human Research Ethics Committee of Children’s Health Queensland (LNR/18/QCHC/46374). Use of reflexive thematic analysis (Braun & Clarke, 2022) enabled both a descriptive and interpretative analysis of adolescents’ perspectives of responsibility-sharing through the identification of patterns of commonality in the data. We followed the Consolidated Criteria for Reporting Qualitative Research guidelines (Tong et al., 2007) when reporting the qualitative methodology.
Participants were identified by a diabetes educator working in the endocrinology clinic of a major metropolitan hospital in Australia. Purposive sampling included adolescents with T1D who had diverse treatment regimens and schooling types and met the inclusion criteria: age 15 or 16 yr, attending a mainstream high school, and with no concomitant disability. The diabetes educator sought parents’ consent to be contacted by phone by Lisa Gardener, who explained the study and invited parental consent for their adolescent’s involvement. Adolescents were then contacted directly for their assent to participate.
Participants
Eleven adolescents (all Caucasian, with six identifying as female and five as male), representing a mix of diabetes regimens (insulin pump, multiple daily injections, and/or continuous glucose monitor) and schooling types, participated (Table 1).
Participant Demographics
Note. All participant names are pseudonyms. CGM = continuous glucose monitor; MDI = multiple daily injections.
Data Collection
Semistructured interviews of 45–75 min duration were conducted via participants’ choice of phone call, Zoom, or in person (see Appendix). Interviews were audio recorded. Recordings were transcribed verbatim and deidentified, and then transcripts were compared with recordings to ascertain accuracy. Recruitment continued until the research team, through constant comparison of data during collection, agreed that a point of substantial information power (Malterud et al., 2016) had been reached. This was determined by data that sufficiently addressed the research questions, given the focus on identifying pragmatic issues relating to self-management, the homogeneous participant sample, and high-quality dialogues with participants.
Data Analysis
Lisa Gardener undertook all data collection. The coauthors who collaborated in the analysis were female academic occupational therapists with doctoral qualifications and extensive experience in qualitative research. Two authors have lived experience of parenting adolescents with T1D attending school. After the first five interviews, Lisa Gardener and Helen Bourke-Taylor engaged in collaborative first-round coding, and then Lisa Gardener analyzed all transcripts using NVivo (Version 12). Throughout the analysis, she continued an iterative cycle of coding and reflection and met regularly with all of the coauthors to discuss assumptions that were possibly influencing this process and to clarify the identification of meaningful themes.
Trustworthiness was enhanced through methodological triangulation by integrating the insights gained from the cross-sectional survey analysis into the analysis of qualitative data. Credibility was further supported by having two researchers independently code the initial data set and holding ongoing peer debriefings in addition to research team meetings. Dependability of findings was strengthened by recording the evolving analysis, through both collation of the NVivo-supported analyses (e.g., mind maps) and team meeting documentation. To enhance confirmability of the data, Lisa Gardener reflexively journaled her observations, assumptions, and decision-making throughout. Transferability was considered through the provision of thick descriptions of the research process and findings (Nowell et al., 2017).
Results
Adolescents described the occupation of DSM at school as complex and composed of multiple activities. These activities were dominated by parent and adolescent involvement (Table 2). Three themes and eight subthemes were identified (Figure 1).
Adolescent Descriptions of School-based Diabetes Self-Management With Perceived Allocation of Responsibility for Each Task
Note. Check marks indicate that the item was reported by the majority of participants.
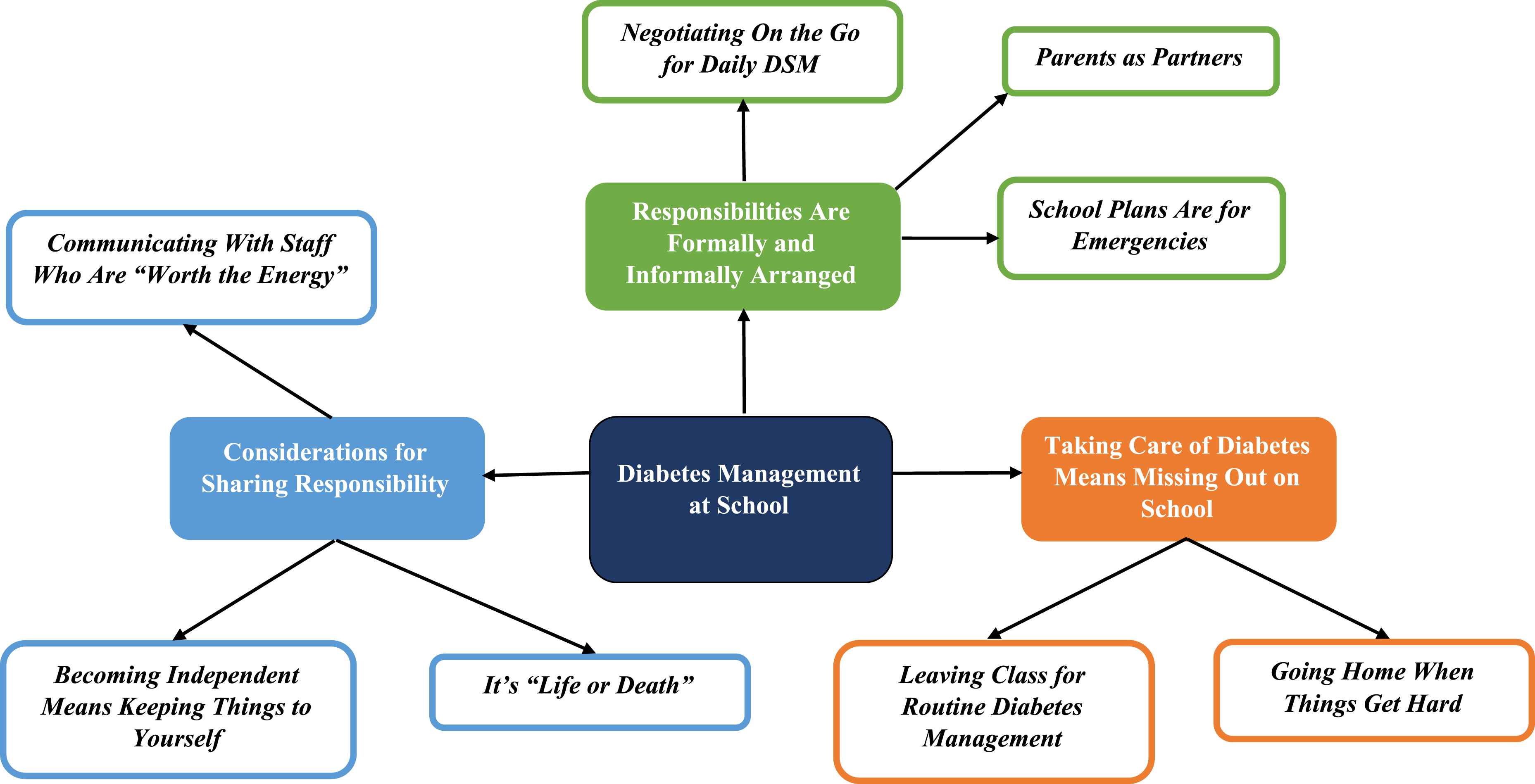
Themes and subthemes.
Theme 1: Responsibilities Are Formally and Informally Arranged
This theme reflects adolescents’ perceptions that responsibilities for school-based DSM were both formally (in the form of school plans) and informally (through communications with parents and school staff) arranged.
Parents as Partners
All adolescents reported needing some help with daily DSM. As Pia explained, “I’ll have a good idea of what I want to do, but I just want to make sure . . . I’m not fully grown. I still make bad choices.” Adolescents referred to their parents as having knowledge that was more advanced than their own: “I don’t really disagree with anything to do with diabetes—[if] Mum says something, that’s usually what it is. Mum is really good at this” (Ted).
Participants described parents as supporting their developing autonomy (e.g., allowing them to make the choice to go home early from school to manage diabetes). They reported that these decisions did not have any clinical oversight and, further, that parents’ sense of anxiety about their DSM with respect to school participation was greater than their own. As Thomas explained, “She was kind of worried, as every mum is.”
Participants generally reported that parents had sole ownership of communication that advanced the school’s understanding of diabetes management: Mum and I, we would chat about some things that we thought would need to happen, and then she would chat to the school. Just because they seemed to keep in contact with parents a little bit better than students. (Sophie)
School Plans Are for Emergencies
Participants who were aware of their school plan described them as risk management tools for school staff that were managed by parents. They reported being uninvolved in the plans’ development and felt teachers were unlikely to use them. As Sophie said, “I think it’s important[,] but at the same time, if it’s not an emergency, it doesn’t do very much.”
Negotiating On the Go for Daily DSM
Participants concurred that responsibility for negotiating daily diabetes-related activities at school was, as Sally expressed, “mostly my job.” In general, they described a habit of not communicating with school staff about their diabetes unless there was a problem. As Sally noted, “I often don’t let the teacher know if [my blood glucose levels are] high—only if I’m really, really sick.” Errant blood sugar readings typically resulted in the adolescent deciding on a course of action and then informing the school staff of that decision: I mean, it’s pretty much self-directed. I can always tell my coach, and they’re usually very nice. They’ll let me have what I need to have in terms of space, testing, and letting me be off [the field] when I’m low. (Liam)
Pia commented that leaving elementary school meant a shift in responsibilities: As soon as I got into secondary school it was more like I told the teachers what I needed to get done. . . . Mum was there in case I needed advice. . . . [The] teachers just went along with it.
Theme 2: Considerations for the Sharing of Responsibility
This theme reflects intentional adolescent management of their own school-based diabetes responsibilities.
It’s “Life or Death”
Adolescents described managing diabetes at school as perilous—with DSM strategies couched in terms such as “life or death.” As Sally explained, “My blood sugars are [my] first priority—you know—to keep me alive.” They chose to share the weight of this responsibility in case they passed out in class. This was reported to affect their mental health: “Like, I’ll just be sitting, right there on my laptop, and then it will just hit me just like, ‘Whoa, I could die from this!’ And then you get really down, and sometimes I get a little panic attack” (Hannah).
Becoming Independent Means Keeping Things to Yourself
Adolescents commonly reported a pressing feeling that as they got older, they needed to become more independent. Emily said, “As you get older, you’ll gradually move out of home and stuff—so you’ve got to be independent.” They took “independence” to mean keeping DSM to themselves. As Thomas explained, “I don’t tell teachers—[because I am] quite independent.” Moreover, they related the amount of communication with others to their degree of independence: “I don’t feel like I need to speak about it as much, unless it’s—I’m not managing it well, but I feel like I’m doing pretty good” (Matt).
Communicating With Staff Who Are “Worth the Energy”
Most participants reported preferring to keep their diabetes private. As Ethan explained, “If it’s an emergency I’ll obviously have to, but I would prefer to do it more low-profile–ish.” Adolescents were pragmatic about seeking support. “Office ladies” (i.e., school administrative staff) were commonly referred to as supporting adolescents’ choices by providing immediate practical assistance, such as supplying food or communicating with parents. As Hannah said, “You kind of figure out who’s going to be the most helpful and who’s not going to be, so you use less energy on the people who aren’t going to help you that much.”
If staff were perceived as controlling, or hostile, adolescents reported avoiding them: I’d have to go to them, deliver my insulin, and they’d have to watch me. . . . [It] feels like a trustworthy barrier or whatever, but I just had to do that; it was advised by the school. I just really didn’t like it. So, I’d rather just keep everything personal, and everything organized by me. (Ethan)
Theme 3: Taking Care of Diabetes Means Missing Out on School
This theme reflects the adolescents’ perspective that the impact of current diabetes care arrangements translated to reduced school participation.
Leaving Class for Routine DSM
Adolescents routinely left class to deal with errant blood glucose readings: I’ll go up to the health center, have some jellybeans and then I’ll sit there for 15 [minutes], and if it’s still low, I’ll just tell the lady what my blood sugars are still and I’ll wait another 15. But if I’m all good, I’ll just go back to class. (Matt)
Prioritizing time out of class influenced learning, as Ted explained: “It sucks because [you’re] missing out on things that you need to know, but it’s important to make sure that you’re taking care of it and not dying. Obviously.” Missed class time reportedly also affected the overall quality of learning, even once back in the classroom: I feel like, when you leave they are talking about a simple topic and then when you come back, you’re just like “What’s going on?” I could be out of class for a half hour or so. . . . It feels like every time you leave something else important is covered. (Hannah)
Going Home When Things Get Hard
It was common practice for adolescents to decide to leave school if problems could not be quickly resolved. “[If] I don’t have spare equipment on me, I would just call my mum and then she would get me picked up and then we’d be able to sort it out at home” (Ethan—reported to have missed 100 days of school last year).
Participants who missed sport practices or camps reported that this was usually decided between themselves and their parents, without support from the school or health care team. Thomas explained, “I think my mum just asked me if I wanted to go, and I just said no. There wasn’t really—you didn’t really need anything—you just needed to hand in a permission note.”
Discussion
These results provide the foundational understanding that, congruent with descriptions of managing T1D in the family context (Farthing et al., 2022), adolescents perceived the management of diabetes at school to be a complex occupation that comprised multiple activities, for which they were largely responsible. Adolescents valued an overarching shared approach to the management of T1D at school, although current practices at times limited their school participation. The sharing of responsibility at school was influenced by the adolescents’ need to manage risk; to be independent; and to obtain timely, practical assistance in the event of errant blood glucose readings.
Arrangement of Responsibility for DSM
Consistent with studies that have examined chronic health management in the family context (Chung et al., 2020 ; Nightingale et al., 2019), arranging responsibility for DSM at school was perceived to occur largely as a function of an interdependent parent–adolescent partnership that was based on regular communication that was highly responsive to difficult situations. This supports the conception of DSM as a co-occupation in the school context with the understanding that sharing communication, emotionality, and intentionality can define co-occupation, even when participants are not physically sharing task performance (Pizur-Barnekow & Pickens, 2019).
Adolescents’ heavy reliance on the parent–adolescent partnership meant daily responsibilities were generally not perceived as shared with the wider team, such that decisions about reducing school participation were often made without clinical or educative oversight (e.g., leaving school early or not attending a camp). Adolescents reported that their parents’ sense of worry about diabetes was greater than their own; this corroborates other qualitative findings that adolescents and parents have unique perceptions regarding diabetes care priorities (Spencer et al., 2013). One cross-sectional study found that substantial dissimilarity between illness perceptions of parents and adolescents with T1D, together with low levels of school support, was associated with poorer quality of life (Almeida et al., 2020), which suggests these are important targets for intervention.
Overall, parents were seen as responsible for organizing formal procedures for diabetes management (e.g., school plans), whereas adolescents arranged support on the go, as needed during the school day. This meant that adolescents did not share responsibility for the final determination of school-based DSM strategies even though they were primarily responsible for the enactment of these strategies at school. This division of responsibilities may not play to adolescents’ cognitive strengths. A literature review found that, compared with adults, adolescents are highly creative and fast thinkers, although their decision-making performance is hampered in emotional contexts (Casey & Caudle, 2013). Herlitz et al. (2016) argued that adolescents are therefore more suited to deliberative, rather than in-the-moment decision-making. This lends support to the importance of including students in formal school planning.
The allocation of responsibility to parents, for the structuring of formal diabetes support, may explain the commonly reported finding that, despite the fact that a formal school plan is generally mandated, many adolescents perceived that they did not have one (McCollum & O’Grady, 2020). Participants who knew of their school plans viewed them as emergency advice for teachers, which is at odds with the broad recommendation that the school plan should be used to clarify stakeholder responsibilities, determine support for psychosocial issues, and manage environmental barriers (Jackson & Albanese-O’Neill, 2016). Clarified team roles and responsibilities have been reported as fundamental to effective sharing of responsibility with adolescents with T1D (Olinder et al., 2011). Although analyses of co-occupation with adolescents are minimally present in the literature, clear roles have been reported as important to the functioning of co-occupation for parents with adult children (Wilburn et al., 2022). This suggests that a school plan could be used more comprehensively to delineate and allocate team responsibilities. Occupational therapists’ skills in occupational analysis would be a valuable contribution to this process in providing clarity around roles and responsibilities and helping with plans that attend to the integration of DSM into daily school routines.
Factors Affecting Adolescents’ Sharing of Their Responsibility
Participants’ sense of DSM at school as a matter of life or death pervaded their decision-making and gave rise to the sharing of responsibility primarily as a means of subverting impending personal danger—which commonly equated to reduced participation at school. Some participants reported heightened anxiety related to this emphasis on risk management in diabetes care. This is important given that a systematic review reported that one-third of adolescents with T1D have elevated levels of diabetes-related distress (Hagger et al., 2016).
A review of 50 years of advancing diabetes management and related outcomes for adolescents with T1D found that treatment emphasis has shifted from avoidance of hypoglycemia to the minimization of glucose variability (Fairchild, 2015). In keeping with this shift, diabetes management strategies may be better focused on support for health-promoting habits rather than the subversion of danger. Occupational therapists’ capacity to analyze task performance and habit formation within the school context would be a valuable addition to a team-based management of diabetes that aims to enable appropriate risk management while optimizing school participation.
The way adolescents participated in the sharing of responsibility appeared to be further underpinned by their pressing need to build independence, which participants understood to mean managing diabetes by themselves. This likely reflects a normative and culturally tied expectation that as an adolescent becomes older, they will increasingly differentiate themselves from their family unit (Casey & Caudle, 2013). A qualitative study of 61 17-year-olds found that adolescents had a sense of running out of time to become proficient at DSM and that this feeling was overwhelming at times (Ladd et al., 2022). In high- and middle-income countries, changing societal dynamics mean that half of all young adults will still live at home until at least age 24, so for many this sense of urgency may be misplaced (Australian Institute of Family Studies, 2023; U.S. Census Bureau, 2023).
Participants reported reducing their communication about DSM was a necessary mark of becoming independent. This reduction in communication as they grew older has also been reported to be a function of shifting familial responsibilities (Tuohy et al., 2023). However, this may not be optimal given that many older adolescents are not meeting their blood glucose targets, which are associated with better health outcomes (Gregory et al., 2022). In addition, older adolescents have been reported to have uniquely elevated mental health symptoms compared with younger adolescents, suggesting an ongoing need for emotional support (Fried et al., 2018). Better DSM is reported when responsibility is shared across the course of adolescence and into emerging adulthood and thus represents an important consideration for school planning (Kelly et al., 2019).
In this study, the participants’ reports of increased independence meant they were less likely to access school services, and they often left school to manage their diabetes at home, thereby affecting their school engagement. A review of factors that influence DSM for late adolescents and emerging adults concurred that instead of focusing on independence, it may be beneficial to support young people to actively regulate the involvement of others (Wiebe et al., 2018). This is consistent with a literature review of shifting responsibilities in families of adolescents who have one or more chronic conditions (e.g., asthma, cystic fibrosis, epilepsy) that concluded there is limited evidence to support independence, or complete responsibility, for self-management as reasonable goals for this population (Nightingale et al., 2019). A qualitative study of 32 parent–adolescent dyads affirmed that aiming for interdependence may better support long-term outcomes for adolescents who are self-managing their diabetes (Farthing et al., 2022). These concerns are echoed by the broader health literature that questions a focus on independence as an end goal for health care, wherein it is understood to mean completing a task on one’s own, because this may function to diminish both autonomy and opportunities for social support (McClure & Leah, 2021).
The results of this research highlight the value these adolescents placed on parental sharing of responsibility. This reinforces the importance of retaining the involvement of parents and adolescents on teams that manage diabetes care for schools and prompts consideration of interdependence as the aim of successful adolescent DSM. The American Occupational Therapy Association (AOTA; 2020) endorses this view of co-occupation as a conceivable endpoint for intervention.
Finally, adolescents’ reports of limiting their sharing of responsibility to staff who were “worth the energy” provided insights into their pragmatic approach to DSM. They valued school staff who had knowledge of diabetes, offered a sense of relatedness, and supported their choices in management. Adolescents’ tendency to keep diabetes management private if they did not perceive a reason to share details reflects developmentally typical growth in autonomy (Datye et al., 2019). This is consistent with the understanding that warm, autonomy-supportive communication best supports adolescents’ sharing of responsibility for DSM (Tuohy et al., 2023). Teachers’ lack of diabetes-related knowledge and communication has been reported to reduce both adolescents’ willingness to share responsibility and teachers’ potential to minimize educational disruption (Almeida et al., 2020). Hence, teachers’ involvement in the development of diabetes management strategies is important.
Impact of Current Processes on School Participation
Participants’ current DSM practices often resulted in reduced school attendance and involvement. They rarely referred to DSM in the context of enabling optimal performance for school activities but instead focused on managing school-based risks. This meant they frequently reported leaving the classroom and/or going home when difficulties with DSM arose. These results are consistent with reports that adolescents with T1D experience restrictions on school engagement (Fried et al., 2018) and miss more school time than their peers (French et al., 2022). Other studies have similarly reported hypoglycemia as often managed by leaving class, a strategy proposed to be inherently unsafe because of the associated incidence of cognitive impairment (Kise et al., 2017).
In general, the arrangement of school-based responsibilities in this study did not reflect current recommendations for a collaborative team-based approach to the negotiation of diabetes care strategies (Lawrence et al., 2022). All stakeholders must be present if school planning is to enable the kind of responsibility-sharing that can support the integration of DSM into daily routines such that adolescents are not unnecessarily excluded from school activities.
Limitations
This study has some limitations. Recruitment was dependent on the diabetes educator’s judgments about the families’ suitability. Parents, as the first contact point, made the initial decision about whether their adolescent should have an opportunity to take part in this study. This approach may have limited the diversity of participants; however, the impact is unknown given that we did not collect comprehensive demographic data for those who consented or declined to participate. In addition, our results reflect adolescents’ perspectives of DSM at school and may not align with views held by other team members (e.g., endocrinologists, diabetes educators, school staff).
Directions for Future Research
Pyatak et al. (2018) reported on the efficacy of an occupational therapy intervention that supports the development of health-promoting habits for emerging adults with T1D. The present study supports the identified need for further investigation of the role of occupational therapists in supporting families with adolescents who have T1D (Thompson et al., 2023). Future research could explore the development of occupationally focused DSM interventions that are scaffolded for adolescent students’ needs as well as new ways to facilitate their improved participation in school-based occupations.
Implications for Occupational Therapy Practice
AOTA’s Practice Guidelines provide sound evidence for family-centered occupational therapy interventions that enable the development of healthy routines for children and youth with chronic health conditions; however, they do not identify specific interventions for T1D (Cahill & Beisbier, 2020). Our investigation illuminates a particular need for school-based interventions for adolescents with T1D. The value of occupational therapy interventions within the school environment, for the development of health-promoting habits, was recently highlighted (Pfirman et al., 2023).
Although government policies commonly equate DSM with autonomous diabetes care (Chung et al., 2020), a focus on independence may be counterproductive in adolescence. This study demonstrates the value of considering school-based adolescent DSM as a co-occupation that aligns with responsibility-sharing, whereby parents and adolescents operate as a responsive, interdependent unit to manage diabetes at school. Provision of occupational therapy services in the school environment could provide a clear analysis of the constituent tasks of DSM that supports effective responsibility-sharing, to enable healthy habit formation and optimal school participation.
Conclusion
The organizing and sharing of responsibility for diabetes management in secondary schools were characterized by fragmented team communication patterns and an overarching focus on risk that resulted in frequent exclusion from school activities. Adolescents valued an interdependent approach to diabetes management at school, which is in keeping with the consideration of DSM as a co-occupation. They were, however, underrepresented in the formal determination of DSM strategies to be used when at school. Effective responsibility-sharing for DSM depends on autonomy-supportive, team-based communication that enables frequent, clear, mutually agreeable task allocation across the course of adolescence (Gardener et al., 2022). The present results underscore the potential benefits to adolescent health and well-being of more regular, team-based delineation and negotiation of responsibilities for DSM at school. Occupational therapists are uniquely situated to support the effective sharing of responsibility through clear occupational analyses and interventions that enable the appropriate integration of the complex occupation of DSM into the adolescent school day. An opportunity exists for the profession to be more broadly represented in the health care team that serves this population.
Footnotes
Appendix: Interview Guide
What has to be done to take care of your diabetes when you are at school? Who takes care of each job? How was that decided? What do you/your parents think about how important it is that each job gets done? How does taking care of diabetes affect your school day? What do you think about the amount of communication about your diabetes that you have with school now, compared to when you were younger?